Extension of the National Emergency Action Plan for Polio Eradication | 2018/2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Pishin Inital Pages(F)
The designation of geographical entities in this book, and the presentation of the material, do not imply the expression of any opinion whatsoever on the part of IUCN concerning the legal status of any country, territory, or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. Published by: IUCN Pakistan Copyright: © 2011 IUCN, the International Union for Conservation of Nature and Natural Resources. Pishin - Integrated District Development Vision was developed by the Pishin District Government, with technical assistance of IUCN Pakistan under its project Balochistan Partnerships for Sustainable Development (BPSD) and financial support by the Embassy of the Kingdom of the Netherlands (EKN). Citation is encouraged. Reproduction and/or translation of this publication for educational or other non-commercial purposes is authorised without prior written permission from IUCN Pakistan, provided the source is fully acknowledged. Reproduction of this publication for resale or other commercial purposes is prohibited without prior written permission from IUCN Pakistan. The opinions expressed in this document do not constitute an endorsement by the EKN. Citation: Pishin District Government (2011). Pishin - Integrated District Development Vision. IUCN Pakistan, Quetta, Pakistan. xii+100 pp. Research and development: Abdul Latif Rao Resource person: Hamid Sarfraz Facilitation: Zabardast Khan Bangash, Mehboob Ali, Naseebullah Khan Editors: Madiha Aijaz, Zeevar Scheik and Sara Fatima Azfar Design: Azhar Saeed, IUCN Pakistan Cover photographs: Naseebullah Khan, Madiha Aijaz and IUCN Balochistan Programme Printed by: Rosette Printers Available from: IUCN Pakistan Balochistan Programme Office Marker Cottage, Zarghoon Road Quetta, Pakistan Tel: +92 (81) 2840450/51/52 Fax: +92 (81) 2820706 www.iucn.org/pakistan Pishin Integrated Development Vision Contents Acronyms . -

Buffer Zone, Colonial Enclave, Or Urban Hub?
Working Paper no. 69 - Cities and Fragile States - BUFFER ZONE, COLONIAL ENCLAVE OR URBAN HUB? QUETTA :BETWEEN FOUR REGIONS AND TWO WARS Haris Gazdar, Sobia Ahmad Kaker, Irfan Khan Collective for Social Science Research February 2010 Crisis States Working Papers Series No.2 ISSN 1749-1797 (print) ISSN 1749-1800 (online) Copyright © H. Gazdar, S. Ahmad Kaker, I. Khan, 2010 24 Crisis States Working Paper Buffer Zone, Colonial Enclave or Urban Hub? Quetta: Between Four Regions and Two Wars Haris Gazdar, Sobia Ahmad Kaker and Irfan Khan Collective for Social Science Research, Karachi, Pakistan Quetta is a city with many identities. It is the provincial capital and the main urban centre of Balochistan, the largest but least populous of Pakistan’s four provinces. Since around 2003, Balochistan’s uneasy relationship with the federal state has been manifested in the form of an insurgency in the ethnic Baloch areas of the province. Within Balochistan, Quetta is the main shared space as well as a point of rivalry between the two dominant ethnic groups of the province: the Baloch and the Pashtun.1 Quite separately from the internal politics of Balochistan, Quetta has acquired global significance as an alleged logistic base for both sides in the war in Afghanistan. This paper seeks to examine different facets of Quetta – buffer zone, colonial enclave and urban hub − in order to understand the city’s significance for state building in Pakistan. State-building policy literature defines well functioning states as those that provide security for their citizens, protect property rights and provide public goods. States are also instruments of repression and the state-building process is often wrought with conflict and the violent suppression of rival ethnic and religious identities, and the imposition of extractive economic arrangements (Jones and Chandaran 2008). -

Evaluating Urbanization Impact on Stressed Aquifer of Quetta Valley, Pakistan
Desalination and Water Treatment 222 (2021) 103–113 www.deswater.com May doi: 10.5004/dwt.2021.27068 Evaluating urbanization impact on stressed aquifer of Quetta Valley, Pakistan Faizan Dawooda, Malik Muhammad Akhtarb,*, Muhsan Ehsanc aDepartment of Civil Engineering, Balochistan University of Information Technology, Engineering and Management Sciences, Quetta, Pakistan, email: [email protected] bDepartment of Environmental Sciences, Balochistan University of Information Technology, Engineering and Management Sciences, Quetta, Pakistan, Tel. +92 335 445 7067; email: [email protected] cDepartment of Earth and Environmental Sciences, Bahria University, Islamabad, Pakistan, email: [email protected] Received 14 February 2020; Accepted 16 January 2021 abstract This research is focused on the land use/land cover (LU/LC) changes impacts on the groundwater table and urbanization trend of Quetta valley for a period of 10 y. The land cover changes are occur- ring locally, regionally, and worldwide, which results in the expansion of urbanization trend and groundwater table depletion. Population growth leads to fast change in land use patterns, which increases the demand for basic needs. Urbanization and climatic impacts on depleting groundwa- ter resources in Quetta need to assess and find a scientific solution using applications of the latest software. This study investigated the land cover changes in three categories, which were barren land, vegetation, built-up area by using maximum likelihood classification (MLC). Water table depletion was defined in five ranges from very low to very high by using the Kriging Method. It is inferred that the built-up area was increased the most in the last 10 y, that is, 2008–2018 as com- pared to other classes. -

Balochistan Province Report on Mouza Census 2008
TABLE 1 NUMBER OF KANUNGO CIRCLES,PATWAR CIRCLES AND MOUZAS WITH STATUS NUMBER OF NUMBER OF MOUZAS KANUNGO CIRCLES/ PATWAR ADMINISTRATIVE UNIT PARTLY UN- SUPER- CIRCLES/ TOTAL RURAL URBAN FOREST URBAN POPULATED VISORY TAPAS TAPAS 1 2 3 4 5 6 7 8 9 BALOCHISTAN 179 381 7480 6338 127 90 30 895 QUETTA DISTRICT 5 12 65 38 15 10 1 1 QUETTA CITY TEHSIL 2 6 23 7 9 7 - - QUETTA SADDAR TEHSIL 2 5 38 27 6 3 1 1 PANJPAI TEHSIL 1 1 4 4 - - - - PISHIN DISTRICT 6 17 392 340 10 3 8 31 PISHIN TEHSIL 3 6 47 39 2 1 - 5 KAREZAT TEHSIL 1 3 39 37 - 1 - 1 HURAM ZAI TEHSIL 1 4 16 15 - 1 - - BARSHORE TEHSIL 1 4 290 249 8 - 8 25 KILLA ABDULLAH DISTRICT 4 10 102 95 2 2 - 3 GULISTAN TEHSIL 1 2 10 8 - - - 2 KILLA ABDULLAH TEHSIL 1 3 13 12 1 - - - CHAMAN TEHSIL 1 2 31 28 1 2 - - DOBANDI SUB-TEHSIL 1 3 48 47 - - - 1 NUSHKI DISTRICT 2 3 45 31 1 5 - 8 NUSHKI TEHSIL 1 2 26 20 1 5 - - DAK SUB-TEHSIL 1 1 19 11 - - - 8 CHAGAI DISTRICT 4 6 48 41 1 4 - 2 DALBANDIN TEHSIL 1 3 30 25 1 3 - 1 NOKUNDI TEHSIL 1 1 6 5 - - - 1 TAFTAN TEHSIL 1 1 2 1 - 1 - - CHAGAI SUB-TEHSIL 1 1 10 10 - - - - SIBI DISTRICT 6 15 161 124 7 1 6 23 SIBI TEHSIL 2 5 35 31 1 - - 3 KUTMANDAI SUB-TEHSIL 1 2 8 8 - - - - SANGAN SUB-TEHSIL 1 2 3 3 - - - - LEHRI TEHSIL 2 6 115 82 6 1 6 20 HARNAI DISTRICT 3 5 95 81 3 3 - 8 HARNAI TEHSIL 1 3 64 55 1 1 - 7 SHARIGH TEHSIL 1 1 16 12 2 1 - 1 KHOAST SUB-TEHSIL 1 1 15 14 - 1 - - KOHLU DISTRICT 6 18 198 195 3 - - - KOHLU TEHSIL 1 2 37 35 2 - - - MEWAND TEHSIL 1 5 38 37 1 - - - KAHAN TEHSIL 4 11 123 123 - - - - DERA BUGTI DISTRICT 9 17 224 215 4 1 - 4 DERA BUGTI TEHSIL 1 -

New Discovered Archaeological Sites in Nushki District of Balochistan (A Field Report)
- 59 - BI-ANNUAL RESEARCH JOURNAL “BALOCHISTAN REVIEW” ISSN 1810-2174 Balochistan Study Centre, UoB, Quetta (Pak) VOL. XXVIII NO.1, 2013 NEW DISCOVERED ARCHAEOLOGICAL SITES IN NUSHKI DISTRICT OF BALOCHISTAN (A FIELD REPORT) History Farooq Baloch*& Waheed Razzaq† Abstract: Balochistan is known as a mother land of ancient cultures because, of its countless Archaeological sites. Balochistan is divided among three countries, Pakistan, Iran and Afghanistan, and the part Pakistan consists approximately 3, 47,190, square kilometer, and it is 44% out of the total area of Pakistan. It is further divided into 6 Divisions and 30 Districts. Every district has a huge importance by its Archaeological sites which consist on Mounds, Graveyards, Tombs, Inscriptions, Karezes and Ancient Dames etc. Some very important sites are excavated by the Archaeologists, like Mehrgarh in Bolan District, Peerak in Sibi District, Mound of Killi Gul Mohammad in Quetta District, Pariano Ghundai in Zhob District, Anjeera in Kalat District, Bala Kot in Bela District and Meeri Kalat in Kech District, etc., large number of archaeological sites have been discovered but still they are not excavated. On the other side different archaeolocial sites of Balochistan are still unexplored. Many sites are still hidden and not discovered by any Archaeologist, the sites of Nushki District have always been ignored by local peopal and Archaeologists. In the espect of Archaeology Nushki has also many attractive and important archaeological sites. The following research article is about the new discovered Archaeological sites in the Nushki District by a team of Balochistan study centre. The objectives behind this study are to overview the new Archaeological sites in the Nushki District and explain their historical, cultural, anthropological and social importance. -

Development Profile District Quetta
District Development Q Development u e P R O F I L E t t 2 0 1 1 a - D i s t Quetta r i c t D e v e l o p m e n t P r o f i l e 2 0 1 1 Planning & Development Department United Nations Children’s Fund Government of Balochistan, Quetta Provincial Office Balochistan, Quetta Planning & Development Department, Government of Balochistan in Collaboration with UNICEF District Development P R O F I L E 2 0 1 1 Q u e t t a Prepared by Planning & Development Department, Government of Balochistan, Quetta in Collaboration with United Nations Children’s Fund Provincial Office Balochistan, Quetta July 18, 2011 Message Foreword In this age of knowledge economy, reliance on every possible tool The Balochistan District Development Profile 2010 is a landmark exercise of Planning and available for decision making is crucial for improving public resource Development Department, Government of Balochistan, to update the district profile data management, brining parity in resource distribution and maximizing that was first compiled in 1998. The profiles have been updated to provide a concise impact of development interventions. These District Development landmark intended for development planning, monitoring and management purposes. Profiles are vivid views of Balochistan in key development areas. The These districts profiles would be serving as a tool for experts, development practitioners Planning and Development Department, Government of Balochistan and decision-makers/specialists by giving them vast information wrapping more than 18 is highly thankful to UNICEF Balochistan for the technical and dimensions from Balochistan’s advancement extent. -

Secondary Education Department Government of Balochistan 0
E3092v2 ENVIRONMENTAL AND SOCIAL IMPACT ASSESSMENT Public Disclosure Authorized (ESIA) Promoting Girls Education in Balochistan (PGEB) Project Public Disclosure Authorized Public Disclosure Authorized (AUGUST 2012) Public Disclosure Authorized Project Director PROMOTING GIRLS EDUCATION IN BALOCHISTAN PROJECT SECONDARY EDUCATION DEPARTMENT GOVERNMENT OF BALOCHISTAN 0 Tel: + 92 81 9202102 1 EXECUTIVE SUMMARY 1. The present environmental and social impact assessment (ESIA) study of the Promoting Girls Education in Balochistan (PGEB) project has been carried out in compliance with the national environmental laws of Pakistan and the World Bank Operational Policies (OPs). The ESIA delineates the environmental and social issues emerging from the PGEB project, identifies the potentially adverse environmental and social impacts of the project activities, and suggests appropriate mitigation measures to offset or reduce these impacts. The report also suggests guidelines for environmental enhancement opportunities available during various phases of project implementation to maximize the benefit to environment. The mitigation measures and guidelines have been organized in the form of an environmental and social management plan (ESMP) to be implemented by the Project Management Unit (PMU) of the PGEB project for avoiding or mitigating the significant environment and social impacts. 2. The scope of the study entails assessment of the environmental and social impacts of PGEB project activities in the selected 12 districts of the province including Kachhi, Loralai, Jhal Magsi, Khuzdar, Kalat, Lasbela, Jaferabad, Kech, Panjgur, Kila Saifullah, Pishin and Naseerabad districts. The project area spreads over from north to south of the province covering almost 138,011 square kilometers (40%) area of the province. The environmental and social assessment covers physical, biological and social impacts of project activities during various implementation stages from site selection and designing to construction and operational phase of the school buildings. -

Delivery of MNH Services in Conflict Areas of KP, Balochistan, and FATA
November 2013 Care-Plus Delivery of MNH Services A Project Funded by: Principal Investigator Research Team Maternal and Newborn Health Programme Dr. Asma Bokhari Dr. Muhammad Bashirul Haq in Conflict Areas of Research and Advocacy Fund (RAF) Co-Principal Investigator Ms. Sadia Batool Implemented by: Ms. Meher Sana Arshad Prof Dr. Naveed-i-Rahat KP, Balochistan and FATA SoSec Consulting Services Mr. Moin ud din Declaration “I have read the report titled “Care-Plus Delivery of MNH Services in Conflict Areas of KP, Balochistan and FATA” and acknowledge and agree with the information, data and findings contained”. Dr. Riaz A Malik Managing Director, SoSec Consulting Services Islamabad i Introduction Anthropologist / Provincial Coordinators had a positive impact on field activity. The Programme Coordinator also supervised the fieldwork, and sought clarification wherever needed about the data Pakistan in recent years has faced ongoing conflict and insurgency in the provinces of Khyber received from the field. Pakhtunkhwa (KP), Balochistan, and the Federally Administered Tribal Areas (FATA). Hence, access to social services, including Maternal and Newborn Health (MNH) services was significantly reduced in Four senior researchers holding Ph.D. and M.Sc. degree in Anthropology/ Social Sciences were the conflict areas. selected as Data Analysts. The Data Analysts managed the data systematically by assigning a unique identification number to each transcript received from the field. Data analysis was done manually using This qualitative research study, was undertaken both at the demand and supply sides of the matrices developed in Microsoft Excel. The Anthropologist supervised the data management and data governance equation. On the demand side, the research assessed the influence of patriarchal power analysis. -

Khuzdar – Quetta Industrial 132KV Double Circuit Transmission Line Subproject
Initial Environmental Examination October 2012 MFF 0021-PAK: Power Distribution Enhancement Investment Program – Proposed Tranche 3 Prepared by the Quetta Electric Supply Company for the Asian Development Bank. Power Distribution Enhancement Project (PAK) Tranche 3 INITIAL ENVIRONMENTAL EXAMINATION (Draft) Khuzdar – Quetta Industrial 132KV Double Circuit Transmission line Subproject Submitted to Asian Development Bank October 2012 Submitted By Quetta Electric Supply Company (QESCO) Government of the Islamic Republic of Pakistan Power Distribution Enhancement Multi Tranche Financing Facility PAK Tranche 3 Khuzdar-Quetta Industrial 132KV DC Transmission line Initial Environmental Examination Table of Contents 1. Introduction 1 1.1 Overview 1 1.2 Background 3 1.3 Scope of the IEE Study and Personnel 3 1.4 Policy and Statutory Requirements in Pakistan 5 1.5 Structure of Report 9 2. Description of the Project 11 2.1 Type of Project 11 2.2 Categorization of the Project 11 2.3 Need for the Project 11 2.4 Location and Scale of Project 12 2.5 Decommissioning and Disposal of Material 9 2.6 QESCO Subproject 13 2.7 Proposed Schedule for Implementation 13 3. DESCRIPTION OF THE ENVIRONMENT 14 3.1 Project Area 14 3.2 Physical Resources 14 3.3 Ecological Resources 17 3.4 Economic Development 18 3.5 Social and Cultural Resources 19 4. SCREENING POTENTIAL ENVIRONMENTAL IMPACTS AND MITIGATION MEASURES 22 4.1 Project Location 22 4.2 General Approach to Mitigation 22 4.3 Potential Environmental Impacts during Design & Pre-Construction Stage 24 4.4 Potential Environmental Impacts from Construction 24 4.5 Potential Environmental Impacts during Operation 28 5. -

Quetta :Between Four Regions and Two Wars
Working Paper no. 69 - Cities and Fragile States - BUFFER ZONE, COLONIAL ENCLAVE OR URBAN HUB? QUETTA :BETWEEN FOUR REGIONS AND TWO WARS Haris Gazdar, Sobia Ahmad Kaker, Irfan Khan Collective for Social Science Research February 2010 Crisis States Working Papers Series No.2 ISSN 1749-1797 (print) ISSN 1749-1800 (online) Copyright © H. Gazdar, S. Ahmad Kaker, I. Khan, 2010 24 Crisis States Working Paper Buffer Zone, Colonial Enclave or Urban Hub? Quetta: Between Four Regions and Two Wars Haris Gazdar, Sobia Ahmad Kaker and Irfan Khan Collective for Social Science Research, Karachi, Pakistan Quetta is a city with many identities. It is the provincial capital and the main urban centre of Balochistan, the largest but least populous of Pakistan’s four provinces. Since around 2003, Balochistan’s uneasy relationship with the federal state has been manifested in the form of an insurgency in the ethnic Baloch areas of the province. Within Balochistan, Quetta is the main shared space as well as a point of rivalry between the two dominant ethnic groups of the province: the Baloch and the Pashtun.1 Quite separately from the internal politics of Balochistan, Quetta has acquired global significance as an alleged logistic base for both sides in the war in Afghanistan. This paper seeks to examine different facets of Quetta – buffer zone, colonial enclave and urban hub − in order to understand the city’s significance for state building in Pakistan. State-building policy literature defines well functioning states as those that provide security for their citizens, protect property rights and provide public goods. States are also instruments of repression and the state-building process is often wrought with conflict and the violent suppression of rival ethnic and religious identities, and the imposition of extractive economic arrangements (Jones and Chandaran 2008). -
Quetta Blockwise
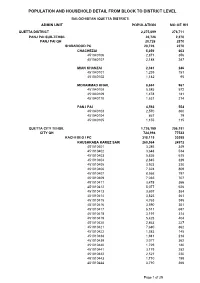
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL BALOCHISTAN (QUETTA DISTRICT) ADMIN UNIT POPULATION NO OF HH QUETTA DISTRICT 2,275,699 276,711 PANJ PAI SUB-TEHSIL 20,726 2,370 PANJ PAI QH 20,726 2370 SHIRAROOD PC 20,726 2370 CHACHEZAI 5,059 603 451040106 2,871 356 451040107 2,188 247 MIAN KHANZAI 2,381 246 451040101 1,239 151 451040102 1,142 95 MOHAMMAD KHAIL 8,694 967 451040108 5,585 572 451040109 1,478 181 451040110 1,631 214 PANJ PAI 4,592 554 451040103 2,570 360 451040104 867 79 451040105 1,155 115 QUETTA CITY TEHSIL 1,726,199 206,151 CITY QH 724,994 77533 KACHI BEG I PC 318,115 30395 KHUSHKABA KAREZ SARIAB 260,564 24972 451010401 3,286 349 451010402 3,648 534 451010403 5,826 615 451010404 2,845 329 451010405 3,923 330 451010406 7,324 809 451010407 8,566 797 451010409 7,036 707 451010411 3,478 366 451010412 5,077 626 451010413 3,697 384 451010414 3,823 361 451010415 4,763 395 451010416 3,590 351 451010417 6,511 697 451010418 3,191 314 451010419 5,425 404 451010420 2,863 227 451010421 7,680 862 451010422 1,583 145 451010438 1,941 218 451010439 3,077 362 451010440 1,729 180 451010441 3,179 282 451010442 2,521 220 451010443 1,710 195 451010444 3,710 366 Page 1 of 25 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL BALOCHISTAN (QUETTA DISTRICT) ADMIN UNIT POPULATION NO OF HH 451010445 5,667 591 451010446 5,675 498 451010447 2,063 342 451010448 6,413 580 451010449 4,524 394 451010450 9,103 938 451010451 4,617 436 451010452 4,092 479 451010453 6,419 477 451010454 2,631 217 451010455 6,719 518 451010456 2,714 218 -

EARTHQUAKE in BALOCHISTAN PAKISTAN Situation Report No
EARTHQUAKE IN BALOCHISTAN PAKISTAN Situation Report No. 2 1 November 2008 OVERVIEW • The National Disaster Management Authority confirms 155 deaths and over 375 people injured. Media reports more than 300 deaths. • Adequate health coverage in all major Quetta hospitals and there is still capacity to accommodate more casualties. • From day one, WHO Polio and DEWS surveillance teams have participated in damage and needs assessments in Ziarat and Pishin districts. • The Department of Health (DoH) dispatched 10 teams to affected districts to vaccinate children and women against measles and tetanus and provide vitamin A to children. • The DoH and Health Cluster partners ensuring provision of care in affected districts. • Emergency Health Cluster meeting on 30 October in Islamabad held to coordinate response activities. Next meeting scheduled for 3 November. SITUATION UPDATE • The 28 October 2008 earthquake in Baluchistan caused massive destruction in Ziarat and Pishin districts, some parts of Zhob district and Quetta. The National Disaster Management Authority (NDMA) reports 155 deaths and more than 375 people injured, with media reporting more than 300 deaths. In affected areas, night temperatures have fallen below freezing. • In Ziarat district (130 000 people), 14 villages in Kawas and Kach Union Councils (35 000 people) are badly affected. Around 12 000 people are displaced. • In Pishin district (475 619 people), Khanozai, Rod Mulazai and Dilsora Union Councils are the most affected. • Recurring aftershocks have prompted some people to move to safer places. The remaining population is living in tents or partially damaged houses. However, there are not enough tents to accommodate all of them, leaving many exposed to harsh cold weather and risk of respiratory diseases.