3D Lingual Treatment with Suresmile and Tads Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular Tads by Randy J
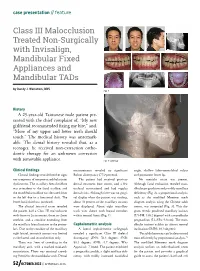
case presentation // feature Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular TADs by Randy J. Weinstein, DDS Fig. 1 History A 25-year-old Taiwanese male patient pre- sented with the chief complaint of, “My new girlfriend recommended fixing my bite,” and, “More of my upper and lower teeth should touch.” The medical history was unremark- able. The dental history revealed that, as a teenager, he received non-extraction ortho- dontic therapy for an unknown correction with removable appliance. Fig. 2: Overlay Clinical findings measurements revealed no significant angle, shallow labio-mentolabial sulcus Clinical findings revealed neither signs Bolton discrepancy (77.9 percent). and prominent lower lip. nor symptoms of temporomandibular joint The patient had received previous No mentalis strain was present. dysfunction. The maxillary dental midline dental treatment (one crown, and a few Although facial evaluation revealed man- was coincident to the facial midline, and occlusal restorations) and had regular dibular prognathism and possibly maxillary the mandibular midline was deviated 2mm dental visits. Although there was no gingi- deficiency (Fig. 2), a proportional analysis, to the left due to a functional shift. The val display when the patient was smiling, such as the modified Moorrees mesh lower facial third was increased. about 70 percent of the maxillary incisors diagram analysis using the Chinese adult The clinical intraoral exam revealed were displayed. About eight maxillary norms, was computed (Fig. 3). This dia- the patient had a Class III malocclusion teeth were shown with buccal corridors gram reveals proclined maxillary incisors with 0mm to 2mm overjet, 0mm to -2mm within normal limits (Fig. -
What's in YOUR Clinical Bag of Tricks? Page 12 Self-Ligating Brackets
The Biggest Risk is the One You Can Manage by Dr. Donald E. Machen, page 43 October 2011 – Volume 4, Issue 8 Message Board What’s in YOUR Clinical Bag of Tricks? page 12 Focus On Self-ligating Brackets page 49 Publications Mail Agreement No. 40902037 A Division of Farran Media, LLC www.orthotown.com Finally. A system that puts control back in your hands. It’s Your Choice: Fully Interactive or Dual Activation System Interactive Anteriors and Passive Posteriors s-ULTIPLEPRESCRIPTIONOPTIONS s(OOKOPTIONAVAILABLEONALL posterior teeth and laterals s4HREEBICUSPIDPADOPTIONS sEmpower SL molars available soon MADE IN THEHE USAUSA www.empowerbraces.com contents October 2011 43 From right: Paul Humphrey, president; Doug Hurford, corporate controller; Sandy McPherson, office manager; and Karri Denny, marketing coordinator. 34 4949 Photograph by John Fedele Articles Advansync, Anyone? 30 Herbst and Advansync each have a following. Have you ever considered switching? The Biggest Risk is One You Can Manage Dr. Donald E. Machen discusses the importance of developing 43 Which Bands (Company)? a strategic plan as well as a regular and frequent protocol With so many to choose from, docs discuss what bands they for review of your personal financial investments with your 33 use and why. investment adviser. Orthodontists Are Finding “There’s an App for That” 46 Angela Weber explores the benefits and current opportunities In This Issue of mobile phone apps for your practice’s Web site. The Truth About Self-ligating Brackets On Orthotown.com 49 Orthotown Magazine surveyed several orthodontic companies, 4 asking all about their self-ligating bracket systems, making it easier than ever to find the system right for you. -

An Overview on Interproximal Enamel Reduction
DENTISTRY ISSN 2377-1623 http://dx.doi.org/10.17140/DOJ-1-104 Open Journal Review An Overview on Interproximal Enamel *Corresponding author Reduction Yanqi Yang Assistant Professor in Orthodontics Faculty of Dentistry, the University of Deborah Chee#, Chong Ren# and Yanqi Yang* Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying #equally contributed Pun, Hong Kong, China Tel. +852-28590252 Orthodontics, Faculty of Dentistry, the University of Hong Kong, 34 Hospital Road, Hong Kong Fax: +852-25593803 SAR, China E-mail: [email protected] Volume 1 : Issue 1 ABSTRACT Article Ref. #: 1000DOJ1104 Ever since its first introduction seven decades ago, there has been continuous advance- ment of the concept and technique of Interproximal enamel reduction (IPR). It’s demonstrated Article History that with correct case selection and clinical performance, IPR is safe and effective for alleviat- Received: October 28th, 2014 ing crowding, improving dental and gingival aesthetics as well as facilitating post-treatment Accepted: December 5th, 2014 stability. The fulfilment of treatment outcomes depends on careful pre-treatment examination Published: December 8th, 2014 and planning, appropriate clinical procedures and effective post-treatment protection. This re- view aims to provide a general introduction to IPR in terms of its history background, risks and Citation benefits and clinical performance. Chee D, Ren C, Yang Y. An overview on interproximal enamel reduction. Dent Open J. 2014; 1(1): 14-18. doi: KEYWORDS: Interproximal enamel reduction; Orthodontic treatment; Crowding; Tooth re- 10.17140/DOJ-1-104 contouring. INTRODUCTION Interproximal enamel reduction (IPR) also described as “stripping”, “reproximation” and “slenderizing” has been applied in clinical orthodontics for almost seven decades.1,2 By removing part of the enamel tissue from the interproximal contact area, this technique has been proved to be effective in improving dental alignment, stability and aesthetics. -

The Concept of a New Dental Disease: Orthodontosis and Orthodontitis
Journal of Dental Health, Oral Disorders & Therapy The Concept of a New Dental Disease: Orthodontosis and Orthodontitis Abstract Research Article Introduction: Angle’s 110 year old classification of malocclusion lacks verifiable Volume 1 Issue 5 - 2014 scientific validity, and lacks substantiation on whether ideal occlusion significantly 1 2 locationimproves of oral bone function in the horizontal or provides dimension. significant benefits in oral or general health. We Anthony D Viazis , Evangelos Viazis and propose a new orthodontic classification based on evaluating the position of roots and Tom C Pagonis3* Materials and Methods: Thousands of completed orthodontic cases, with an 1Orthodontist, Private Practice, USA 2Private Practice, Greece 3Department of Restorative Dentistry and Biomaterials overwhelming majority treated non-extraction were subjected to photographic and of Sciences, Harvard School of Dental Medicine, USA radiographic evaluation. Based upon this we propose new orthodontic classifications *Corresponding author: in the horizontal dimension caused by the displaced root(s) of the tooth, typically palatallya. Orthodontosis, or lingually. defined as the non-inflammatory deficiency of the alveolar bone Tom C Pagonis, Department of Restorative Dentistry and Biomaterials Sciences, Harvard School of Dental Medicine, 188 Longwood Avenue, Boston, MA 02115, USA, Tel: +1617-432-5846; Fax: +1617-432- b.Discussion: Orthodontitis To date, defined a link as betweenexcess soft malocclusions tissue manifestation and periodontal and chronic condition inflammation. remains 0901;Received: Email: August 24, 2014 | Published: September 30, 2014 and treated accordingly based on their own individual genetic and morphologic appearanceunclear and rather controversial. than an arbitraryWith this ideal. new classification patients will be diagnosed Conclusion: is proposed for malpositioned teeth based on the clinical morphology, appearance A new orthodontic classification namely Orthodontosis and Orthodontitis orthodonticand contour therapeuticof the alveolar modalities. -

Orthodontics & Esthetic Dentistry
SCIENTIFIC SESSION TORONTO 2016 ORTHODONTICS & ESTHETIC DENTISTRY: MISSION POSSIBLE! A Broader Approach to Interdisciplinary Esthetic Treatment David M. Sarver, DMD, MS AACD 2016 TORONTO: THURSDAY MORNING “TRIPLE PLAY!” One Session. One Theme. Three Big Hitters. Dr. David M. Sarver, along with Dr. J. William Robbins and Dr. Jeffrey Rouse, will “cover the bases” on diagnosis, decision making, and treatment planning. These three “big hitters” will be presenting sequentially in the same room on Thursday, April 28, 2016. Dr. Sarver will present “Orthodontics— How it Has Changed and What You Really Want to Know!” This article discusses how orthodontics is incorporating smile design principles into its overall functional and esthetic treatment goals. Abstract For decades, dentistry has been evolving into a Patients seeking esthetic profession that is extremely multifaceted and varied in its approach to both smile and facial esthetics. treatment today wish to The coordination of macro esthetics (the face), mini enhance their appearance esthetics (the smile), and micro esthetics (the dental for improved self-esteem esthetic component) offers a complete approach to esthetic planning. This article presents an expanded and quality of life. vision of esthetic treatment designed to take readers to another level of facial, smile, and dental esthetic planning that can elevate patient outcomes. Key Words: macro esthetics, mini esthetics, micro esthetics, orthodontics, smile design 14 Winter 2016 • Volume 31 • Number 4 Sarver Figure 1: In both multidisciplinary and orthodontic diagnosis, three esthetic divisions are advocated: macro esthetics (the face), mini esthetics (the smile), and micro esthetics (the teeth). …there are principles of cosmetic dentistry that orthodontists can use to enhance their work to provide a superior esthetic outcome. -

ANGELALIGN TECHNOLOGY INC. 時代天使科技有限公司 (The “Company”) (Incorporated in the Cayman Islands with Limited Liability)
The Stock Exchange of Hong Kong Limited and the Securities and Futures Commission take no responsibility for the contents of this Application Proof, make no representation as to its accuracy or completeness and expressly disclaim any liability whatsoever for any loss howsoever arising from or in reliance upon the whole or any part of the contents of this Application Proof. Application Proof of ANGELALIGN TECHNOLOGY INC. 時代天使科技有限公司 (the “Company”) (Incorporated in the Cayman Islands with limited liability) WARNING The publication of this Application Proof is required by The Stock Exchange of Hong Kong Limited (the “Exchange”) and the Securities and Futures Commission (the “Commission”) solely for the purpose of providing information to the public in Hong Kong. This Application Proof is in draft form. The information contained in it is incomplete and is subject to change which can be material. By viewing this document, you acknowledge, accept and agree with the Company, its sponsor, advisers or members of the underwriting syndicate that: (a) this document is only for the purpose of providing information about the Company to the public in Hong Kong and not for any other purposes. No investment decision should be based on the information contained in this document; (b) the publication of this document or supplemental, revised or replacement pages on the Exchange’s website does not give rise to any obligation of the Company, its sponsor, advisers or members of the underwriting syndicate to proceed with an offering in Hong Kong or any other -

University of Würzburg Medical Faculty Research Report 2010
University of Würzburg University of Würzburg Universitätsklinikum Würzburg Medical Faculty Medical Faculty Josef-Schneider-Str. 2 · 97080 Würzburg 2010 Report – Research University of Würzburg Medical Faculty http://www.uni-wuerzburg.de/ueber/fakultaeten/ Research Report 2010 medizin/startseite/ University of Würzburg Medical Faculty Research Report 2010 Content 1 General Part 1.1 Preface ..................................................................................................................................................................... 4 1.2. Medical Education .................................................................................................................................................... 10 1.3 Students’ Representatives ......................................................................................................................................... 13 1.4 The History of the Würzburg Medical Faculty ............................................................................................................... 14 2. Research Institutes 2.1 Institute of Anatomy and Cell Biology, Chair of Anatomy I .............................................................................................. 16 2.2 Institute of Anatomy and Cell Biology, Chair of Anatomy II ............................................................................................. 18 2.3 Institute of Anatomy and Cell Biology, Chair of Anatomy III ........................................................................................... -

An Overview on Interproximal Enamel Reduction Review
DENTISTRY ISSN 2377-1623 http://dx.doi.org/10.17140/DOJ-1-104 Open Journal Review An Overview on Interproximal Enamel *Corresponding author Reduction Yanqi Yang Assistant Professor in Orthodontics Faculty of Dentistry, the University of Deborah Chee#, Chong Ren# and Yanqi Yang* Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying #equally contributed Pun, Hong Kong, China Tel. +852-28590252 Orthodontics, Faculty of Dentistry, the University of Hong Kong, 34 Hospital Road, Hong Kong Fax: +852-25593803 SAR, China E-mail: [email protected] Volume 1 : Issue 1 ABSTRACT Article Ref. #: 1000DOJ1104 Ever since its first introduction seven decades ago, there has been continuous advance- ment of the concept and technique of Interproximal enamel reduction (IPR). It’s demonstrated Article History that with correct case selection and clinical performance, IPR is safe and effective for alleviat- Received: October 28th, 2014 ing crowding, improving dental and gingival aesthetics as well as facilitating post-treatment Accepted: December 5th, 2014 stability. The fulfilment of treatment outcomes depends on careful pre-treatment examination Published: December 8th, 2014 and planning, appropriate clinical procedures and effective post-treatment protection. This re- view aims to provide a general introduction to IPR in terms of its history background, risks and Citation benefits and clinical performance. Chee D, Ren C, Yang Y. An overview on interproximal enamel reduction. Dent Open J. 2014; 1(1): 14-18. doi: KEYWORDS: Interproximal enamel reduction; Orthodontic treatment; Crowding; Tooth re- 10.17140/DOJ-1-104 contouring. INTRODUCTION Interproximal enamel reduction (IPR) also described as “stripping”, “reproximation” and “slenderizing” has been applied in clinical orthodontics for almost seven decades.1,2 By removing part of the enamel tissue from the interproximal contact area, this technique has been proved to be effective in improving dental alignment, stability and aesthetics. -

Movingnot Removing Enamel
VOLUME 01 / ISSUE 01 The Academy for Clear Aligner Therapy the AmericanJournal Academy of Cosmetic Orthodontics MOVING not removing ENAMEL. PEER-REVIEWED SOLUTIONS that will make Clear Aligner Treatment THAT MUCH EASIER. Like this Journal? start receiving your quarterly issue today! The official academy for Clear Aligner Therapy. Become a member TODAY! www.aacortho.com AACO Board Members Dr. David Galler: President the Dr. Mark Hodge: Vice President Dr. Perry Jones: Director of Education Dr. Jeffrey Galler: Editor AmericanJournal Academy of Cosmetic Orthodontics Dr. Len Tau: Director of Media Relations Dr. Bruce McFarlane: Orthodontist, Advisory Board Article is Peer Reviewed Article offers CE Credit at www.aacortho.com Dr. David Harrnick: Orthodontist, Advisory Board Dr. Sandi Bosin: Orthodontist, Editorial Board Case Reports Dr. Peter Rivolli: ClearCorrect Clinical Expert Dr. Yana Shampanksy: Invisalign Expert 2 Upper Lateral Incisor Crossbite with Dr. Lori Trost: MTM Clinical Expert Lower Premolar in Lingual Version by Dr. Cathy Sherry 4 Invisalign Correction of a Teenager’s Class 2 Division 1 Malocclusion by Dr. David J. Harnick 8 Upper Arch Spacing and Lower Editorial Arch Overcrowding I’ve been reading numerous by Dr. David Galler dental journals every Practice Development month for many years, 14 The Economics of Buying vs. but don’t remember ever Renting Your Next Office actually reading an editorial completely, from beginning by Jake Jacklich to end. 16 “Doctor, I’ve been your patient for I resolved that in this, my first 10 years; how come you never editorial for the Journal of the American mentioned orthodontics before?” Academy of Cosmetic Orthodontics, by Gary Kadi I would write an editorial that readers Retention would, in fact, read from the very first to the very last word. -

Orthodontic Treatment of Class Three Malocclusion Using Clear Aligners
Journal of Oral Biology and Craniofacial Research 9 (2019) 360–362 Contents lists available at ScienceDirect Journal of Oral Biology and Craniofacial Research journal homepage: www.elsevier.com/locate/jobcr Case study Orthodontic treatment of class three malocclusion using clear aligners: A case report T ∗ Edoardo Staderini , Simonetta Meuli, Patrizia Gallenzi Institute of Dentistry and Maxillofacial Surgery, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Largo A, Gemelli N°1, Rome, RM, 00168, Italy ARTICLE INFO ABSTRACT Keywords: Class III malocclusion is a growth-related challenging condition for orthodontists. We present a case of a 11-year- Angle class III old girl with a skeletal class III malocclusion with bilateral cross bite, and a functional shift of the lower dental Clear aligner midline. A multiphase clear aligners' treatment was scheduled with the aim of removing all dental interferences Interceptive orthodontic treatment which involved an anterior displacement of the mandible. At one-year follow-up, clear aligners’ therapy resulted in skeletal and dental improvements. Clear aligners therapy represents a valid alternative to fixed appliance therapy in the early interception of class III malocclusion. The present manuscript was prepared following the CARE guidelines. 1. Introduction relation was noticed.4 At intraoral evaluation, the patient presented a late mixed dentition with a bilateral class III malocclusion, along with a Class III malocclusion is a challenging dentoalveolar growth defor- functional mandibular lateral deviation towards the patient's left side, mity, affecting between 5.5% and 19.4% of the population.1 Early without any sign or symptom of temporomandibular joint disorders. -
3D Airway Changes Using CBCT in Patients Following Mandibular Setback Surgery ± Maxillary Advancement
Received: 5 December 2018 | Accepted: 7 December 2018 DOI: 10.1111/ocr.12291 SUPPLEMENT ARTICLE 3D Airway changes using CBCT in patients following mandibular setback surgery ± maxillary advancement Andrew G. Havron1 | Sharon Aronovich2 | Anita V. Shelgikar3 | H. Ludia Kim4 | R. Scott Conley5 1Department of Orthodontics and Pediatric Dentistry, University of Michigan, Ann Structured Abstract Arbor, Michigan Introduction: The aim of this study was to determine the 3D airway changes that 2 Department of Oral and Maxillofacial occur following mandibular setback surgery alone vs bimaxillary surgery in patients Surgery, University of Michigan, Ann Arbor, Michigan with similar skeletal start forms. 3Department of Neurology, University of Setting and Sample Population: The University of Michigan School of Dentistry and Michigan, Ann Arbor, Michigan Medical Center. A total of 85 patients undergoing mandibular setback with or with- 4Private Practice, Ann Arbor, Michigan out simultaneous maxillary advancement. 5Department of Orthodontics, University at Buffalo, Buffalo, New York Materials and Methods: A retrospective evaluation of pre- and post- surgical CBCT scans for patients undergoing mandibular setback surgery alone (14) vs bimaxillary Correspondence R. Scott Conley, University at Buffalo School surgery (71) was performed. Cross- sectional evaluation at standardized locations, of Dental Medicine, Buffalo, NY. minimum cross section and volumetric analysis were performed (Dolphin Imaging & Email: [email protected] Management Solutions). Results: Patients who underwent mandibular setback surgery alone showed a statis- tically significant average increase of 47.5 mm2 in minimum axial area. Patients who underwent bimaxillary surgery showed a statistically significant increase in airway volume, minimum axial area, location of minimum axial area, and axial area at the re- tropalatal and retroglossal regions. -

Journal of Cosmetic Dentistry
Journal of Cosmetic Dentistry Rubber Dam First Calin Pop, DDS Analysis with Imaging & Photography Conservative Composite Bonding 2020 VOLUME 36 ISSUE 3 “We asked, they delivered!” Based on AACD members’ feedback, Ivoclar Vivadent developed a NEW Higher Viscocity Veneer Cement. Amanda Seay, DDS, FAACD INTRODUCING Variolink® Esthetic LC HV Higher viscosity light curing cement • Controlled seating GET YOUR FREE REFILL AT • Precise cleanup blog.ivoclarvivadent.us/free-variolink-sample • Ideal for veneers ivoclarvivadent.com For more information, call us at 1-800-533-6825 in the U.S., 1-800-263-8182 in Canada. © 2020 Ivoclar Vivadent, Inc. Ivoclar Vivadent and Variolink are registered trademarks of Ivoclar Vivadent, Inc. 13722_VE LC HV_JCD.indd 1 11/3/20 3:51 PM A PEER-REVIEWED PUBLICATION OF THE AMERICAN ACADEMY OF COSMETIC DENTISTRY EDITORIAL REVIEW BOARD Pinhas Adar, MDT, CDT, Atlanta, GA Irfan Ahmad, BDS, Middlesex, United Kingdom Somkiat Aimplee, DDS, MSc, AAACD, Bangkok, Thailand volume 36 issue 3 Gary Alex, DMD, AAACD, Huntington, NY Journal of Cosmetic Dentistry Edward P. Allen, DDS, PhD, Dallas, TX Chad J. Anderson, DMD, MS, Fresno, CA Elizabeth M. Bakeman, DDS, FAACD, Grand Rapids, MI Lee Ann Brady, DMD, Glendale, AZ Kevin M. Brown, DDS, AAACD, Bellevue, WA Ricardo M. Carvalho, DDS, PhD, Vancouver, BC, Canada EDITOR-IN-CHIEF Edward Lowe, DMD, AAACD Christian Coachman, DDS, CDT, Sáo Paulo, Brazil Vancouver, BC, Canada, [email protected] John C. Cranham, DDS, Chesapeake, VA EXECUTIVE DIRECTOR Barbara J. Kachelski, MBA, CAE, [email protected] Michael W. Davis, DDS, Santa Fe, NM Newton Fahl Jr., DDS, MS, Curitiba-PR, Brazil CHIEF MARKETING OFFICER Mike DiFrisco, CAE, [email protected] Jonathan L.