June 1, 2021 Dear Prevea360 Health Plan Provider
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
= 'NH., Diseases, Central Nerrous System M)Ury and Different Foims of Mflannnation
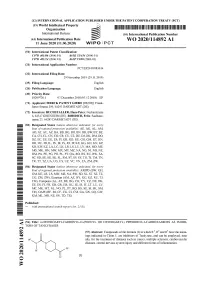
(12) INTERNATIONAL APPLICATION Pl;BLISHED 1. NDER THE PATENT COOPERATION TREATY (PCT) (19) World intellectual Property Organraation llIlllIlllIlIllllllllIlllllIIllIllIlllIlllllllllllIlllIllIlIlllIllIlIllIllIlIIIIIIIIIIIIIIIIIII International Bureau (10) International Publication Number (43) International Publication Date WO 2020/114892 Al 11 June 2020 (11.06.2020) W 4 P Gl I P 0 T (51) International Patent Classification: C07D 401/06 (200G 0 I) AGJK31/454 (200G 0l) C07D dt)J//4 (2006 01) A61P35/ttd (200G 0l) (21) International Application Number: PCT/EP2019/l)8 3014 (22) International Filing Date: 29 Nosember 2019 (29.11.2019) (25) Filing Language: Enghsh (26) Publication Language Enghsh (30) Priority Data: 1820972/i 1 03 December 20)8 (03 12 2018) EP (71) Applicant: MERCK PATENT GMBH IDE/DE]. Frm&(s- furter Strasse 230. 64293 DARMSTADT (DE) (72) Inventors: BUCHSTALLER, Hans-Peter. Ncc)sa&strasse G. G4347 GRIESHELVI (DE). ROHDICH, Feliru Saalbaus- tmssc 23. 64283 DARMSTADT (DE). (81) Designated States /unless i&themmse n&d&ct&md, /or e&ery hind of national protect«&n menial&le/ AF, AG, AL, AVI AO, AT. AU. AZ, BA, BB, BG, BH. B N. BR, BW, BY. BZ. CA. CH, CL, CN. CO, CR. C U, CZ. DE, DJ, DK. DM DO. DZ, EC. EE, EG. ES. FI, GB. GD. GE. GH, GM. GT. HN. HR. HU, ID, IL. IN, IR, IS. JO, JP, KE. KG, KH. KN, KP. KR. KW, KZ, LA. L C, LK. LR, LS, LU. LY. MA. MD, ME. WIG. MK. MN, MW, MX. MY. MZ. NA. NG. NI, NO. NZ. OM, PA. PE, PG. PH, PL. PT. QA, RO, RS. -

Antibody–Drug Conjugates
Published OnlineFirst April 12, 2019; DOI: 10.1158/1078-0432.CCR-19-0272 Review Clinical Cancer Research Antibody–Drug Conjugates: Future Directions in Clinical and Translational Strategies to Improve the Therapeutic Index Steven Coats1, Marna Williams1, Benjamin Kebble1, Rakesh Dixit1, Leo Tseng1, Nai-Shun Yao1, David A. Tice1, and Jean-Charles Soria1,2 Abstract Since the first approval of gemtuzumab ozogamicin nism of activity of the cytotoxic warhead. However, the (Mylotarg; Pfizer; CD33 targeted), two additional antibody– enthusiasm to develop ADCs has not been dampened; drug conjugates (ADC), brentuximab vedotin (Adcetris; Seat- approximately 80 ADCs are in clinical development in tle Genetics, Inc.; CD30 targeted) and inotuzumab ozogami- nearly 600 clinical trials, and 2 to 3 novel ADCs are likely cin (Besponsa; Pfizer; CD22 targeted), have been approved for to be approved within the next few years. While the hematologic cancers and 1 ADC, trastuzumab emtansine promise of a more targeted chemotherapy with less tox- (Kadcyla; Genentech; HER2 targeted), has been approved to icity has not yet been realized with ADCs, improvements treat breast cancer. Despite a clear clinical benefit being dem- in technology combined with a wealth of clinical data are onstrated for all 4 approved ADCs, the toxicity profiles are helping to shape the future development of ADCs. In this comparable with those of standard-of-care chemotherapeu- review, we discuss the clinical and translational strategies tics, with dose-limiting toxicities associated with the mecha- associated with improving the therapeutic index for ADCs. Introduction in antibody, linker, and warhead technologies in significant depth (2, 3, 8, 9). Antibody–drug conjugates (ADC) were initially designed to leverage the exquisite specificity of antibodies to deliver targeted potent chemotherapeutic agents with the intention of improving Overview of ADCs in Clinical Development the therapeutic index (the ratio between the toxic dose and the Four ADCs have been approved over the last 20 years (Fig. -
Management of Multiple Myeloma: the Changing Paradigm
Management of Multiple Myeloma: The Changing Paradigm Relapsed/Refractory Disease Jeffrey A. Zonder, MD Karmanos Cancer Institute Objectives • Discuss use of standard myeloma therapies when used as therapy after relapse • Consider patient and disease factors which might impact therapy decisions. • Describe off-label options for patients who are not protocol candidates. Line ≠ Line ≠ Line ≠ … POLICE LINE – DO NOT CROSS POLICE LINE – DO NOT CROSS POLICE LINE – DO NOT CROSS POLICE LINE – DO NOT CROSS POLI LINE – DO NOT Define “Line” • A pre-defined course of therapy utilizing agents either simultaneously or sequentially – Len/Dex – Len/Dex ASCT – Vel/Dex ASCT Len/Dex – VDT-PACE ASCT TD ASCT VPT-PACE LD • Pts who have had the same # of “lines” of Rx may have had vastly different amounts of Rx What Is Relapsed/Refractory Disease? • Relapsed: recurrence after a response to therapy • Refractory: progression despite ongoing therapy What Do We Know About the Pt’s Myeloma? • What prior therapy has been used? • How well did it work? • Did the myeloma progress on active therapy? • High-risk cytogenetics/FISH/GEP? What Do We Know About the Patient? • Age • Other medical problems – Diabetes – Blood Clots • Lasting side effects from past therapies – Peripheral Neuropathy • Personal preferences and values Choosing Therapy for Relapsed/Refractory Myeloma Proteasome IMiDs Anthracyclines Alkylators Steroids HDACs Antibodies Inhibitors Thalidomide Bortezomib Doxil Melphalan Dex Panobinostat Elotuzumab Lenalidomide Carfilzomib Cytoxan Pred Vorinostat -

Multiple Myeloma
Advances in Treatment Paradigms for Multiple Myeloma Bao Dao, PharmD, MBA, BCPS, BCOP Hematology/Bone Marrow Transplant Clinical Pharmacist Assistant Clinical Professor University of California San Francisco Medical Center Disclosure Advisory committee member for Seattle Genetics Learning Objectives • Identify the mechanism of action of select new therapeutic agents for multiple myeloma • Summarize literature regarding the use of new agents for multiple myeloma • Explain expected outcomes to a given therapeutic modality in terms of response and toxicity • State the place in therapy of the new therapeutic agents for multiple myeloma Multiple Myeloma (MM) • MM is the second most common hematologic malignancy • Malignancy of monoclonal plasma cells • 26,850 new cases estimated in US in 2015 o 11,240 deaths • Mean age of affected individuals: 62 years old • MM remains an incurable malignancy o Goal of therapy remains disease control o Overall survival has increased 3 - 5 years to 5 - 7 years with novel agents NCCN. Multiple Myeloma. V.3.2016. Available at: www.nccn.org/professional/physician_gls/pdf/myeloma. Evolution of Myeloma Therapy Bortezomib Panobinostat Melphalan Lenalidomide Daratumumab 1950’s Ixazomib Corticosteroids 2015 2000’s Elotuzumab Thalidomide Carfilzomib Autologous Stem Cell Transplant Pomalidomide 1990’s 2010’s 2 4 Kyle RA, et al. Blood. 2008; 111(6):2962-72. Current Approach to Treatment Primary Therapy Yes ASCT Maintenance x 2-4 cycles Therapy Relapse/ Newly Transplant Refractory Diagnosed MM Candidate? Therapies Maintenance No Primary Therapy Therapy NCCN. Multiple Myeloma. V.3.2016. Available at: www.nccn.org/professional/physician_gls/pdf/myeloma. Outline Mechanism of Action FDA Approval Trial Dosing/Administration Toxicity/Monitoring Place in therapy Daratumumab • IgG human monoclonal antibody to CD38 • CD38 = transmembrane glycoprotein highly expressed on myeloma cells ◦ Low expression on other myeloid/lymphoid cells • Complement and antibody dependent cytotoxicity Lokhorst HM, et al. -

Genmab and Seattle Genetics Present Data from Tisotumab Vedotin Innovatv 204 Pivotal Trial in Recurrent Or Metastatic Cervical Cancer at ESMO Virtual Congress 2020
Genmab and Seattle Genetics Present Data from Tisotumab Vedotin innovaTV 204 Pivotal Trial in Recurrent or Metastatic Cervical Cancer at ESMO Virtual Congress 2020 Media Release COPENHAGEN, Denmark and BOTHELL, Wash., 21 September 2020 • Data featured in late-breaking proffered paper oral presentation • Biologics license application submission planned to support accelerated approval pathway with the FDA Genmab A/S (Nasdaq: GMAB) and Seattle Genetics, Inc. (Nasdaq: SGEN) today presented data from the innovaTV 204 pivotal phase 2, single-arm clinical trial evaluating tisotumab vedotin as monotherapy in patients with previously treated recurrent and/or metastatic cervical cancer at the European Society for Medical Oncology (ESMO) Virtual Congress 2020. Patients had previously received a doublet chemotherapy and, if eligible, bevacizumab as first-line therapy. Results from the trial showed a 24 percent confirmed objective response rate (ORR) by independent central review with a median duration of response (DOR) of 8.3 months. The most common treatment-related adverse events (greater than or equal to 20 percent) included alopecia, epistaxis (nose bleeds), nausea, conjunctivitis, fatigue and dry eye. Tisotumab vedotin is an investigational antibody-drug conjugate (ADC) directed to tissue factor (TF), which is prevalent on solid tumors including cervical cancer and can promote tumor growth, angiogenesis and metastasis.1 Current therapies for previously treated recurrent and/or metastatic cervical cancer generally result in limited objective response rates of typically less than 15 percent with median overall survival ranging from 6.0 to 9.4 months.1-8 “Following resistance to or progression on first-line standard of care therapy, there are limited treatment options for women with metastatic cervical cancer,” said Robert L. -

Summary of Utilization Management (UM) Program Changes May #2 2020
Summary of Utilization Management (UM) Program Changes May #2 2020 Brand Name Generic Name Utilization Update Summary Type Effective Date Adakveo crizanlizumab Trial and failure or inadequate response, Update 8/01/2020 contraindication, or intolerance to one of the following: Hydroxyurea or L- glutamine (i.e., Endari) Oxbryta voxelotor Clarified age to 12 years or older Update 8/01/2020 Givlaari givosiran Removed requirement that patient will Update 8/01/2020 not be anticipating liver transplantation. Padcev enfortumab vedotin Patient has received prior treatment with Update 8/01/2020 one immune checkpoint inhibitors (CPI) in the neoadjuvant/adjuvant, locally advanced or metastatic setting, unless contraindicated: i) Programmed death receptor-1 (PD-1) inhibitor [e.g.,Opdivo (nivolumab), Keytruda (pembrolizumab)], or ii) Programmed death-ligand 1 (PD-L1) inhibitor [e.g., Tecentriq (atezolizumab), Imfinzi (durvalumab), Bavencio (avelumab)]. Absorica LD isotretinoin A new product that has the same Update 8/01/2020 requirements as Absorica: for patients who are unresponsive to conventional therapy, including oral antibiotics, and is prescribed by a dermatologist. Jatenzo testosterone New oral formulation of testosterone. Update 8/01/2020 undecanoate Requires confirmation of diagnosis, testosterone lab values, and trial of both a testosterone patch and generic testosterone gel that are on formulary. Triluron sodium hyaluronate This new product has been added to the Update 08/01/2020 prior authorization guideline with the other hyaluronic acid derivatives. Approval requires diagnosis of osteoarthritis of the knee, a trial of two oral or an oral and topical medication, and trial of a corticosteroid injection in the knee. The 2019 American College of Rheumatology Osteoarthritis Guidelines now recommend use of duloxetine and topical capsaicin for knee osteoarthritis, so we will be adding these as alternatives to the oral/topical medications for each drug in this group. -

Elotuzumab (Empliciti®) Horizons Infosheet Clinical Trials and Novel Drugs
Elotuzumab (Empliciti®) Horizons Infosheet Clinical trials and novel drugs This Horizons Infosheet contains information on elotuzumab (also known as Empliciti®), a drug being investigated for the treatment of myeloma. The Horizons Infosheet series What is Elotuzumab? provides information relating Elotuzumab is a new drug being to novel drugs and treatment investigated for the treatment of strategies that are currently being myeloma. investigated for the treatment of myeloma. The series also aims to Elotuzumab is a monoclonal highlight the considerable amount antibody which attaches to a of research currently taking place in specific protein that is present on the field of myeloma. the surface of myeloma cells. The drugs and treatment strategies What is a monoclonal described in the Horizons Infosheets antibody? may not be licensed and/or approved for use in myeloma. You Monoclonal antibodies are a class may, however, be able to access of drug being investigated in the them as part of a clinical trial. treatment of myeloma. Infoline: 0800 980 3332 1 Monoclonal antibodies are made monoclonal monoclonal antibody drug in the laboratory to mimic the antibody drug antibodies that your own immune system produces in response to foreign organisms (such as bacteria) that enter the body. Antibodies recognise proteins on the surface of myeloma myeloma cell harmful or abnormal cells and flag cell them for destruction by the immune proteins system. proteins on the cell on the cell surface surface monoclonal monoclonal antibody locked Monoclonal antibody drugs are antibody locked onto the cell- onto the cell- surface protein designed to recognise and attach surface protein to specific proteins on the surface Figure 1. -

CDER Breakthrough Therapy Designation Approvals Data As of December 31, 2020 Total of 190 Approvals
CDER Breakthrough Therapy Designation Approvals Data as of December 31, 2020 Total of 190 Approvals Submission Application Type and Proprietary Approval Use Number Number Name Established Name Applicant Date Treatment of patients with previously BLA 125486 ORIGINAL-1 GAZYVA OBINUTUZUMAB GENENTECH INC 01-Nov-2013 untreated chronic lymphocytic leukemia in combination with chlorambucil Treatment of patients with mantle cell NDA 205552 ORIGINAL-1 IMBRUVICA IBRUTINIB PHARMACYCLICS LLC 13-Nov-2013 lymphoma (MCL) Treatment of chronic hepatitis C NDA 204671 ORIGINAL-1 SOVALDI SOFOSBUVIR GILEAD SCIENCES INC 06-Dec-2013 infection Treatment of cystic fibrosis patients age VERTEX PHARMACEUTICALS NDA 203188 SUPPLEMENT-4 KALYDECO IVACAFTOR 21-Feb-2014 6 years and older who have mutations INC in the CFTR gene Treatment of previously untreated NOVARTIS patients with chronic lymphocytic BLA 125326 SUPPLEMENT-60 ARZERRA OFATUMUMAB PHARMACEUTICALS 17-Apr-2014 leukemia (CLL) for whom fludarabine- CORPORATION based therapy is considered inappropriate Treatment of patients with anaplastic NOVARTIS lymphoma kinase (ALK)-positive NDA 205755 ORIGINAL-1 ZYKADIA CERITINIB 29-Apr-2014 PHARMACEUTICALS CORP metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib Treatment of relapsed chronic lymphocytic leukemia (CLL), in combination with rituximab, in patients NDA 206545 ORIGINAL-1 ZYDELIG IDELALISIB GILEAD SCIENCES INC 23-Jul-2014 for whom rituximab alone would be considered appropriate therapy due to other co-morbidities -

Immunotherapies Shape the Treatment Landscape for Hematologic Malignancies Jane De Lartigue, Phd
Feature Immunotherapies shape the treatment landscape for hematologic malignancies Jane de Lartigue, PhD he treatment landscape for hematologic of TIL therapy has been predominantly limited to malignancies is evolving faster than ever melanoma.1,3,4 before, with a range of available therapeutic Most recently, there has been a substantial buzz Toptions that is now almost as diverse as this group around the idea of genetically engineering T cells of tumors. Immunotherapy in particular is front and before they are reintroduced into the patient, to center in the battle to control these diseases. Here, increase their anti-tumor efficacy and minimize we describe the latest promising developments. damage to healthy tissue. This is achieved either by manipulating the antigen binding portion of the Exploiting T cells T-cell receptor to alter its specificity (TCR T cells) The treatment landscape for hematologic malig- or by generating artificial fusion receptors known as nancies is diverse, but one particular type of therapy chimeric antigen receptors (CAR T cells; Figure 1). has led the charge in improving patient outcomes. The former is limited by the need for the TCR to be Several features of hematologic malignancies may genetically matched to the patient’s immune type, make them particularly amenable to immunother- whereas the latter is more flexible in this regard and apy, including the fact that they are derived from has proved most successful. corrupt immune cells and come into constant con- CARs are formed by fusing part of the single- tact with other immune cells within the hemato- chain variable fragment of a monoclonal antibody poietic environment in which they reside. -

Novel Approaches to Improve Myeloma Cell Killing by Monoclonal Antibodies
Journal of Clinical Medicine Review Novel Approaches to Improve Myeloma Cell Killing by Monoclonal Antibodies Paola Storti 1,* , Federica Costa 1, Valentina Marchica 1, Jessica Burroughs-Garcia 1,2, Benedetta dalla Palma 1, Denise Toscani 1, Rosa Alba Eufemiese 1 and Nicola Giuliani 1 1 Department of Medicine and Surgery, University of Parma, 43126 Parma, Italy; [email protected] (F.C.); [email protected] (V.M.); [email protected] (J.B.-G.); [email protected] (B.d.P.); [email protected] (D.T.); [email protected] (R.A.E.); [email protected] (N.G.) 2 Department of Medical-Veterinary Science, University of Parma, 43126 Parma, Italy * Correspondence: [email protected]; Tel.: +39-0521-033303 Received: 11 August 2020; Accepted: 31 August 2020; Published: 4 September 2020 Abstract: The monoclonal antibodies (mAbs) have significantly changed the treatment of multiple myeloma (MM) patients. However, despite their introduction, MM remains an incurable disease. The mAbs currently used for MM treatment were developed with different mechanisms of action able to target antigens, such as cluster of differentiation 38 (CD38) and SLAM family member 7 (SLAMF7) expressed by both, MM cells and the immune microenvironment cells. In this review, we focused on the mechanisms of action of the main mAbs approved for the therapy of MM, and on the possible novel approaches to improve MM cell killing by mAbs. Actually, the combination of anti-CD38 or anti-SLAMF7 mAbs with the immunomodulatory drugs significantly improved the clinical effect in MM patients. On the other hand, pre-clinical evidence indicates that different approaches may increase the efficacy of mAbs. -
Sarclisa, INN-Isatuximab
25 February 2021 EMA/CHMP/186236/2021 Committee for Medicinal Products for Human Use (CHMP) Assessment report SARCLISA International non-proprietary name: isatuximab Procedure No. EMEA/H/C/004977/II/0003 Note Variation assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union Table of contents 1. Background information on the procedure .............................................. 6 1.1. Type II variation .................................................................................................. 6 1.2. Steps taken for the assessment of the product ........................................................ 6 2. Scientific discussion ................................................................................ 7 2.1. Introduction ........................................................................................................ 7 2.1.1. Problem statement ............................................................................................ 7 2.1.2. About the product ............................................................................................. 9 2.1.3. The development programme/compliance with CHMP guidance/scientific advice ...... 10 2.1.4. General comments on compliance with GCP ....................................................... -

Chemotherapy: Drugs E-O Policy (Chemo Drug E-O)
chemo drug e-o 1 Chemotherapy: Drugs E-O Policy Page updated: September 2020 This section contains policy related to billing for injection services, listed in alphabetical order by generic drug name or drug type. For general billing policy information regarding injections services, refer to the Chemotherapy: An Overview section in this manual. Additional policy information for chemotherapy drug services can be found in the Chemotherapy: Drugs A-D Policy and Chemotherapy: Drugs P-Z Policy sections in this manual. Elotuzumab Elotuzumab is a humanized IgG1 monoclonal antibody that specifically targets the SLAMF7 (signaling lymphocytic activation molecule family member 7) protein. SLAMF7 is expressed on myeloma cells independent of cytogenetic abnormalities. SLAMF7 is also expressed on natural killer cells, plasma cells and at lower levels on specific immune cell subsets of differentiated cells within the hematopoietic lineage. Elotuzumab directly activates natural killer cells through both the SLAMF7 pathway and Fc receptors. Elotuzumab also targets SLAMF7 on myeloma cells and facilitates the interaction with natural killer cells to mediate the killing of myeloma cells through antibody-dependent cellular cytotoxicity (ADCC). Indications Elotuzumab is indicated in combination with lenalidomide and dexamethasone for the treatment of patients ages 18 years or older, with multiple myeloma who have received one to three prior therapies. Pre-medicate with dexamethasone, diphenhydramine, ranitidine and acetaminophen. Advise patients that lenalidomide has the potential to cause fetal harm. Authorization An approved Treatment Authorization Request (TAR) is required for reimbursement. The TAR must state that the treatment is for a patient with multiple myeloma who has received one to three prior therapies.