2. Attitude and Perception of Ruralites Towards Affected HIV AIDS Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Kendrapara District, Odisha)
Migration and Labour Profile of 17 Panchayats of Rajkanika Block (Kendrapara District, Odisha) Shramik Sahayata ‘O’ Soochana Kendra (Gram-Utthan Block Office) Rajkanika INTRODUCTION 1. Brief on the District of Kendrapada: The district of Kendrapara is surrounded by the Bay of Bengal in the east, Cuttack district in the west, Jagatsinghapur district in the south and Jajpur and Bhadrak districts in the north. Towns of the district are Kendrapara (M) (63,678), and Pattamundai (NAC) (19,157). The district has 2.88 lakh of households and the average household size is 5 persons. Permanent houses account for only 14.3 percent, 81.5 percent houses occupied are temporary and 4.2 semi permanent houses. Total number of villages of the district is 1540 of which 1407 villages are inhabited. The district of Kendrapara is one of the new created districts carved out of the old Cuttack district. The district is one of the relatively developed districts particularly in the field of education. The district has a low population growth rate but high population density. The economy of the district is mainly dependent upon cultivation. Out of 100 workers in the district 68 are engaged in agricultural sector. Flood, cyclone and tornado are a regular phenomenon in the district due to its proximity to the coastal belt. Figure 1: Map of Odish with the district and block map of Kendrapara 2. Kendrapara: At a Glance (As per Census 2011) Total Population 1,440,361 Males 717,814 Females 722,547 Number of households 2.88 lakh Household size (per household) 5 Sex ratio (females per 1000 males) 1007 Scheduled Tribe population (Percentage to total population) 0.52 Scheduled Caste population(Percentage to total population) 20.52 Largest SC groups include (major caste group) are Kandra 42.91 Dewar and 13.04 Dhoba etc. -

Livelihoods, Conservation and Forest Rights Act in a National Park: an Oxymoron?
Livelihoods, Conservation and Forest Rights Act in a National Park: An Oxymoron? Subhashree Banerjee Syed Ajmal Pasha ISBN 978-81-7791-245-6 © 2017, Copyright Reserved The Institute for Social and Economic Change, Bangalore Institute for Social and Economic Change (ISEC) is engaged in interdisciplinary research in analytical and applied areas of the social sciences, encompassing diverse aspects of development. ISEC works with central, state and local governments as well as international agencies by undertaking systematic studies of resource potential, identifying factors influencing growth and examining measures for reducing poverty. The thrust areas of research include state and local economic policies, issues relating to sociological and demographic transition, environmental issues and fiscal, administrative and political decentralization and governance. It pursues fruitful contacts with other institutions and scholars devoted to social science research through collaborative research programmes, seminars, etc. The Working Paper Series provides an opportunity for ISEC faculty, visiting fellows and PhD scholars to discuss their ideas and research work before publication and to get feedback from their peer group. Papers selected for publication in the series present empirical analyses and generally deal with wider issues of public policy at a sectoral, regional or national level. These working papers undergo review but typically do not present final research results, and constitute works in progress. Working Paper Series Editor: Marchang Reimeingam LIVELIHOODS, CONSERVATION AND FOREST RIGHTS ACT IN A NATIONAL PARK: AN OXYMORON? Subhashree Banerjee* and Syed Ajmal Pasha† Abstract National Parks in India are highly vulnerable due to excessive pressure on their ecosystems as a result of growing population and high dependency of forest dwellers on these resources. -
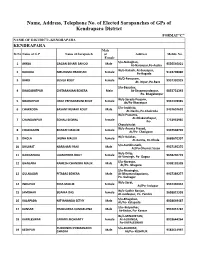
Name, Address, Telephone No. of Elected Sarapanches of Gps Of
Name, Address, Telephone No. of Elected Sarapanches of GPs of Kendrapara District FORMAT"C" NAME OF DISTRICT:-KENDRAPARA KENDRAPARA Male Sl.No Name of G.P Name of Sarapanch or Address Mobile No. Female S/o-Nabaghan, 1 AYABA GAGAN BIHARI SAHOO Male At-Naranpur,Po-Ayaba 9556546021 W/o-Kailash, At-Suryapur, 2 BAGADA NIRUPAMA PRADHAN Female Po-Bagada 9124708080 W/O-Parsuram, 3 BARO SUSILA ROUT Female At- Itipur, Po-Baro 9937392919 S/o-Basudev, 4 BHAGABATPUR CHITARANJAN BEHERA Male At-Shyamsundarpur, 9853731343 Po- Bhagabatpur W/o-Sarada Prasann, 5 BHARATPUR JINAT PRIYADARSINI ROUT Female At/Po-Bharatpur 9937478985 S/o-Arakhita, 6 CHAKRODA BASANT KUMAR ROUT Male At-Narilo, Po-Chakroda 9437607692 W/o-Prasanta, At-Nilakanthapur, 7 CHANDANPUR SONALI BISWAL Female Po- 7751961985 Choudakulat W/o-Ananta Prasad, 8 CHARIGAON BHARATI MALLIK Female At/Po- Charigaon 9937538739 W/o-Kalakar, 9 DHOLA JHUNA MALLIK Female At-Kantia, Po-Dhola 9668670397 S/o-Sambhunath, 10 DHUMAT NARAHARI PANI Male At/Po-Dhumat Sasan 9937195375 W/o-Dillip, 11 GANGAPADA LAXMIPRIYA ROUT Female At-Versingh, Po- Gogua 9658230719 S/o-Narayan, 12 GHAGARA RAMESH CHANDRA MALIK Male At/Po- Ghagara 9938192328 S/o-Nrusingha, 13 GULNAGAR PITABAS BEHERA Male At-Bhramardiapatana, 9937389277 Po- Gulnagar W/o-Sarat, 14 INDUPUR RINA MALLIK Female At/Po- Indupur 9937440044 W/o-Sudhir Ranjan, 15 JAMDHAR SISAMA DAS Female At-Juidaspur, Po- Pandiri 9658821395 S/o-Bhagaban, 16 KALAPADA NITYANANDA SETHY Male At/Po- Kalapada 9938649487 S/o- Bidyadhar, 17 KANSAR PRADUMNA KUMAR JENA Male At-Endar, Po- -

Odisha State Beverages Corporation Ltd ( a G O V E R N M E N T O F O D I S H a U N D E R T a K I N G )
Odisha State Beverages Corporation Ltd ( A G o v e r n m e n t o f O d i s h a U n d e r t a k i n g ) H.O.- 2nd FLOOR, FORTUNE TOWERS,CHANDRASEKHARPUR, BHUBANESWAR-751023 (ODISHA) E-mail : [email protected], Phone : 0674 -2303972 RETAILER INFORMATION Sl Type of District Name Retailer Name Address Shop Details No. Shop C.O, 120 INFANTRY BATTALION 1 ANGUL (TERITORIAL ARMY) BBSR, ANGULCSD EXT COUNTER,ANGUL DEFENCE EXTENSION COUNTER AT ANGUL SATYANANDA DALABEBERA, HOTEL 2 ANGUL DURGA,RAINBROW BRITE TURANGA, HOTEL DURGA,TURANGA,ANGUL ON SHOP HOTEL ANGUL SATYA RANJAN SAMANTA, 3 ANGUL HOTEL ARYA, TURANGA ,ANGUL ON SHOP RESTAURANT TURANGA,ANGUL M/S KALINGA GUEST HOUSE & RESORTS(KAMLESH SATYABRATA SWAIN, HOTEL 4 ANGUL CONTINENTAL), INDUSTRIAL AREA HAKIM ON SHOP HOTEL KAMLESH CONTIINNETAL PADA,ANGUL 5 ANGUL NITAN JAISWAL, DERANGA DERANGA OFF SHOP RAMESH CHANDRA SAHOO & BIJAY 6 ANGUL ANGUL TOWN,ANGUL,Ward No.21,Municipality,Angul OFF SHOP KUMAR SAHOO,ANGUL TOWN NO.I RAMESH CHANDRA SAHOO & BIJAY 7 ANGUL CHHENDIPADA, ANGUL OFF SHOP KUMAR SAHOO, CHHENDIPADA RAMESH CHANDRA SAHOO& BIJAY 8 ANGUL SOUTH BALANDA, ANGUL OFF SHOP KUMAR SAHOO, SOUTHBALANDA RAMESH CHANDRA SAHOO& BIJAY 9 ANGUL KUMAR SAHOO,TALCHER NO-IV( HANDIDHUA,ANGUL OFF SHOP HANDIDHUA) PRABHU KUMAR & SITARAM 10 ANGUL BANTALA ,ANGUL OFF SHOP PRADHAN, BANTALA NO.I RAMESH CHANDRA SAHU & BIJAYA 11 ANGUL AT-BAMUR,P.S-KISHORENAGAR,ANGUL OFF SHOP KUMAR SAHU,BAMUR 12 ANGUL BANSIDHAR DEHURY, NISHA NISHA,ANGUL OFF SHOP 13 ANGUL BANSIDHAR DEHURY, KUMANDA KUMANDA,ANGUL OFF SHOP 14 ANGUL JYOTI RANJAN -

Annual Activities Report Year 2012-2013
Annual Activities Report Year 2012-2013 CHALE CHALO S-3/60, Niladri Vihar, Po- Sailashree Vihar Bhubaneswar – 751021, Dist – Khurda, Odisah, India Ph-0674-2721157, Mob-9439400352 Email- [email protected] Web – www.chalechalo.org.in Page 2 PREFACE The year was dedicated to enormous working on the themes of Education, Empowerment, Environment and Child Rights. Our effort to recreate a luxurious green belt around coastal Kendrapara and ensure its bio-diversity unrestrained flourish is moving at a steady pace. Through community participation, we have planted around 1 lakh mangrove species and 2 lakh general plant species across the 60 operational villages since 2006. The movement has taken on new heights with more people, youth, women and children orienting determinedly towards it. School children are no less enthusiastic, and are cooperating with us in every way through their eco-clubs which we have facilitated for strengthening in all 60 schools in Rajnagar Pattamundai Mahakalpada Aul and Rajkanika Blocks. We have in the meanwhile set up a new MANGRO Center at Rajnagar which would stand out as an excellent resource center of the region inspiring progress of the masses in social, economic and environmental sectors. We are also engaged in intensive empowerment drive targeted at 6000 marginalized families in 60 backward villages of drought-prone KBK region of Odisha. We are assisting them to articulate their genuine problems, demand civil and constitutional rights and constitute legitimate forums to bear on the government collectively for accessing entitlements. We have brought in the community radio technology to strengthen their voice and reach, and it has worked superbly. -

Kendrapara Zone
SHRI JAGANNATH SANSKRIT VISHVAVIDYALAYA, SHRI VIHAR, PURI LIST OF EXAMINERS FOR SHASTRI–IInd YEAR 2018 VALUATION VALUATION CENTRE -ABHAYA AYURVEDA SANSKRIT COLLEGE, AT/PO – NASADIPUR, DIST – KENDRAPARA Date of Valuation: 30.04.2018 onwards SHRI JAGANNATH SANSKRIT VISHVAVIDYALAYA, SHRI VIHAR, PURI LIST OF EXAMINERS FOR SHASTRI–IInd YEAR 2018 VALUATION CENTRE -ABHAYA AYURVEDA SANSKRIT COLLEGE, No. – 1378 (20) Dt- 20.04.2018 AT/PO – NASADIPUR, DIST - KENDRAPARA SUBJECT – M.I.L.(ODIA) Sl. Sl. No. No of Gr. Name of the Examiners List 1. 5 Dr. Gangadhar Samantaray, Bijay Chand Sanskrit College, Samagol, Kujang, Jagatsinghpur. 2. 14 Artatrana Biswal, Ramachandi Sanskrit Moahavidyalaya, Mundalo, Hariank, Danpur, Kendrapara. 3. 15 Malaya Kumar Jena, Sri Sri Ananta Narayan Sanskrit Mohavidyalaya, Ayatpur, Karilopatna, Kendrapara. 4. 18 Pabitra Kumar Swain, Gopinathpur Sanskrit College, Gopinathpur Sasan, Jadupur, Marshaghai, Kendrapara. 5. 19 Laxmi Narayan Dash, Dr. H.K. Mahtab Adar sha Sanskrit Mahavidyalaya, Shankarpur, Cuttack-12. 6. 27 Alok Ranjan Dash, Bagdevi Sanskrit College, Daliji, Chandol, Kendrapara. 7. 28 Kishore Ch. Jena, Tulasi Sanskrit College, Narendrapur, Nembra, Kendrapara. 8. 30 Jayanti Jena, Krushna Chandra Sanskrit Women’s College, At – Bhitarbampu, P.O. – Janarabarimul, Via – Danpur, Dist – Kendrapara, PIN - 754210 9. 33 Sagarika Singh, Bata Baba Sanskrit College, Tunapur, Bagada, Sri Baladevjew, Kendrapara. 10. 42 Somanath Nayak, Barabati Sanskrit College, Barabati, D harmashala, Jajpur. 11. 44 Pramod Kumar Das, Atmaram Sanskrit Mahavidyalaya, Jatadhari Ashram, At - Ramakrishnapur, P.O- Bhera, Via- Mauda, Dist- Cuttack, Pin- 754290 12. 47 Dipti Ranjan Jena, Sidheswar Sanskrit Mahavidyalaya, Siddha Vihar, Gelapur, Baradia, Via-Anakhia, Jagatsinghpur . 13. 48 Bibhuti Nath Sharma, Pravakar Sanskrit Mohavidyalaya, Chandrasekharpur, Ramachandrapur, Jajpur. -

List of Core Banks Available in Orissa
LIST OF CORE BANKS AVAILABLE IN ORISSA DISTRICT BLOCK BANK NAME IFSC ADDRESS ANGUL ANGUL ANDHRA BANK ANDB0000704 SHANKAR CINEMA RAOD, ANGUL - 759122 AXIS BANK LTD UTIB0000288 SREERAM MARKET COMPLEX,P.O.ANGUL,ORISSA - 759122 BANK OF BARODA BARB0ANGULX AMALPARA, NEAR BUS STAND, ANGUL-ORISSA-759122 NANDA BHAVAN, AMALAPADA, 2ND LANE, ANGUL, DIST. :ANGUL BANK OF INDIA BKID0005560 ORISSA - 759 122 CANARA BANK CNRB0002322 NATARAJ BUILDING AMLAPADA , NEAR BUS STAND ANGUL-759122 UMASHANKAR BAZAR, CALTAX CHHAK, TURANG, ANGUL, DIST.- CENTRAL BANK OF INDIA CBIN0283308 ANGUL,ORISSA-759122 PLOT NO. 961/1890 & 1891, I FLOOR, SREERAM MARKET COMPLEX, CORPORATION BANK CORP0001433 ANGUL, ORISSA-759122 DENA BANK BKDN0911196 AMLAPADA 2ND LANE,NH 42,:ANGUL ORISSA-759122 SHANKAR CINEMA ROAD, ANGUL, DIST - ANGUL ANGUL ORISSA HDFC BANK LTD. HDFC0000764 759122 ICICI BANK LTD., FIRST FLOOR, NANDA BHAWAN, ICICI BANK LTD ICIC0000460 AMLAPARA II LINE, ANGUL, ORISSA- 759122 INDIAN BANK IDIB000A136 HARIMAHURI CHHAK MAIN ROAD ANUGUL 759122 INDIAN OVERSEAS BANK IOBA0000966 I FLOOR, TADA BUILDING, ANGUL POST, , ANGUL, PIN : 759122 IOBA0001163 NALCO NAGAR INDUSIND BANK LTD. INDB0000252 GRD FLR + FRT FLR, SANKAR CINEMA ROAD, ANGUL-759122, ORISSA PLOT NO 1606/3202, SHARMA CHHAK, PO TALCHER- 759 100, DIST: INDB0000256 ANGUL, ORISSA ANGUL 1ST FLOOR, PLOT NO. 1270, SHANTI BAZAAR, ANGUL- KARNATAKA BANK LTD KARB0000033 759122,ORISSA ORIENTAL BANK OF COMMERCE ORBC0101239 NANDA BHAWAN MAMALAPADI SECOND LANE ANGUL ORISSA PO- AMLAPADA, 1ST LINE, KANCHAN TALKIES ROAD ANGUL ORISSA PUNJAB -

Valuation of the Bhitarkanika Mangrove Ecosystem for Ecological Security and Sustainable Resource Use
EERC Theme: Wetlands and Biodiversity EERC Working Paper Series: WB-1 Valuation of the Bhitarkanika Mangrove Ecosystem for Ecological Security and Sustainable Resource Use Ruchi Badola and S A Hussain Wildlife Institute of India, Dehradun MOEF IGIDR WORLD BANK Valuation of the Bhitarkanika Mangrove Ecosystem for Ecological Security and Sustainable Resource Use A World Bank Aided India Environmental Management Capacity Building Technical Assistance Project, IGIDR, Mumbai 2003 Valuation of the Bhitarkanika Mangrove Ecosystem for Ecological Security and Sustainable Resource Use A World Bank Aided India Environm ental Management Capacity Building Technical Assistance Pr oject, IGIDR, Mumbai Project Advisor Prof. Jyoti Parekh, IGIDR, Mumbai Principal Investigators Ruchi Badola and S.A. Hussain Remote Sensing and GIS Qamar Qureshi and Nita Shah Research Fellows Hemant K. Sahu, Poonam Prabha Semwal Kalpana Ambastha Shivani Chandola, Anoop K.R. 2003 Citation: Badola, R. & Hussain S.A. (2003) Valuation of the Bhitarkanika Mangrove ecosystem for ecological security and sustainable resource use. Study Report. Wildlife Institute of India. Dehra Dun. 101 pp. Photo credits: Cover Page (from top) Mangrove forest (Rhizophora mucronata) Poonam P. Semwal The living fossil, Horseshoe crab (Limulus polyphemus) Bivash Pandav Crimson rose butterfly (Pachliopta hector) Gopi Sundar Olive Ridley turtle (Lepidochelys olivacea) Bivash Pandav Estuarine crocodile (Crocodilus porosus) P.O.Nameer King cobra (Ophiophagus hannah) Bivash Pandav Grey heron (Ardea -

Appointment Order of 365 Medical Officers
GOVERNMENT OF ODISHA HEALTH & FAMILY WELFARE DEPARTMENT ***** NOTIFICATION File No. HFW-MSI-ESTT-0099-2019 - 8723/H. Dated 21.03.2020 On the recommendation of the Odisha Public Service Commission, Cuttack vide their letter No- 696/PSC, dated-28.01.2020, 365 (Three Hundred Sixty Five) number of candidates are hereby appointed as Assistant Surgeons in the rank of Group-'A' (Junior) of Odisha Medical & Health Services Cadre under Health and Family Welfare Department and posted in the places as mentioned against each in the scale of pay of Rs.56,100/-(as per 7th Pay Commission) and other allowances as admissible and sanctioned by the Government from time to time. 1. The appointment is purely temporary and terminable at any time without prior notice and without assigning any reason thereof. The appointment is subject to the final outcome of the Writ Petition bearing No. W.P. (C) No. 47, 48 & 49 of 2020 and any other similar type of order passed by the Hon'ble High Court of Odisha. 2. The appointments are subject to their medical fitness to be determined by the Medical Board and their characters, antecedents are found to be satisfactory after verification. In case, adverse reports are received, the services of the candidates concerned would be terminated forthwith. 3. As reported by the Odisha Public Service Commission, the following Fifteen (15) candidates bearing following Roll Nos have not passed Odia up to M.E. School Standard. Roll Nos. 100061, 100076, 100134, 100148, 100156,100274, 100379, 100420, 100485, 100504, 100518, 100531, 100565, 100600, 100615, 100624, 100761, 100824, 100845, 100848, 100854, 100899, 100912, 100933, 100958, 100968, 101032, 101091, 101108, 101121, 101276, 101301, 101320, 101329, 101479, 101524, 101531, 101582, 101605, 101622, 101702, 101706 & 101717 = 43 Candidates As per the Rule 7(v) of Odisha Medical &Health Services (Method of Recruitment and Conditions of Service) Rules, 2017, they shall be allowed to pass the said examination conducted by Board of Secondary Education. -

KENDRAPARA.Pdf
1 2 3 Chapter CONTENTS Page No. Number 1 Introduction 8 1.1 District Profile 8 1.2 Demography 10 1.3 Biomass and Livestock 12 1.4 Agro-Ecology, Climate, Hydrology and Topography 12 1.5 Soil Profile 13 1.6 Soil Erosion and Runoff Status 15 1.7 Land Use Pattern 15 1.8 District Irrigation Plan 23 2 District Water Profile 26 2.1 Area Wise, Crop Wise Irrigation Status 27 2.2 Production and Productivity of Major Crops 28 2.3 Irrigation Based Classification 41 3 Water Availability 42 3.1 Status of Water Availability 43 3.2 Status of Ground Water Availability 54 3.3 Status of Command Area 54 3.4 Existing Type of Irrigation 55 4 Water Requirement / Demand 67 4.1 Domestic Water Demand 68 4 4.2 Crop Water Demand 69 4.3 Livestock Water Demand 71 4.4 Industrial Water Demand 72 4.5 Water Demand for Power Generation 72 4.6 Total Water Demand of the District for Various Sectors 72 4.7 Water Budget 73 5 Strategic Action Plan for Irrigation in district under PMKSY 75 5 List of Tables Table No. Details Page No. Table 1.1 General Profile of Kendrapara District 8 Table 1.2 Demography 11 Table 1.3 Biomass and Live stock 12 Table 1.4 Agro-Ecology, Climate, Hydrology and 14 Topography Table 1.5 Soil Profile 16 Table 1.7 Land Use Pattern of Kendrapara 18 Area-wise, Crop-wise Irrigation Status Table 2.1 29 (Kendrapara Dist.) Table 2.1 (a) Area-wise, Crop-wise Irrigation Status (Block wise) 30 Production and Productivity of Major Crops Table 2.2. -

District Statistical Hand Book, Kendrapara
GOVERNMENT OF ODISHA DISTRICT STATISTICAL HAND BOOK KENDRAPARA 2018 DIRECTORATE OF ECONOMICS AND STATISTICS, ODISHA ARTHANITI ‘O’ PARISANKHYAN BHAWAN HEADS OF DEPARTMENT CAMPUS, BHUBANESWAR PIN-751001 Email : [email protected]/[email protected] Website : desorissa.nic.in [Price : Rs.25.00] ସଙ୍କର୍ଷଣ ସାହୁ, ଭା.ପ.ସେ ଅର୍ଥନୀତି ଓ ପରିସଂ孍ୟାନ ଭବନ ନିସଦେଶକ Arthaniti ‘O’ Parisankhyan Bhawan ଅର୍େନୀତି ଓ ପରିେଂଖ୍ୟାନ HOD Campus, Unit-V Sankarsana Sahoo, ISS Bhubaneswar -751005, Odisha Director Phone : 0674 -2391295 Economics & Statistics e-mail : [email protected] Foreword I am very glad to know that the Publication Division of Directorate of Economics & Statistics (DES) has brought out District Statistical Hand Book-2018. This book contains key statistical data on various socio-economic aspects of the District and will help as a reference book for the Policy Planners, Administrators, Researchers and Academicians. The present issue has been enriched with inclusions like various health programmes, activities of the SHGs, programmes under ICDS and employment generated under MGNREGS in different blocks of the District. I would like to express my thanks to Dr. Bijaya Bhusan Nanda, Joint Director, DE&S, Bhubaneswar for his valuable inputs and express my thanks to the officers and staff of Publication Division of DES for their efforts in bringing out this publication. I also express my thanks to the Deputy Director (P&S) and his staff of DPMU, Kendrapara for their tireless efforts in compilation of this valuable Hand Book for the District. Bhubaneswar (S. Sahoo) May, 2020 Dr. Bijaya Bhusan Nanda, O.S. & E.S.(I) Joint Director Directorate of Economics & Statistics Odisha, Bhubaneswar Preface The District Statistical Hand Book, Kendrapara’ 2018 is a step forward for evidence based planning with compilation of sub-district level information. -

Kendrapara.Pdf
LIST OF MAJOR HEALTH INSTITUTIONS S.No BLOCK NAC PLACE HEALTH UNIT NAME 1 Kendrapada Mty DHH Kendrapara DHH ,Kendrapara 2 Rajakanika AH Olava AH ,RN Rath Hospital,Olava 3 Aul UGPHC Aul UGPHC ,Aul 4 Derabis CHC Derabis CHC ,Derabis 5 Garadpur UGPHC Patkura UGPHC ,Patkura 6 Kendrapada CHC Indupur CHC ,Indupur 7 Mahakalpada CHC Mahakalpada CHC ,Mahakalpada 8 Marsaghai CHC Marsaghai CHC ,Marsaghai 9 Pattamundai UGPHC Pattamundai UGPHC ,Pattamundai 10 Rajakanika CHC Rajakanika CHC ,Rajakanika 11 Rajnagar CHC Rajnagar CHC ,Rajnagar 12 Aul PHC(New) Dasipur PHC(New) ,Dasipur 13 Aul PHC(New) Mahu PHC(New) ,Mahu 14 Aul PHC(New) Batipara PHC(New) ,Batipara 15 Aul PHC(New) Govindpur PHC(New) ,Govindpur 16 Aul PHC(New) Sanamanga PHC(New) ,Sanamanga 17 Aul PHC(New) Palimi PHC(New) ,Palimi 18 Derabis PHC(New) Biranilakanthapur PHC(New) ,Biranilakanthapur 19 Derabis PHC(New) Chandol PHC(New) ,Chandol 20 Derabis PHC(New) Danpur PHC(New) ,Danpur 21 Derabis PHC(New) Mundala-Harianka PHC(New) ,Mundala-Harianka 22 Derabis PHC(New) Santhapura PHC(New) ,Santhapura 23 Garadpur PHC(New) Korua PHC(New) ,Korua 24 Garadpur PHC(New) Madhusasan PHC(New) ,Madhusasan 25 Garadpur PHC(New) Tendakura PHC(New) ,Tendakura 26 Kendrapada PHC(New) Bhagabatpur(Balia) PHC(New) ,Bhagabatpur(Balia) 27 Kendrapada PHC(New) Kalapada PHC(New) ,Kalapada 28 Kendrapada PHC(New) Ayaba PHC(New) ,Ayaba 29 Kendrapada PHC(New) Chandanpur PHC(New) ,Chandanpur 30 Mahakalpada PHC(New) Ramnagar PHC(New) ,Ramnagar 31 Mahakalpada PHC(New) Bijayanagar PHC(New) ,Bijayanagar 32 Mahakalpada PHC(New)