Hip Arthroscopy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Baseball Classics All-Time All-Star Greats Game Team Roster
BASEBALL CLASSICS® ALL-TIME ALL-STAR GREATS GAME TEAM ROSTER Baseball Classics has carefully analyzed and selected the top 400 Major League Baseball players voted to the All-Star team since it's inception in 1933. Incredibly, a total of 20 Cy Young or MVP winners were not voted to the All-Star team, but Baseball Classics included them in this amazing set for you to play. This rare collection of hand-selected superstars player cards are from the finest All-Star season to battle head-to-head across eras featuring 249 position players and 151 pitchers spanning 1933 to 2018! Enjoy endless hours of next generation MLB board game play managing these legendary ballplayers with color-coded player ratings based on years of time-tested algorithms to ensure they perform as they did in their careers. Enjoy Fast, Easy, & Statistically Accurate Baseball Classics next generation game play! Top 400 MLB All-Time All-Star Greats 1933 to present! Season/Team Player Season/Team Player Season/Team Player Season/Team Player 1933 Cincinnati Reds Chick Hafey 1942 St. Louis Cardinals Mort Cooper 1957 Milwaukee Braves Warren Spahn 1969 New York Mets Cleon Jones 1933 New York Giants Carl Hubbell 1942 St. Louis Cardinals Enos Slaughter 1957 Washington Senators Roy Sievers 1969 Oakland Athletics Reggie Jackson 1933 New York Yankees Babe Ruth 1943 New York Yankees Spud Chandler 1958 Boston Red Sox Jackie Jensen 1969 Pittsburgh Pirates Matty Alou 1933 New York Yankees Tony Lazzeri 1944 Boston Red Sox Bobby Doerr 1958 Chicago Cubs Ernie Banks 1969 San Francisco Giants Willie McCovey 1933 Philadelphia Athletics Jimmie Foxx 1944 St. -

Heroes of the 5544 2008 Championship Jimmy Rollins Carlos Ruiz
N4 FRIDAY, OCTOBER 31, 2008 THE MORNING CALL FRIDAY, OCTOBER 31, 2008 N5 YO, PHILLY! WE DID IT! 1111 2288 2266 6 5 8 JIMMY ROLLINS • SS JAYSON WERTH • RF CHASE UTLEY • 2B RYAN HOWARD • 1B PAT BURRELL • LF SHANE VICTORINO • CF 1199 HEROES OF THE 5544 2008 CHAMPIONSHIP JIMMY ROLLINS CARLOS RUIZ In Game 161 of the regular season, he started an acrobatic 6-4-3 double play on Ryan After a dismal regular season at the plate, he was a lifeline for the Phillies in the postseason. In Zimmerman’s bases-loaded ground ball that looked like it was destined for center fi eld. The the fi rst three World Series games, he was 4-for-8 with four walks and a team-best three extra- twin-killing preserved the Phils’ 4-3 win over the Washington Nationals and gave the Phils their base hits (two doubles and a home run). In fi ve NLCS games and the opening three World Series second consecutive NL East Division title. Then after going 0-for-10 in the fi rst two games of games, hit .360. the World Series, was 5-for-9 and scored four runs in Games 3 and 4. JAMIE MOYER JAYSON WERTH Led the Phillies in regular-season wins (16). Although he got a no-decision, pitched well in GREG DOBBS • PH/3B Worked his way out of a platoon role and into the starting lineup just past the halfway part of Game 3 of the World Series, giving up just three runs, fi ve hits and one walk in 6 1/3 innings. -

2013BB Pages 62-122.Indd
1940 UCLA Baseball Jackie Robinson spent the 1940 season playing baseball at UCLA. Robinson (far left, top row) played his first game on March 10, 1940. He finished his career at UCLA as the school’s first four-sport letterwinner (baseball, football, basketball, track and field). Gary Adams UCLA’s all-time winningest head coach (below, center), Gary Adams led the Bruins to the 1997 College World Series. That season, UCLA overcame an early loss in NCAA Regional action by winning its next five games in dominating fashion. Adams played at UCLA from 1959-62. Bob Andrews Playing under head coach Art Reichle, Paul Ellis Bob Andrews pitched for UCLA from Shown here being congratulated by his teammtes, 1948-50 when the Bruins were Paul Ellis (#19) served as the Bruins’ starting members of the CIBA. catcher in 1989 and 1990. He was a consensus first-team All-America selection and Diviion I ABCA Player of the Year honoree in 1990. 2010 UCLA Baseball The Bruins posted a program-best 51-17 record in 2010, closing the season with UCLA’s first-ever trip to the finals of the College World Series in Omaha, Neb. Anchored by starting pitchers Gerrit Cole, Trevor Bauer and Rob Rasmussen, the Bruins took down Cal State Fullerton in the Super Regionals to advance to the College World Series. 2012 UCLA Baseball Dan Guerrero Jim Parque Led by the winningest junior class in school history, the An infielder on UCLA’s baseball team from Among the top pitchers in the nation in 2012 UCLA Baseball team advanced to their second 1971-73, Guerrero has served as UCLA’s 1997, Parque posted a career 25-11 record with a 3.55 ERA College World Series in three years. -

Hand Signed Sports Memorabilia from Around the U.S
NNNorthN America’s Charity Fundraising “One Stop Shop” BW Unlimited is proud to provide this incredible list of hand signed Sports Memorabilia from around the U.S. All of these items come complete with a Certificate of Authenticity (COA) from a 3rd Party Authenticator. From Signed Full Size Helmets, Jersey’s, Balls and Photo’s…you can find everything you could possibly ever want. Please keep in mind that our vast inventory constantly changes and each item is subject to availability. When speaking to your Charity Fundraising Representative, let them know which items you would like in your next Charity Fundraising Event: Hand Signed Sports Memorabilia BALTIMORE RAVENS 1. Jacoby Jones Signed/Autographed Baltimore Ravens 16x20 Photo JSA (BWU001IS) $175 2. Jacoby Jones Signed Baltimore Ravens 16x20 Sports Illustrated Photo JSA (BWU001IS) $175 3. Ray Lewis Signed Ravens Super Bowl Full Size Helmet Raven For Life JSA (BWU001IS) $388 4. Ray Lewis Signed Ravens Super Bowl Full Size Helmet SB XLVII Champs JSA W432086 (BWU001IS) $388 5. Autographed Ray Lewis NFL Football (BWU001EPA) $300.00 6. Terrell Suggs Signed/Autographed Pro Style Black Jersey JSA W390362 (BWU001IS) $244 7. Terrell Suggs Signed/Autographed Pro Style Purple Jersey JSA W390338 (BWU001IS) $244 8. Terrell Suggs Signed Pro Style White Jersey SB XLVII Champs JSA (BWU001IS) $269 9. Terrell Suggs Signed/Autographed Arizona State Jersey JSA (BWU001IS) $261 10. Terrell Suggs Signed Baltimore Ravens Super Bowl Mini Helmet JSA W390272 (BWU001IS) $184 11. Terrell Suggs Signed Baltimore Ravens SMOKE 16x20 Photo JSA (BWU001IS) $210 12. Terrell Suggs Signed Baltimore Ravens 16x20 SB XLVII Celebration Photo JSA (BWU001IS) $210 13. -

PHILADELPHIA PHILLIES (60-72) Vs
PHILADELPHIA PHILLIES (60-72) vs. NEW YORK METS (59-71) Wednesday, August 28, 2013 – Citi Field – 7:10 p.m. EDT – Game 133; Road 67 LHP Cole Hamels (5-13, 3.62) vs. RHP Daisuke Matsuzaka (0-1, 9.00) LAST NIGHT’S ACTION: The Phillies were shut out by the New York Mets, 5-0, at Citi Field ... PHILLIES PHACTS Starter Kyle Kendrick (10-11) allowed 5 runs (1 ER) over 6.0 innings for the loss ... Opposing starter Jonathon Niese tossed a complete game shutout ... The Phillies managed just 3 hits and 4 total Record (2013): 60-72 (.455) Home (2013): 35-31 baserunners in the game, only one of which reached 2nd base (Michael Young, leadoff double in the 8th rd Road (2013): 25-41 inning) ... The Mets scored 1 run in the 3 inning on an RBI single by Daniel Murphy ... They plated 4 Current Streak: Lost 1 th runs in the 6 inning, all of which were unearned ... A throwing error by Kevin Frandsen put runners Last 5 Games: 3-2 on 2nd and 3rd with nobody out ... Travis d’Arnaud then hit a sac fly before Niese hit a 2-out, bases- Last 10 Games: 7-3 clearing double ... Zach Miner and Justin De Fratus each threw 1.0 scoreless relief inning in a game Series Record/# of series: 16-20-6 that lasted just 2 hours and 19 minutes. Sweeps/Swept: 1/6 ELIAS SAYS: Jonathon Niese threw a three-hit shutout and drove in three runs with a bases-loaded PHILLIES VS. -

Batting Order
Fantistics Projected MLB Lineups ( updated 7/30/06 ) Roto-accurate projections by LYLE (the AX cuts deep) LOGAN National League National East Atlanta Florida NY Mets Philadelphia Washington 1 Marcus Giles 2B 1 Am'z'ga//H R'mirez cf/ss 1 Jose Reyes SS 1 Jimmy Rollins SS 1 Alfonso Soriano LF 2 Edgar Renteria SS 2 H Ramirez//Uggla ss/2b 2 Paul Lo Duca C 2 Chase Utley 2B 2 Felipe Lopez SS 3 McCann//Frncoeur c/rf 3 Miguel Cabrera 3B 3 Carlos Beltran CF 3 Bobby Abreu RF 3 Ryan Zimmerman 3B 4 Andruw Jones CF 4 Jacobs//C Ross 1b/cf 4 Carlos Delgado 1B 4 Pat Burrell LF 4 Nick Johnson 1B 5 LaRoche//M Diaz 1b/lf 5 Uggla//Wllngham 2b/lf 5 David Wright 3B 5 Ryan Howard 1B 5 Austin Kearns RF 6 Frncoeur//McCann rf/c 6 Hermida//Helms rf/1b 6 Cliff Floyd LF 6 Aaron Rowand CF 6 Marlon Anderson 2B 7 Willy Aybar 3B 7 Wllnghm//H'rmida lf/rf 7 Jo Valentin//Nady 2b/rf 7 Abraham Nunez 3B 7 Church//Matos CF 8 Lngrhns//L'Roche lf/1b 8 Miguel Olivo C 8 Nady//Jo Valentin rf/2b 8 Mike Lieberthal C 8 Schneider//Fick C 9 PITCHER 9 PITCHER 9 PITCHER 9 PITCHER 9 PITCHER bench & DL bench & DL bench & DL bench & DL bench & DL Chipper Jones reg 3B Joe Borchard of Chris Woodward inf David Dellucci of Jose Vidro reg 2B Scott Thorman of/1b Reg. Abercrombie of Endy Chavez of Shane Victorino of Damian Jackson util Pete Orr util Matt Treanor c Eli Marrero util Danny Sandoval inf Alex Escobar of Todd Pratt c Ramon Castro c Chris Coste c Daryle Ward of/1b National Central Chi Cubs Cincinnati Houston Milwaukee Pittsburgh St Louis 1 Juan Pierre CF 1 Ryan Freel RF 1 Craig Biggio 2B -

The Chase Utley Question: a Controversial Collision Between Tort Law and Professional Sports
CORE Metadata, citation and similar papers at core.ac.uk Provided by St. John's University School of Law St. John's Law Review Volume 90 Number 3 Volume 90, Fall 2016, Number 3 Article 10 March 2017 The Chase Utley Question: A Controversial Collision Between Tort Law and Professional Sports Kaitlin Decker Follow this and additional works at: https://scholarship.law.stjohns.edu/lawreview Recommended Citation Kaitlin Decker (2016) "The Chase Utley Question: A Controversial Collision Between Tort Law and Professional Sports," St. John's Law Review: Vol. 90 : No. 3 , Article 10. Available at: https://scholarship.law.stjohns.edu/lawreview/vol90/iss3/10 This Note is brought to you for free and open access by the Journals at St. John's Law Scholarship Repository. It has been accepted for inclusion in St. John's Law Review by an authorized editor of St. John's Law Scholarship Repository. For more information, please contact [email protected]. FINAL_DECKER 2/23/2017 5:10 PM NOTES THE CHASE UTLEY QUESTION: A CONTROVERSIAL COLLISION BETWEEN TORT LAW AND PROFESSIONAL SPORTS KAITLIN DECKER† INTRODUCTION The slide was late. The slide was high. The slide was questionably legal and arguably dirty. 1 It happened on a Saturday night in October, just outside downtown Los Angeles. The lights were bright, the crowds deafening, the atmosphere electric. It was Game 2 of the National League Division Series between the Los Angeles Dodgers and the New York Mets. The Dodgers, touting one of baseball’s largest payrolls, were aiming to prove that the franchise was capable of finally making it deep in the playoffs. -

Cheap Nike Shoes for Sale with All Sizes Available for Your Selection
Buy Cheap Jordan | Air Max | Free Run Shoes on Nike Wholesale Online Store.--Cheap Nike Shoes For Sale with all sizes available for your selection. Enjoy 30 days return policy, Get 7*24 online support! Jordan 93 Reviews - Online Shopping Jordan 93 Reviews on Aliexpress.com | Alibaba Group--Read Jordan 93 Reviews and Customer Ratings on Jordan 93 Reviews, Reviews and more at Aliexpress.com. Buy Cheap Jordan 93 Now. LANDOVER,new nfl nike jerseys, Md. -- A not many thoughts all around the going to be the Washington Redskins' victory Sunday exceeding going to be the Arizona Cardinals: What a resource box means: That going to be the Redskins are in before anything else place,just as everyone expected they'd be Seriously, Washington is the reason that 2-0 going into its let me give you road game concerning going to be the year and he or she utilize them and achieve at their store allowing an individual a multi function strong running game and an inspired-looking criminal There was a multi function parcel and for going to be the Redskins to explore overcome for game,new nfl jersey,so that you have quarterback Rex Grossman throwing two ahead of due date interceptions and going to be the missed opportunities piling entirely all the way through going to be the preparing any other part half. And and then for many years a resource box looked a little as though going to be the with safety in mind of game going to be the Redskins have become that can be used to educate yourself regarding losing at least going to be the past couple to do with some time Instead, it's an all in one tough, feel-good win piggybacked throughout the last week's season-opening victory in excess of going to be the rival Giants. -

Letter to the Editor: Chase Utley Will Be Missed by Phillies Fans, and Animal Lovers, Too
The Delaware County Daily Times (http://www.delcotimes.com) Letter to the Editor: Chase Utley will be missed by Phillies fans, and animal lovers, too By Rich Westcott, Times Guest Columnist Friday, August 21, 2015 Some time ago, my wife and I adopted a dog that was badly in need of a new home. The previous owners, having purchased the pedigreed dog for a large chunk of money, had for some unfathomable reason turned to abusing the lovely creature. After they were finally persuaded to let her go, we became the lucky owners. This was by no means the first dog we’d ever rescued. Nor was it the last. But there was one thing about this youngster that we’d never experienced before. It had a computer chip, which identified its owner, imbedded in its neck. Perhaps as dog people we should’ve been more knowledgeable about such things. But we’d never had a dog with a computer chip, and we had no idea how to access the information. Then, along came Chase Utley. Utley and I had had a variety of conversations over the years, mostly when I was seeking information or his opinion for whatever book I was writing at the time. Although a quiet person who was never too talkative, Chase was always very cooperative and for me, it was always a valuable interview. But sometimes, we also talked about one of our favorite subjects — dogs. A pet owner himself, Utley and his wife, Jennifer, were heavily involved in raising funds for the Pennsylvania SPCA, and over the years had raised more than $1 million for that and other pet-rescue organizations. -

The Best Phillie Whose Last Name B
Each night on my 94WIP show, in alphabetical order, we will try to come up with (for example) the best Phillie whose last name begins with "A" going up against the best Met whose last name begins with the letter "A." Remember, all that counts is how that player performed with his Philly or NY team. What they did with other teams counts for NOTHING. Here's what we have so far. (BTW, what's it say when WE have R-Diddy representing us and The Donald repping NY?) A Richie Ashburn vs Tommy Agee (Winner!) Eric Allen vs Jesse Armstead (Winner!) Carmello Anthony Ron Anderson vs (Winner!) Barry Ashbee vs Tony Amonte (Winner!) B Jim Bunning vs Carlos Beltran (Winner!) Chuck Bednarik vs Tiki Barber (Winner!) Charles Barkley vs Bill Bradley (Winner!) Bill Barber vs Andy Bathgate (Winner!) C Steve Carlton vs Gary Carter (Winner!) Harry Carson Harold Carmichael vs (Winner!) Wilt Chamberlain vs Bill Cartwright (Winner!) Bobby Clarke vs Neil Coville (Winner!) D Ed Delaehanty vs Ron Darling (Winner!) Brian Dawkins vs David Diehl (Winner!) Dave DeBusschere Darryl Dawkins vs (Winner!) Gary Dornhoffer vs Cecil Dillon (Winner!) E Del Ennis vs Kevin Elster (Winner!) Jumbo Elliot Herm Edwards vs (Winner!) Julius Erving vs Patrick Ewing (Winner!) Phil Esposito Pelle Eklund vs (Winner!) F Sid Fernandez Turk Farrell vs (Winner!) Irving Fryar vs Ray Flaherty (Winner!) Walt Frazier Lloyd (World B.) Free vs (Winner!) Bob Froese vs Bill Fairbairn (Winner!) G Dwight Gooden Tony Gonzalez vs (Winner!) Frank Gifford Mike Golic vs (Winner!) Hal Greer vs Richie Guerin (Winner!) -

Chase Utley, Ruben Tejada, and the Long History of the Mets Avenging Injustices by Eric Trager
MENU Policy Analysis / Articles & Op-Eds Chase Utley, Ruben Tejada, and the Long History of the Mets Avenging Injustices by Eric Trager Oct 1, 2015 ABOUT THE AUTHORS Eric Trager Eric Trager was the Esther K. Wagner Fellow at The Washington Institute. Articles & Testimony early 48 hours later, Mets fans are still reeling. Dodgers second baseman Chase Utley's filthy, far-to-the-right- N of-the-bag slide into Mets shortstop Ruben Tejada during Saturday night's playoff game ended Tejada's postseason and could end his career, while the umpires' boobish mishandling of the ruling on the field cost the Mets the game. So when the best-of-five series resumes in Flushing with Game 3 on Monday night, Mets fans will demand two things: redemption in the form of victory, and justice for Tejada in the form of a fastball right at Utley's backside (Utley himself has been suspended for two games but, with his appeal pending, is expected to play tonight). In sports mythology, these two things are linked. Every good sports fable foretells that the Mets will rally to avenge Utley's hit on Tejada, unite behind whichever pitcher plunks Utley (or some other unfortunate Dodger), and then destroy the Dodgers on sheer adrenaline. And that is precisely what would happen in a just world. But as Mets fans know quite well, the world is extremely unjust -- and justice has been elusive almost every time a Met has sought it. Take, for example, an incident during the Mets inaugural season in 1962, when Giants great Willie Mays spiked Mets shortstop Elio Chacon while sliding into second base. -
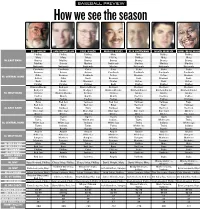
W6 Predictions.Indd
BASEBALL PREVIEW How we see the season BILL CONLIN SAM DONNELLON PAUL HAGEN MARCUS HAYES RISH HOFFMANN DAVID MURPHY JOHN SMALLWOOD Phillies Phillies Phillies Mets Mets Phillies Phillies Mets Mets Mets Phillies Phillies Mets Mets NL EAST RANK Braves Marlins Braves Braves Braves Braves Braves Marlins Braves Marlins Nationals Marlins Marlins Marlins Nationals Nationals Nationals Marlins Nationals Nationals Nationals Cardinals Cardinals Cubs Cubs Cubs Cubs Cubs Brewers Astros Astros Cardinals Cardinals Cardinals Cardinals Cubs Brewers Cardinals Astros Brewers Astros Brewers NL CENTRAL RANK Astros Cubs Reds Brewers Reds Brewers Reds Reds Reds Brewers Pirates Astros Reds Astros Pirates Pirates Pirates Reds Pirates Pirates Pirates Diamondbacks Dodgers Diamondbacks Dodgers Dodgers Dodgers Dodgers Dodgers Rockies Dodgers Diamondbacks Diamondbacks Diamondbacks Diamondbacks NL WEST RANK Rockies Diamondbacks Rockies Rockies Giants Giants Giants Padres Giants Giants Giants Rockies Rockies Padres Giants Padres Padres Padres Padres Padres Rockies Rays Red Sox Yankees Red Sox Yankees Yankees Rays Red Sox Rays Red Sox Rays Red Sox Rays Yankees AL EAST RANK Yankees Yankees Rays Yankees Rays Red Sox Red Sox Blue Jays Blue Jays Blue Jays Blue Jays Blue Jays Blue Jays Orioles Orioles Orioles Orioles Orioles Orioles Orioles Blue Jays Indians Tigers Tigers Tigers Indians Tigers Tigers Twins Twins White Sox Indians Tigers White Sox Twins AL CENTRAL RANK White Sox White Sox Indians White Sox Twins Indians White Sox Tigers Indians Twins Twins White Sox Twins Indians