Vision Test Report (MV-619)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
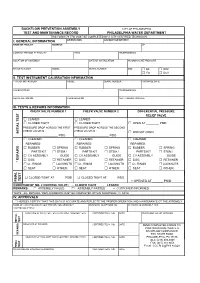
BFP Test Form
BACKFLOW PREVENTION ASSEMBLY CITY OF PHILADELPHIA TEST AND MAINTENANCE RECORD PHILADELPHIA WATER DEPARTMENT THIS FORM (79-770) MUST BE COMPLETED BY A CITY CERTIFIED TECHNICIAN I. GENERAL INFORMATION ORIENTATION ACCOUNT OR METER # NAME OF FACILITY ADDRESS ZIP CONTACT PERSON AT FACILITY TITLE TELEPHONE NO. LOCATION OF ASSEMBLY DATE OF INSTALLATION INCOMING LINE PRESSURE MANUFACTURER MODEL SERIAL NUMBER SIZE □ DS □ RPZ □ FS □ DCV II. TEST INSTRUMENT CALIBRATION INFORMATION TYPE OF INSTRUMENT MODEL SERIAL NUMBER PURCHASE DATE CALIBRATED BY TELEPHONE NO. REGISTRATION NO. CALIBRATED ON NEXT CALIBRATION DUE III. TESTS & REPAIRS INFORMATION CHECK VALVE NUMBER 1 CHECK VALVE NUMBER 2 DIFFERENTIAL PRESSURE RELIEF VALVE □ LEAKED □ LEAKED □ CLOSED TIGHT □ CLOSED TIGHT □ OPEN AT ________ PSID PRESSURE DROP ACROSS THE FIRST PRESSURE DROP ACROSS THE SECOND CHECK VALVE IS : CHECK VALVE IS : INITIAL TEST INITIAL □ DID NOT OPEN ______________________ PSID ______________________ PSID □ CLEANED □ CLEANED □ CLEANED REPAIRED: REPAIRED: REPAIRED: □ RUBBER □ SPRING □ RUBBER □ SPRING □ RUBBER □ SPRING PARTS KIT □ STEM / PARTS KIT □ STEM / PARTS KIT □ STEM / □ CV ASSEMBLY GUIDE □ CV ASSEMBLY GUIDE □ CV ASSEMBLY GUIDE □ DISC □ RETAINER □ DISC □ RETAINER □ DISC □ RETAINER * REPAIRS □ O - RINGS □ LOCKNUTS □ O - RINGS □ LOCKNUTS □ O - RINGS □ LOCKNUTS □ SEAT □ OTHER: □ SEAT □ OTHER: □ SEAT □ OTHER: □ CLOSED TIGHT AT ______ PSID □ CLOSED TIGHT AT ______ PSID TEST FINAL FINAL □ OPENED AT ______ PSID CONDITION OF NO. 2 CONTROL VALVE : □ CLOSED TIGHT □ LEAKED REMARKS : □ ASSEMBLY FAILED □ ASSEMBLY PASSED □ CUSTOMER INFORMED *NOTE : ALL REPAIRS / REPLACEMENTS MUST BE COMPLETED WITHIN FOURTEEN (14) DAYS IV. APPROVALS * I HEREBY CERTIFY THAT THIS DATA IS ACCURATE AND REFLECTS THE PROPER OPERATION AND MAINTENANCE OT THE ASSEMBLY NAME OF CERTIFIED BACKFLOW PREVENTION ASSEMBLY BUSINESS TELEPHONE NO. -
A Brief Introduction to Unix-2019-AMS
Brief Intro to Linux/Unix Brief Intro to Unix (contd) A Brief Introduction to o Brief History of Unix o Compilers, Email, Text processing o Basics of a Unix session o Image Processing Linux/Unix – AMS 2019 o The Unix File System Pete Pokrandt o Working with Files and Directories o The vi editor UW-Madison AOS Systems Administrator o Your Environment [email protected] o Common Commands Twitter @PTH1 History of Unix History of Unix History of Unix o Created in 1969 by Kenneth Thompson and Dennis o Today – two main variants, but blended o It’s been around for a long time Ritchie at AT&T o Revised in-house until first public release 1977 o System V (Sun Solaris, SGI, Dec OSF1, AIX, o It was written by computer programmers for o 1977 – UC-Berkeley – Berkeley Software Distribution (BSD) linux) computer programmers o 1983 – Sun Workstations produced a Unix Workstation o BSD (Old SunOS, linux, Mac OSX/MacOS) o Case sensitive, mostly lowercase o AT&T unix -> System V abbreviations 1 Basics of a Unix Login Session Basics of a Unix Login Session Basics of a Unix Login Session o The Shell – the command line interface, o Features provided by the shell o Logging in to a unix session where you enter commands, etc n Create an environment that meets your needs n login: username n Some common shells n Write shell scripts (batch files) n password: tImpAw$ n Define command aliases (this Is my password At work $) Bourne Shell (sh) OR n Manipulate command history IHateHaving2changeMypasswordevery3weeks!!! C Shell (csh) n Automatically complete the command -

Georgia Department of Revenue
Form MV-9W (Rev. 6-2015) Web and MV Manual Georgia Department of Revenue - Motor Vehicle Division Request for Manufacture of a Special Veteran License Plate ______________________________________________________________________________________ Purpose of this Form: This form is to be used to apply for a military license plate/tag. This form should not be used to record a change of ownership, change of address, or change of license plate classification. Required documentation: You must provide a legible copy of your service discharge (DD-214, DD-215, or for World War II veterans, a WD form) indicating your branch and term of service. If you are an active duty member, a copy of the approved documentation supporting your current membership in the respective reserve or National Guard unit is required. In the case of a retired reserve member from that unit, you must furnish approved documentation supporting the current retired membership status from that reserve unit. OWNER INFORMATION First Name Middle Initial Last Name Suffix Owners’ Full Legal Name: Mailing Address: City: State: Zip: Telephone Number: Owner(s)’ Full Legal Name: First Name Middle Initial Last Name Suffix If secondary Owner(s) are listed Mailing Address: City: State: Zip: Telephone Number: VEHICLE INFORMATION Passenger Vehicle Motorcycle Private Truck Vehicle Identification Number (VIN): Year: Make: Model: CAMPAIGN/TOUR of DUTY Branch of Service: SERVICE AWARD Branch of Service: LICENSE PLATES ______________________ LICENSE PLATES ______________________ World War I World -

The Linux Command Line
The Linux Command Line Fifth Internet Edition William Shotts A LinuxCommand.org Book Copyright ©2008-2019, William E. Shotts, Jr. This work is licensed under the Creative Commons Attribution-Noncommercial-No De- rivative Works 3.0 United States License. To view a copy of this license, visit the link above or send a letter to Creative Commons, PO Box 1866, Mountain View, CA 94042. A version of this book is also available in printed form, published by No Starch Press. Copies may be purchased wherever fine books are sold. No Starch Press also offers elec- tronic formats for popular e-readers. They can be reached at: https://www.nostarch.com. Linux® is the registered trademark of Linus Torvalds. All other trademarks belong to their respective owners. This book is part of the LinuxCommand.org project, a site for Linux education and advo- cacy devoted to helping users of legacy operating systems migrate into the future. You may contact the LinuxCommand.org project at http://linuxcommand.org. Release History Version Date Description 19.01A January 28, 2019 Fifth Internet Edition (Corrected TOC) 19.01 January 17, 2019 Fifth Internet Edition. 17.10 October 19, 2017 Fourth Internet Edition. 16.07 July 28, 2016 Third Internet Edition. 13.07 July 6, 2013 Second Internet Edition. 09.12 December 14, 2009 First Internet Edition. Table of Contents Introduction....................................................................................................xvi Why Use the Command Line?......................................................................................xvi -
File Permissions Do Not Restrict Root
Filesystem Security 1 General Principles • Files and folders are managed • A file handle provides an by the operating system opaque identifier for a • Applications, including shells, file/folder access files through an API • File operations • Access control entry (ACE) – Open file: returns file handle – Allow/deny a certain type of – Read/write/execute file access to a file/folder by – Close file: invalidates file user/group handle • Access control list (ACL) • Hierarchical file organization – Collection of ACEs for a – Tree (Windows) file/folder – DAG (Linux) 2 Discretionary Access Control (DAC) • Users can protect what they own – The owner may grant access to others – The owner may define the type of access (read/write/execute) given to others • DAC is the standard model used in operating systems • Mandatory Access Control (MAC) – Alternative model not covered in this lecture – Multiple levels of security for users and documents – Read down and write up principles 3 Closed vs. Open Policy Closed policy Open Policy – Also called “default secure” • Deny Tom read access to “foo” • Give Tom read access to “foo” • Deny Bob r/w access to “bar” • Give Bob r/w access to “bar • Tom: I would like to read “foo” • Tom: I would like to read “foo” – Access denied – Access allowed • Tom: I would like to read “bar” • Tom: I would like to read “bar” – Access allowed – Access denied 4 Closed Policy with Negative Authorizations and Deny Priority • Give Tom r/w access to “bar” • Deny Tom write access to “bar” • Tom: I would like to read “bar” – Access -

Student Number: Surname: Given Name
Computer Science 2211a Midterm Examination Sample Solutions 9 November 20XX 1 hour 40 minutes Student Number: Surname: Given name: Instructions/Notes: The examination has 35 questions on 9 pages, and a total of 110 marks. Put all answers on the question paper. This is a closed book exam. NO ELECTRONIC DEVICES OF ANY KIND ARE ALLOWED. 1. [4 marks] Which of the following Unix commands/utilities are filters? Correct answers are in blue. mkdir cd nl passwd grep cat chmod scriptfix mv 2. [1 mark] The Unix command echo HOME will print the contents of the environment variable whose name is HOME. True False 3. [1 mark] In C, the null character is another name for the null pointer. True False 4. [3 marks] The protection code for the file abc.dat is currently –rwxr--r-- . The command chmod a=x abc.dat is equivalent to the command: a. chmod 755 abc.dat b. chmod 711 abc.dat c. chmod 155 abc.dat d. chmod 111 abc.dat e. none of the above 5. [3 marks] The protection code for the file abc.dat is currently –rwxr--r-- . The command chmod ug+w abc.dat is equivalent to the command: a. chmod 766 abc.dat b. chmod 764 abc.dat c. chmod 754 abc.dat d. chmod 222 abc.dat e. none of the above 2 6. [3 marks] The protection code for def.dat is currently dr-xr--r-- , and the protection code for def.dat/ghi.dat is currently -r-xr--r-- . Give one or more chmod commands that will set the protections properly so that the owner of the two files will be able to delete ghi.dat using the command rm def.dat/ghi.dat chmod u+w def.dat or chmod –r u+w def.dat 7. -
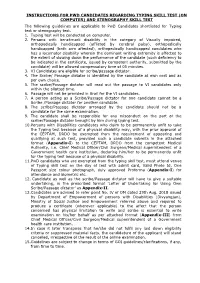
Instructions for Pwd Candidates Regarding Typing Skill Test
INSTRUCTIONS FOR PWD CANDIDATES REGARDING TYPING SKILL TEST (ON COMPUTER) AND STENOGRAPHY SKILL TEST The following guidelines are applicable to PwD Candidates shortlisted for Typing test or stenography test. 1. Typing test will be conducted on computer. 2. Persons with benchmark disability in the category of Visually impaired, orthopedically handicapped (afflicted by cerebral palsy), orthopedically handicapped (both arm affected), orthopedically handicapped candidates who has a locomotor disability wherein the dominant writing extremity is affected to the extent of slowing down the performance of the candidate (such deficiency to be indicated in the certificate, issued by competent authority, submitted by the candidate) will be allowed compensatory time of 05 minutes. 3. VI Candidates are eligible for scribe/passage dictator. 4. The Scribe/ Passage dictator is identified by the candidate at own cost and as per own choice. 5. The scribe/Passage dictator will read out the passage to VI candidates only within the allotted time. 6. Passage will not be provided in Brail for the VI candidates. 7. A person acting as a Scribe/Passage dictator for one candidate cannot be a Scribe /Passage dictator for another candidate. 8. The scribe/Passage dictator arranged by the candidate should not be a candidate for the same examination. 9. The candidate shall be responsible for any misconduct on the part of the scribe/Passage dictator brought by him during typing test. 10.Persons with Disabilities candidates who claim to be permanently unfit to take the Typing test because of a physical disability may, with the prior approval of the CEPTAM, DRDO be exempted from the requirement of appearing and qualifying at such test, provided such a candidate submits in the attached format (Appendix-I) to the CEPTAM, DRDO from the competent Medical Authority, i.e. -
Pingdirectory Administration Guide Version
Release 7.3.0.3 Server Administration Guide PingDirectory | Contents | ii Contents PingDirectory™ Product Documentation................................................ 20 Overview of the Server............................................................................. 20 Server Features.................................................................................................................................20 Administration Framework.................................................................................................................21 Server Tools Location....................................................................................................................... 22 Preparing Your Environment....................................................................22 Before You Begin.............................................................................................................................. 22 System requirements..............................................................................................................22 Installing Java......................................................................................................................... 23 Preparing the Operating System (Linux).......................................................................................... 24 Configuring the File Descriptor Limits.................................................................................... 24 File System Tuning.................................................................................................................25 -

Unix (And Linux)
AWK....................................................................................................................................4 BC .....................................................................................................................................11 CHGRP .............................................................................................................................16 CHMOD.............................................................................................................................19 CHOWN ............................................................................................................................26 CP .....................................................................................................................................29 CRON................................................................................................................................34 CSH...................................................................................................................................36 CUT...................................................................................................................................71 DATE ................................................................................................................................75 DF .....................................................................................................................................79 DIFF ..................................................................................................................................84 -

5 Command Line Functions by Barbara C
ADAPS: Chapter 5. Command Line Functions 5 Command Line Functions by Barbara C. Hoopes and James F. Cornwall This chapter describes ADAPS command line functions. These are functions that are executed from the UNIX command line instead of from ADAPS menus, and that may be run manually or by automated means such as “cron” jobs. Most of these functions are NOT accessible from the ADAPS menus. These command line functions are described in detail below. 5.1 Hydra Although Hydra is available from ADAPS at the PR sub-menu, Edit Time Series Data using Hydra (TS_EDIT), it can also be started from the command line. However, to start Hydra outside of ADAPS, a DV or UV RDB file needs to be available to edit. The command is “hydra rdb_file_name.” For a complete description of using Hydra, refer to Section 4.5.2 Edit Time-Series Data using Hydra (TS_EDIT). 5.2 nwrt2rdb This command is used to output rating information in RDB format. It writes RDB files with a table containing the rating equation parameters or the rating point pairs, with all other information contained in the RDB comments. The following arguments can be used with this command: nwrt2rdb -ooutfile -zdbnum -aagency -nstation -dddid -trating_type -irating_id -e (indicates to output ratings in expanded form; it is ignored for equation ratings.) -l loctzcd (time zone code or local time code "LOC") -m (indicates multiple output files.) -r (rounding suppression) Rules • If -o is omitted, nwrt2rdb writes to stdout; AND arguments -n, -d, -t, and -i must be present. • If -o is present, no other arguments are required, and the program will use ADAPS routines to prompt for them. -
Install and Run External Command Line Softwares
job monitor and control top: similar to windows task manager (space to refresh, q to exit) w: who is there ps: all running processes, PID, status, type ps -ef | grep yyin bg: move current process to background fg: move current process to foreground jobs: list running and suspended processes kill: kill processes kill pid (could find out using top or ps) 1 sort, cut, uniq, join, paste, sed, grep, awk, wc, diff, comm, cat All types of bioinformatics sequence analyses are essentially text processing. Unix Shell has the above commands that are very useful for processing texts and also allows the output from one command to be passed to another command as input using pipe (“|”). less cosmicRaw.txt | cut -f2,3,4,5,8,13 | awk '$5==22' | cut -f1 | sort -u | wc This makes the processing of files using Shell very convenient and very powerful: you do not need to write output to intermediate files or load all data into the memory. For example, combining different Unix commands for text processing is like passing an item through a manufacturing pipeline when you only care about the final product 2 Hands on example 1: cosmic mutation data - Go to UCSC genome browser website: http://genome.ucsc.edu/ - On the left, find the Downloads link - Click on Human - Click on Annotation database - Ctrl+f and then search “cosmic” - On “cosmic.txt.gz” right-click -> copy link address - Go to the terminal and wget the above link (middle click or Shift+Insert to paste what you copied) - Similarly, download the “cosmicRaw.txt.gz” file - Under your home, create a folder -

Manipulating Files and Directories
MANIPULATING FILES AND DIRECTORIES At this point, we are ready for some real work! This chapter will introduce the following commands: z cp—Copy files and directories. z mv—Move/rename files and directories. z mkdir—Create directories. z rm—Remove files and directories. z ln—Create hard and symbolic links. These five commands are among the most frequently used Linux com- mands. They are used for manipulating both files and directories. Now, to be frank, some of the tasks performed by these commands are more easily done with a graphical file manager. With a file manager, we can drag and drop a file from one directory to another, cut and paste files, delete files, and so on. So why use these old command-line programs? www.it-ebooks.info The answer is power and flexibility. While it is easy to perform simple file manipulations with a graphical file manager, complicated tasks can be easier with the command-line programs. For example, how could we copy all the HTML files from one directory to another—but only those that do not exist in the destination directory or are newer than the versions in the destination directory? Pretty hard with a file manager. Pretty easy with the command line: cp -u *.html destination Wildcards Before we begin using our commands, we need to talk about the shell fea- ture that makes these commands so powerful. Because the shell uses file- names so much, it provides special characters to help you rapidly specify groups of filenames. These special characters are called wildcards.