Breathing Exercises
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hypothermia Brochure
Visit these websites for more water safety and hypothermia prevention in- formation. What is East Pierce Fire & Rescue Hypothermia? www.eastpiercefire.org Hypothermia means “low temperature”. Washington State Drowning When your body is exposed to cold tem- Prevention Coalition Hypothermia www.drowning-prevention.org perature, it tries to protect itself by keeping a normal body temperature of 98.6°F. It Children’s Hospital & tries to reduce heat loss by shivering and Regional Medical Center In Our Lakes moving blood from your arms and legs to www.seattlechildrens.org the core of your body—head, chest and and Rivers abdomen. Hypothermia Prevention, Recognition and Treatment www.hypothermia.org Stages of Hypothermia Boat Washington Mild Hypothermia www.boatwashington.org (Core body temperature of 98.6°— 93.2°F) Symptoms: Shivering; altered judg- ment; numbness; clumsiness; loss of Boat U.S. Foundation dexterity; pain from cold; and fast www.boatus.com breathing. Boat Safe Moderate Hypothermia www.boatsafe.com (Core body temperature of 93.2°—86°F) Symptoms: Semiconscious to uncon- scious; shivering reduced or absent; lips are blue; slurred speech; rigid n in muscles; appears drunk; slow Eve breathing; and feeling of warmth can occur. mer! Headquarters Station Sum Severe Hypothermia 18421 Old Buckley Hwy (Core body temperature below 86°F) Bonney Lake, WA 98391 Symptoms: Coma; heart stops; and clinical death. Phone: 253-863-1800 Fax: 253-863-1848 Email: [email protected] Know the water. Know your limits. Wear a life vest. By choosing to swim in colder water you Waters in Western Common Misconceptions Washington reduce your survival time. -

The Hazards of Nitrogen Asphyxiation US Chemical Safety and Hazard Investigation Board
The Hazards of Nitrogen Asphyxiation US Chemical Safety and Hazard Investigation Board Introduction • Nitrogen makes up 78% of the air we breath; because of this it is often assumed that nitrogen is not hazardous. • However, nitrogen is safe to breath only if it is mixed with an appropriate amount of oxygen. • Additional nitrogen (lower oxygen) cannot be detected by the sense of smell. Introduction • Nitrogen is used commercially as an inerting agent to keep material free of contaminants (including oxygen) that may corrode equipment, present a fire hazard, or be toxic. • A lower oxygen concentration (e.g., caused by an increased amount of nitrogen) can have a range of effects on the human body and can be fatal if if falls below 10% Effects of Oxygen Deficiency on the Human Body Atmospheric Oxygen Concentration (%) Possible Results 20.9 Normal 19.0 Some unnoticeable adverse physiological effects 16.0 Increased pulse and breathing rate, impaired thinking and attention, reduced coordination 14.0 Abnormal fatigue upon exertion, emotional upset, faulty coordination, poor judgment 12.5 Very poor judgment and coordination, impaired respiration that may cause permanent heart damage, nausea, and vomiting <10 Inability to move, loss of consciousness, convulsions, death Source: Compressed Gas Association, 2001 Statistics on Incidents CSB reviewed cases of nitrogen asphyxiation that occurred in the US between 1992 and 2002 and determined the following: • 85 incidents of nitrogen asphyxiation resulted in 80 deaths and 50 injuries. • The majority of -

Respiratory Physiology - Part B Experimental Determination of Anatomical Dead Space Value (Human 9 - Version Sept
Comp. Vert. Physiology- BI 244 Respiratory Physiology - Part B Experimental Determination of Anatomical Dead Space Value (Human 9 - Version Sept. 10, 2013) [This version has been modified to also serve as a tutorial in how to run HUMAN's artificial organs] Part of the respiratory physiology computer simulation work for this week allows you to obtain a hand-on feeling for the effects of anatomical dead space on alveolar ventilation. The functional importance of dead space can explored via employing HUMAN's artificial respirator to vary the respiration rate and tidal volume. DEAD SPACE DETERMINATION Introduction The lack of unidirectional respiratory medium flow in non-avian air ventilators creates the existence of an anatomical dead space. The anatomical dead space of an air ventilator is a fixed volume not normally under physiological control. However, the relative importance of dead space is adjustable by appropriate respiratory maneuvers. For example, recall the use by panting animals of their dead space to reduce a potentially harmful respiratory alkalosis while hyperventilating. In general, for any given level of lung ventilation, the fraction of the tidal volume attributed to dead space will affect the resulting level of alveolar ventilation, and therefore the efficiency (in terms of gas exchange) of that ventilation. [You should, of course, refresh your knowledge of total lung ventilation, tidal volume alveolar ventilation.] Your objective here is to observe the effects of a constant "unknown" dead space on resulting alveolar ventilation by respiring the model at a variety of tidal volume-frequency combinations. You are then asked to calculate the functional dead space based on the data you collect. -

Clinical Management of Severe Acute Respiratory Infections When Novel Coronavirus Is Suspected: What to Do and What Not to Do
INTERIM GUIDANCE DOCUMENT Clinical management of severe acute respiratory infections when novel coronavirus is suspected: What to do and what not to do Introduction 2 Section 1. Early recognition and management 3 Section 2. Management of severe respiratory distress, hypoxemia and ARDS 6 Section 3. Management of septic shock 8 Section 4. Prevention of complications 9 References 10 Acknowledgements 12 Introduction The emergence of novel coronavirus in 2012 (see http://www.who.int/csr/disease/coronavirus_infections/en/index. html for the latest updates) has presented challenges for clinical management. Pneumonia has been the most common clinical presentation; five patients developed Acute Respira- tory Distress Syndrome (ARDS). Renal failure, pericarditis and disseminated intravascular coagulation (DIC) have also occurred. Our knowledge of the clinical features of coronavirus infection is limited and no virus-specific preven- tion or treatment (e.g. vaccine or antiviral drugs) is available. Thus, this interim guidance document aims to help clinicians with supportive management of patients who have acute respiratory failure and septic shock as a consequence of severe infection. Because other complications have been seen (renal failure, pericarditis, DIC, as above) clinicians should monitor for the development of these and other complications of severe infection and treat them according to local management guidelines. As all confirmed cases reported to date have occurred in adults, this document focuses on the care of adolescents and adults. Paediatric considerations will be added later. This document will be updated as more information becomes available and after the revised Surviving Sepsis Campaign Guidelines are published later this year (1). This document is for clinicians taking care of critically ill patients with severe acute respiratory infec- tion (SARI). -
QUESTIONS ABOUT YOUR BREATHING Name:______Please Answer the Questions Below for ONLY the PATIENT Seeing the Doctor Today, Date of Birth:______You OR Your Child
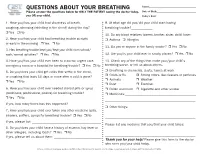
QUESTIONS ABOUT YOUR BREATHING Name:_____________________________________ Please answer the questions below for ONLY THE PATIENT seeing the doctor today, Date of Birth:_______________________________ you OR your child. Today’s Date:_______________________________ 1. Have you/has your child had shortness of breath, 9. At what age did you/did your child start having coughing, wheezing (whistling in the chest) during the day? breathing trouble?_____________ r Yes r No 10. Do any blood relatives (parent, brother, sister, child) have: 2. Have you/has your child had breathing trouble at night r Asthma r Allergies or early in the morning r Yes r No 11. Do you or anyone in the family smoke? r Yes r No 3. Has breathing trouble kept you/kept your child from school/ work/normal activities? r Yes r No 12. Are you/is your child ever in smoky places? r Yes r No 4. Have you/has your child ever been to a doctor, urgent care, 13. Check any of the things that make your/your child’s emergency room or a hospital for breathing trouble? r Yes r No breathing worse, or tell us about others. 5. Do you/does your child get colds that settle in the chest, r Breathing in chemicals, dusts, fumes at work r Colds or flu r Strong odors, like cleaners or perfumes or coughing that lasts 10 days or more after a cold is gone? r Animals r Weather r Yes r No r Dust r Exercise 6. Have you/has your child ever needed steroid pills or syrup r Pollen and mold r Cigarette and other smoke (prednisone, prednisolone, prelone) for breathing trouble? r Medicines:___________________________________________ r Yes r No _______________________________________________________ If yes, how many times has this happened? ___________________ r Other things: 7. -

Brownie's THIRD LUNG
BrMARINEownie GROUP’s Owner’s Manual Variable Speed Hand Carry Hookah Diving System ADVENTURE IS ALWAYS ON THE LINE! VSHCDC Systems This manual is also available online 3001 NW 25th Avenue, Pompano Beach, FL 33069 USA Ph +1.954.462.5570 Fx +1.954.462.6115 www.BrowniesMarineGroup.com CONGRATULATIONS ON YOUR PURCHASE OF A BROWNIE’S SYSTEM You now have in your possession the finest, most reliable, surface supplied breathing air system available. The operation is designed with your safety and convenience in mind, and by carefully reading this brief manual you can be assured of many hours of trouble-free enjoyment. READ ALL SAFETY RULES AND OPERATING INSTRUCTIONS CONTAINED IN THIS MANUAL AND FOLLOW THEM WITH EACH USE OF THIS PRODUCT. MANUAL SAFETY NOTICES Important instructions concerning the endangerment of personnel, technical safety or operator safety will be specially emphasized in this manual by placing the information in the following types of safety notices. DANGER DANGER INDICATES AN IMMINENTLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, WILL RESULT IN DEATH OR SERIOUS INJURY. THIS IS LIMITED TO THE MOST EXTREME SITUATIONS. WARNING WARNING INDICATES A POTENTIALLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, COULD RESULT IN DEATH OR INJURY. CAUTION CAUTION INDICATES A POTENTIALLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, MAY RESULT IN MINOR OR MODERATE INJURY. IT MAY ALSO BE USED TO ALERT AGAINST UNSAFE PRACTICES. NOTE NOTE ADVISE OF TECHNICAL REQUIREMENTS THAT REQUIRE PARTICULAR ATTENTION BY THE OPERATOR OR THE MAINTENANCE TECHNICIAN FOR PROPER MAINTENANCE AND UTILIZATION OF THE EQUIPMENT. REGISTER YOUR PRODUCT ONLINE Go to www.BrowniesMarineGroup.com to register your product. -

What Are the Health Effects from Exposure to Carbon Monoxide?
CO Lesson 2 CARBON MONOXIDE: LESSON TWO What are the Health Effects from Exposure to Carbon Monoxide? LESSON SUMMARY Carbon monoxide (CO) is an odorless, tasteless, colorless and nonirritating Grade Level: 9 – 12 gas that is impossible to detect by an exposed person. CO is produced by the Subject(s) Addressed: incomplete combustion of carbon-based fuels, including gas, wood, oil and Science, Biology coal. Exposure to CO is the leading cause of fatal poisonings in the United Class Time: 1 Period States and many other countries. When inhaled, CO is readily absorbed from the lungs into the bloodstream, where it binds tightly to hemoglobin in the Inquiry Category: Guided place of oxygen. CORE UNDERSTANDING/OBJECTIVES By the end of this lesson, students will have a basic understanding of the physiological mechanisms underlying CO toxicity. For specific learning and standards addressed, please see pages 30 and 31. MATERIALS INCORPORATION OF TECHNOLOGY Computer and/or projector with video capabilities INDIAN EDUCATION FOR ALL Fires utilizing carbon-based fuels, such as wood, produce carbon monoxide as a dangerous byproduct when the combustion is incomplete. Fire was important for the survival of early Native American tribes. The traditional teepees were well designed with sophisticated airflow patterns, enabling fires to be contained within the shelter while minimizing carbon monoxide exposure. However, fire was used for purposes other than just heat and cooking. According to the historian Henry Lewis, Native Americans used fire to aid in hunting, crop management, insect collection, warfare and many other activities. Today, fire is used to heat rocks used in sweat lodges. -
Breathing Air Quality, Sampling and Testing
Breathing Air Quality, Sampling and Testing Environmental Health Laboratory Department of Environmental and Occupational Health Sciences School of Public Health University of Washington Funding and support from The State of Washington Department of Labor & Industries Safety & Health Investment Projects Medical Aid and Accident Fund Breathing Air Quality, Sampling, and Testing Environmental Health Laboratory Department of Environmental and Occupational Health Sciences School of Public Health University of Washington Funding and support from The State of Washington Department of Labor & Industries Safety & Health Investment Projects Medical Aid and Accident Funds 1 University of Washington Environmental Health Laboratory Table of Contents Overview ...............................................................................1 Background ...........................................................................2 Regulated Components of Breathing Air ...............................7 Performance of Breathing Air Testing Kits ............................9 Laboratory Accreditation .....................................................18 Guidance Summary .............................................................19 Glossary ..............................................................................20 References ...........................................................................22 List of Tables Table 1. Breathing Air Quality Specifications ........................2 Table 2. Description of Kits Tested ........................................9 -

Diving Air Compressor - Wikipedia, the Free Encyclopedia Diving Air Compressor from Wikipedia, the Free Encyclopedia
2/8/2014 Diving air compressor - Wikipedia, the free encyclopedia Diving air compressor From Wikipedia, the free encyclopedia A diving air compressor is a gas compressor that can provide breathing air directly to a surface-supplied diver, or fill diving cylinders with high-pressure air pure enough to be used as a breathing gas. A low pressure diving air compressor usually has a delivery pressure of up to 30 bar, which is regulated to suit the depth of the dive. A high pressure diving compressor has a delivery pressure which is usually over 150 bar, and is commonly between 200 and 300 bar. The pressure is limited by an overpressure valve which may be adjustable. A small stationary high pressure diving air compressor installation Contents 1 Machinery 2 Air purity 3 Pressure 4 Filling heat 5 The bank 6 Gas blending 7 References 8 External links A small scuba filling and blending station supplied by a compressor and Machinery storage bank Diving compressors are generally three- or four-stage-reciprocating air compressors that are lubricated with a high-grade mineral or synthetic compressor oil free of toxic additives (a few use ceramic-lined cylinders with O-rings, not piston rings, requiring no lubrication). Oil-lubricated compressors must only use lubricants specified by the compressor's manufacturer. Special filters are used to clean the air of any residual oil and water(see "Air purity"). Smaller compressors are often splash lubricated - the oil is splashed around in the crankcase by the impact of the crankshaft and connecting A low pressure breathing air rods - but larger compressors are likely to have a pressurized lubrication compressor used for surface supplied using an oil pump which supplies the oil to critical areas through pipes diving at the surface control point and passages in the castings. -

The Future of Mechanical Ventilation: Lessons from the Present and the Past Luciano Gattinoni1*, John J
Gattinoni et al. Critical Care (2017) 21:183 DOI 10.1186/s13054-017-1750-x REVIEW Open Access The future of mechanical ventilation: lessons from the present and the past Luciano Gattinoni1*, John J. Marini2, Francesca Collino1, Giorgia Maiolo1, Francesca Rapetti1, Tommaso Tonetti1, Francesco Vasques1 and Michael Quintel1 Abstract The adverse effects of mechanical ventilation in acute respiratory distress syndrome (ARDS) arise from two main causes: unphysiological increases of transpulmonary pressure and unphysiological increases/decreases of pleural pressure during positive or negative pressure ventilation. The transpulmonary pressure-related side effects primarily account for ventilator-induced lung injury (VILI) while the pleural pressure-related side effects primarily account for hemodynamic alterations. The changes of transpulmonary pressure and pleural pressure resulting from a given applied driving pressure depend on the relative elastances of the lung and chest wall. The term ‘volutrauma’ should refer to excessive strain, while ‘barotrauma’ should refer to excessive stress. Strains exceeding 1.5, corresponding to a stress above ~20 cmH2O in humans, are severely damaging in experimental animals. Apart from high tidal volumes and high transpulmonary pressures, the respiratory rate and inspiratory flow may also play roles in the genesis of VILI. We do not know which fraction of mortality is attributable to VILI with ventilation comparable to that reported in recent clinical practice surveys (tidal volume ~7.5 ml/kg, positive end-expiratory pressure (PEEP) ~8 cmH2O, rate ~20 bpm, associated mortality ~35%). Therefore, a more complete and individually personalized understanding of ARDS lung mechanics and its interaction with the ventilator is needed to improve future care. -

PHYSIOLOGY of RESPIRATION Respiration Includes 2 Processes: 1) External Respiration – Is the Uptake of O 2 and Excretion Of
PHYSIOLOGY OF RESPIRATION Respiration includes 2 processes: 1) External respiration – is the uptake of O 2 and excretion of CO 2 in the lungs 2) Internal respiration – means the O 2 and CO 2 exchange between the cells and capillary blood The quality of these respiration processes depends on: a) pulmonary ventilation – it means the inflow and outflow of air between the atmosphere and the lung alveoli b) diffusion of oxygen and CO 2 between the alveoli and the blood c) perfusion – of lungs with blood d) transport of O 2 and CO 2 in the blood e) regulation of respiration Nonrespiratory functions: - in voice production - protective reflexes (apnoea, laryngospasm) - defensive reflexes (cough, sneeze) - in thermoregulation STRUCTURE OF THE RESPIRATORY TRACT Upper airways - nose,nasopharynynx - borderline - larynx Lower airways - trachea, bronchi, bronchioles. The airways divide 23 times to 23 generations between the trachea and: Alveoli - 300 milion - total surface area 70 m 2 lined pneumocytes - type I -flat cells - type II - producers of the surfactant - lymphocytes, plasma cells, alveolar macrophages, mast cells.... Innervation : Smooth muscles innervated by autonomic nervous system: - parasympathetic - muscarinic - bronchoconstriction - sympathetic - beta 2 - receptors – bronchodilation - mainly to adrenalin - noncholinergic nonadrenergic innervation - VIP MECHANICS OF VENTILATION Inspiration - an active process - contraction of the inspiratory muscles: - Diaphragm - accounts for 60-75% of the tidal volume - External intercostal muscles - Auxiliary -accessory-inspiratory muscles: Scalene and sternocleidomasoid m.m. Expiration - quiet breathing - passive process - given by elasticity of the chest and lungs - forced expirium - active process – expiratory muscles: - Internal intercostal m.m. - Muscles of the anterior abdominal wall Innervation: Motoneurons: Diaphragm – n.n. -

Effect of Dead Space on Breathing Stability at Exercise in Hypoxia Eric Hermand, François Lhuissier, Jean-Paul Richalet
Effect of dead space on breathing stability at exercise in hypoxia Eric Hermand, François Lhuissier, Jean-Paul Richalet To cite this version: Eric Hermand, François Lhuissier, Jean-Paul Richalet. Effect of dead space on breathing sta- bility at exercise in hypoxia. Respiratory Physiology & Neurobiology, 2017, 246, pp.26-32. 10.1016/j.resp.2017.07.008. hal-03189523 HAL Id: hal-03189523 https://hal.archives-ouvertes.fr/hal-03189523 Submitted on 3 Apr 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. 1 Effect of dead space on breathing stability at exercise in hypoxia. 2 3 Eric Hermand1, François J Lhuissier1,2, Jean-Paul Richalet1 4 5 1Université Paris 13, Sorbonne Paris Cité, Laboratoire “Hypoxie et poumon”, EA2363, 6 Bobigny, France 7 2Assistance Publique-Hôpitaux de Paris, Hôpital Avicenne, Service de Physiologie, 8 explorations fonctionnelles et médecine du sport, 93009 Bobigny, France 9 10 11 Corresponding author [email protected] (J.P. Richalet) [email protected] (E. Hermand) 12 13 Laboratoire “Hypoxie & poumon”, EA2363 14 74 rue Marcel Cachin 15 93017 Bobigny Cedex, FRANCE 16 Tel: +33148387758 / Fax: +33148388924 17 18 19 Word count for manuscript: 2946 20 21 22 Key words: Control of ventilation, hypoxia, exercise, periodic breathing, breathing 23 instability, dead space, alveolar ventilation 24 25 26 27 28 29 30 Abstract 31 Recent studies have shown that normal subjects exhibit periodic breathing when submitted to 32 concomitant environmental (hypoxia) and physiological (exercise) stresses.