Endometrial Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

Ovarian Cancer and Cervical Cancer
What Every Woman Should Know About Gynecologic Cancer R. Kevin Reynolds, MD The George W. Morley Professor & Chief, Division of Gyn Oncology University of Michigan Ann Arbor, MI What is gynecologic cancer? Cancer is a disease where cells grow and spread without control. Gynecologic cancers begin in the female reproductive organs. The most common gynecologic cancers are endometrial cancer, ovarian cancer and cervical cancer. Less common gynecologic cancers involve vulva, Fallopian tube, uterine wall (sarcoma), vagina, and placenta (pregnancy tissue: molar pregnancy). Ovary Uterus Endometrium Cervix Vagina Vulva What causes endometrial cancer? Endometrial cancer is the most common gynecologic cancer: one out of every 40 women will develop endometrial cancer. It is caused by too much estrogen, a hormone normally present in women. The most common cause of the excess estrogen is being overweight: fat cells actually produce estrogen. Another cause of excess estrogen is medication such as tamoxifen (often prescribed for breast cancer treatment) or some forms of prescribed estrogen hormone therapy (unopposed estrogen). How is endometrial cancer detected? Almost all endometrial cancer is detected when a woman notices vaginal bleeding after her menopause or irregular bleeding before her menopause. If bleeding occurs, a woman should contact her doctor so that appropriate testing can be performed. This usually includes an endometrial biopsy, a brief, slightly crampy test, performed in the office. Fortunately, most endometrial cancers are detected before spread to other parts of the body occurs Is endometrial cancer treatable? Yes! Most women with endometrial cancer will undergo surgery including hysterectomy (removal of the uterus) in addition to removal of ovaries and lymph nodes. -

Updates in Uterine and Vulvar Cancer
Management of GYN Malignancies Junzo Chino MD Duke Cancer Center ASTRO Refresher 2015 Disclosures • None Learning Objectives • Review the diagnosis, workup, and management of: – Cervical Cancers – Uterine Cancers – Vulvar Cancers Cervical Cancer Cervical Cancer • 3rd most common malignancy in the World • 2nd most common malignancy in women • The Leading cause of cancer deaths in women for the developing world • In the US however… – 12th most common malignancy in women – Underserved populations disproportionately affected > 6 million lives saved by the Pap Test “Diagnosis of Uterine Cancer by the Vaginal Smear” Published Pap Test • Start screening within 3 years of onset of sexual activity, or at age 21 • Annual testing till age 30 • If no history of abnormal paps, risk factors, reduce screening to Q2-3 years. • Stop at 65-70 years • 5-7% of all pap tests are abnormal – Majority are ASCUS Pap-test Interpretation • ASCUS or LSIL –> reflex HPV -> If HPV + then Colposcopy, If – Repeat in 1 year • HSIL -> Colposcopy • Cannot diagnose cancer on Pap test alone CIN • CIN 1 – low grade dysplasia confined to the basal 1/3 of epithelium – HPV negative: repeat cytology at 12 months – HPV positive: Colposcopy • CIN 2-3 – 2/3 or greater of the epithelial thickness – Cold Knife Cone or LEEP • CIS – full thickness involvement. – Cold Knife Cone or LEEP Epidemiology • 12,900 women expected to be diagnosed in 2015 – 4,100 deaths due to disease • Median Age at diagnosis 48 years Cancer Statistics, ACS 2015 Risk Factors: Cervical Cancer • Early onset sexual activity • Multiple sexual partners • Hx of STDs • Multiple pregnancy • Immune suppression (s/p transplant, HIV) • Tobacco HPV • The human papilloma virus is a double stranded DNA virus • The most common oncogenic strains are 16, 18, 31, 33 and 45. -
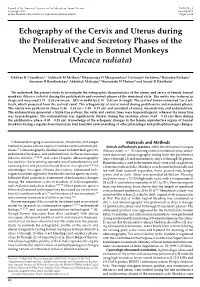
Echography of the Cervix and Uterus During the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca Radiata)
Journal of the American Association for Laboratory Animal Science Vol 53, No 1 Copyright 2014 January 2014 by the American Association for Laboratory Animal Science Pages 18–23 Echography of the Cervix and Uterus during the Proliferative and Secretory Phases of the Menstrual Cycle in Bonnet Monkeys (Macaca radiata) Uddhav K Chaudhari,1,* Siddnath M Metkari,2 Dhyananjay D Manjaramkar,2 Geetanjali Sachdeva,1 Rajendra Katkam,1 Atmaram H Bandivdekar,3 Abhishek Mahajan,4 Meenakshi H Thakur,4 and Sanjiv D Kholkute1 We undertook the present study to investigate the echographic characteristics of the uterus and cervix of female bonnet monkeys (Macaca radiata) during the proliferative and secretory phases of the menstrual cycle. The cervix was tortuous in shape and measured 2.74 ± 0.30 cm (mean ± SD) in width by 3.10 ± 0.32 cm in length. The cervical lumen contained 2 or 3 col- liculi, which projected from the cervical canal. The echogenicity of cervix varied during proliferative and secretory phases. The uterus was pyriform in shape (2.46 ± 0.28 cm × 1.45 ± 0.19 cm) and consisted of serosa, myometrium, and endometrium. The endometrium generated a triple-line pattern; the outer and central lines were hyperechogenic, whereas the inner line was hypoechogenic. The endometrium was significantly thicker during the secretory phase (0.69 ± 0.12 cm) than during the proliferative phase (0.43 ± 0.15 cm). Knowledge of the echogenic changes in the female reproductive organs of bonnet monkeys during a regular menstrual cycle may facilitate understanding of other physiologic and pathophysiologic changes. Ultrasound imaging is a noninvasive, atraumatic, and simple Materials and Methods method to assess various organs in humans and nonhuman pri- Animals and husbandry practices. -

2021 – the Following CPT Codes Are Approved for Billing Through Women’S Way
WHAT’S COVERED – 2021 Women’s Way CPT Code Medicare Part B Rate List Effective January 1, 2021 For questions, call the Women’s Way State Office 800-280-5512 or 701-328-2389 • CPT codes that are specifically not covered are 77061, 77062 and 87623 • Reimbursement for treatment services is not allowed. (See note on page 8). • CPT code 99201 has been removed from What’s Covered List • New CPT codes are in bold font. 2021 – The following CPT codes are approved for billing through Women’s Way. Description of Services CPT $ Rate Office Visits New patient; medically appropriate history/exam; straightforward decision making; 15-29 minutes 99202 72.19 New patient; medically appropriate history/exam; low level decision making; 30-44 minutes 99203 110.77 New patient; medically appropriate history/exam; moderate level decision making; 45-59 minutes 99204 165.36 New patient; medically appropriate history/exam; high level decision making; 60-74 minutes. 99205 218.21 Established patient; evaluation and management, may not require presence of physician; 99211 22.83 presenting problems are minimal Established patient; medically appropriate history/exam, straightforward decision making; 10-19 99212 55.88 minutes Established patient; medically appropriate history/exam, low level decision making; 20-29 minutes 99213 90.48 Established patient; medically appropriate history/exam, moderate level decision making; 30-39 99214 128.42 minutes Established patient; comprehensive history exam, high complex decision making; 40-54 minutes 99215 128.42 Initial comprehensive -

Endometrial Biopsy | Memorial Sloan Kettering Cancer Center
PATIENT & CAREGIVER EDUCATION Endometrial Biopsy This information describes what to expect during and after your endometrial biopsy. About Your Endometrial Biopsy During your endometrial biopsy, your doctor will remove a small piece of tissue from the lining of your uterus. The lining of your uterus is called your endometrium. This tissue is sent to the pathology department to be examined under a microscope. The pathologist will look for abnormal cells or signs of cancer. Before Your Procedure Tell your doctor or nurse if: You’re allergic to iodine. You’re allergic to latex. There’s a chance that you’re pregnant. If you still get your period and are between ages 11 and 50, you will need to take a urine pregnancy test to make sure you’re not pregnant. You won’t need to do anything to get ready for this procedure. During Your Procedure You will have your endometrial biopsy done in an exam room. You will lie on your back as you would for a routine pelvic exam. You will be awake during the procedure. Endometrial Biopsy 1/3 First, your doctor will put a speculum into your vagina. A speculum is a tool that will gently spread apart your vaginal walls, so your doctor can see your cervix (the bottom part of your uterus). Next, your doctor will clean your cervix with a cool, brown solution of povidone- iodine (Betadine® ). Then, they will put a thin, flexible tool, called a pipelle, through your cervix and into your uterus to take a small amount of tissue from your endometrium. -

The Discovery of Different Types of Cervical Mucus and the Billings Ovulation Method
The Discovery of Different Types of Cervical Mucus and the Billings Ovulation Method Erik Odeblad Emeritus Professor, Dept. of Medical Biophysics, University of Umeå, Sweden Published with permission from the Bulletin of the Ovulation Method Research and Reference Centre of Australia, 27 Alexandra Parade, North Fitzroy, Victoria 3068, Australia, Volume 21, Number 3, pages 3-35, September 1994. Copyright © Ovulation Method Research and Reference Centre of Australia 1. Abstract 2. Introduction 3. Anatomy and Physiology 4. What is Mucus? 5. The Commencement of my Research 6. The Existence of Different Types of Crypts and of Mucus 7. Identification and Description of G, L, and S Mucus 8. G- and G+ Mucus 9. Age, Pregnancy, the Pill and Microsurgery 10. P Mucus 11. F Mucus 12. The Role of the Vagina 13. The Different Types of Secretions and the Billings Ovulation Method 14. Early Infertile Days 15. The Days of Possible Fertility 16. Late Infertile Days 17. Anovulatory Cycles 18. Lactation 19. Diseases and the Billings Ovulation Method 20. The Future 21. Acknowledgements 22. Author's Note 23. References 24. Appendix Abstract An introduction to and some new anatomical and physiological aspects of the cervix and vagina are presented and also an explanation of the biosynthesis and molecular structure of mucus. The history of my discoveries of the different types of cervical mucus is given. In considering my microbiological investigations I suspected the existence of different types of crypts and cervical mucus and in 1959 1 proved the existence of these different types. The method of examining viscosity by nuclear magnetic resonance was applied to microsamples of mucus extracted 1 outside of several crypts. -

Primary Immature Teratoma of the Thigh Fig
CORRESPONDENCE 755 8. Gray W, Kocjan G. Diagnostic Cytopathology. 2nd ed. London: Delete all that do not apply: Elsevier Health Sciences, 2003; 677. 9. Richards A, Dalrymple C. Abnormal cervicovaginal cytology, unsatis- Cervix, colposcopic biopsy/LLETZ/cone biopsy: factory colposcopy and the use of vaginal estrogen cream: an obser- vational study of clinical outcomes for women in low estrogen states. Diagnosis: NIL (No intraepithelial lesion WHO 2014) J Obstet Gynaecol Res 2015; 41: 440e4. LSIL (CIN 1 with HPV effect WHO 2014) 10. Darragh TM, Colgan TJ, Cox T, et al. The lower anogenital squamous HSIL (CIN2/3 WHO 2014) terminology standardization project for HPV-associated lesions: back- Squamous cell carcinoma ground and consensus recommendation from the College of American Immature squamous metaplasia Pathologists and the American Society for Colposcopy and Cervical Adenocarcinoma in situ (AIS, HGGA) e Adenocarcinoma Pathology. Arch Pathol Lab Med 2012; 136: 1267 97. Atrophic change 11. McCluggage WG. Endocervical glandular lesions: controversial aspects e Extending into crypts: Not / Idenfied and ancillary techniques. J Clin Pathol 2013; 56: 164 73. Epithelial stripping: Not / Present 12. World Health Organization (WHO). Comprehensive Cervical Cancer Invasive disease: Not / Idenfied / Micro-invasive Control: A Guide to Essential Practice. 2nd ed. Geneva: WHO, 2014. Depth of invasion: mm Transformaon zone: Not / Represented Margins: DOI: https://doi.org/10.1016/j.pathol.2019.07.014 Ectocervical: Not / Clear Endocervical: Not / Clear Circumferenal: Not / Clear p16 status: Negave / Posive Primary immature teratoma of the thigh Fig. 3 A proposed synoptic reporting format for pathologists reporting colposcopic biopsies and cone biopsies or LLETZ. Sir, Teratomas are germ cell tumours composed of a variety of HSIL, AIS, micro-invasive or more advanced invasive dis- somatic tissues derived from more than one germ layer 12 ease. -

Squamous Cell Carcinoma Arising in an Ovarian Mature Cystic Teratoma
Case Report Obstet Gynecol Sci 2013;56(2):121-125 http://dx.doi.org/10.5468/OGS.2013.56.2.121 pISSN 2287-8572 · eISSN 2287-8580 Squamous cell carcinoma arising in an ovarian mature cystic teratoma complicating pregnancy Nae-Ri Yun1, Jung-Woo Park1, Min-Kyung Hyun1, Jee-Hyun Park1, Suk-Jin Choi2, Eunseop Song1 Departments of 1Obstetrics and Gynecology and 2Pathology, Inha University College of Medicine, Incheon, Korea Mature cystic teratomas of the ovary (MCT) are usually observed in women of reproductive age with the most dreadful complication being malignant transformation which occurs in approximately 1% to 3% of MCTs. In this case report, we present a patient with squamous cell carcinoma which developed from a MCT during pregnancy. The patient was treated conservatively without adjuvant chemotherapy and was followed without evidence of disease for more than 60 months using conventional tools as well as positron emission tomography-computed tomography following the initial surgery. We report this case along with the review of literature. Keywords: Dermoid cyst; Malignant transformation; Observation; Positron emission tomography-computed tomography Introduction An 18 cm solid and cystic left ovarian mass with a smooth surface and two small right ovarian cysts were detected re- The incidence of adnexal masses during pregnancy is 1% to sulting in a laparotomy at 13 weeks of gestation and left sal- 9% [1]. Mature cystic teratomas (MCT) are common during pingo-oophorectomy and right ovarian cystectomy (Fig. 1C). pregnancy with the most dreadful complication being ma- The report of the frozen section from both tissues revealed lignant transformation which occurs in approximately 1% to MCT. -
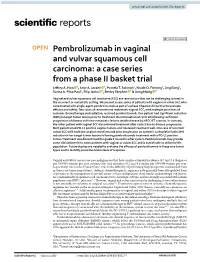
Pembrolizumab in Vaginal and Vulvar Squamous Cell Carcinoma: a Case Series from a Phase II Basket Trial Jefrey A
www.nature.com/scientificreports OPEN Pembrolizumab in vaginal and vulvar squamous cell carcinoma: a case series from a phase II basket trial Jefrey A. How 1, Amir A. Jazaeri 1, Pamela T. Soliman1, Nicole D. Fleming1, Jing Gong2, Sarina A. Piha‑Paul2, Filip Janku 2, Bettzy Stephen 2 & Aung Naing 2* Vaginal and vulvar squamous cell carcinoma (SCC) are rare tumors that can be challenging to treat in the recurrent or metastatic setting. We present a case series of patients with vaginal or vulvar SCC who were treated with single‑agent pembrolizumab as part of a phase II basket clinical trial to evaluate efcacy and safety. Two cases of recurrent and metastatic vaginal SCC, with multiple prior lines of systemic chemotherapy and radiation, received pembrolizumab. One patient had signifcant reduction (81%) in target tumor lesions prior to treatment discontinuation at cycle 10 following confrmed progression of disease with new metastatic lesions (stable disease by irRECIST criteria). In contrast, the other patient with vaginal SCC discontinued treatment after cycle 3 due to disease progression. Both patients had PD‑L1 positive vaginal tumors and tolerated treatment well. One case of recurrent vulvar SCC with multiple surgical resections and prior progression on systemic carboplatin had a 30% reduction in her target tumor lesions following pembrolizumab treatment with a PD‑L1 positive tumor. Treatment was discontinued for grade 3 mucositis after cycle 5. Pembrolizumab may provide some clinical beneft to some patients with vaginal or vulvar SCC and is overall safe to utilize in this population. Future studies are needed to evaluate the efcacy of pembrolizumab in these rare tumor types and to identify predictive biomarkers of response. -

Sexual Dysfunction in Gynecologic Cancer Patients
WCRJ 2017; 4 (1): e835 SEXUAL DYSFUNCTION IN GYNECOLOGIC CANCER PATIENTS L. DEL PUP Division of Gynecological Oncology, CRO Aviano, National Cancer Institute, Aviano (PN), Italy. Abstract – Objective: Sexual dysfunction is prevalent among gynecologic cancer survivors and strongly impacts on the quality of life (QoL), but the subject is poorly diagnosed and treated. Materials and Methods: A comprehensive literature search of English language studies on sex- ual dysfunctions due to gynecologic cancer treatment has been conducted on MEDLINE databases. Results: Surgery, radiation, and chemotherapy can cause any kind of sexual dysfunction with different mechanisms: psychological and relational, hormonal and pharmacological, neurological and vascular, side effects of chemo and radiation therapies, and direct effects of surgery on sexually involved pelvic organs. Many patients expect their healthcare providers to address sexual health concerns, but most have never discussed sex-related issues with their physician, or they do not re- ceive a proper treatment or referral. This can have medical legal consequences, because it must be discussed and documented before starting treatment. Conclusions: Oncology providers can make a significant impact on the QoL of gynecologic cancer sur- vivors by informing patients and by asking them for sexual health concerns. Counseling is per se beneficial, as it improves QoL. Furthermore, it permits a proper referral and resolution of most symptoms. KEYWORDS: Gynecologic cancer, Sexual dysfunction, Vulvar cancer, Vaginal cancer, Cervical cancer, Endometrial cancer, Ovarian cancer, Ospemifene. INTRODUCTION ly ask about sexual issues, but 64% state that phy- sicians never initiates the conversation during their The proportion of people living with and surviv- care3. ing gynecologic cancer is growing. -

Vaginal Discharge, Itching Vaginal Bleeding, Amenorrhea
Common Problem of the Gynecological System Vaginal Discharge, itching vaginal bleeding, amenorrhea 本講義表格資料取自Dains, J.E., Baumann, L.C., & Scheibel, P. (2007). Advanced assessment and clinical diagnosis in primary care. (3rd ed). St. Louis: Mosby. 1 圖片取自Seidel HM, Ball JW, Dains JE, Benedict GW. (1999). Mosby’s guide to physical examination. St. Louis, MO: Mosby. VildihVaginal discharge and itching 2 Vaginitis • Inflammation of vaggggina, cause vaginal discharge • In child bearing women, 95% due to • Trichomonas vaginalis (陰道滴蟲), • Candida, • bacteria vaginosis (BV): • epithelium is not inflamed • Risk for premature rupture of mambrane and early delivery • Postmenopausal women: atrophic vaginitis • In young girl: vulvovaginitis • due to hypoestrogenic state and poor perineal hygiene 3 Characteristic of discharge • Copious, greenish, offensive-smelling: • Trichomonas vaginalis • Mucopurulent or purulent • Gonorrhea and Chlamyy(dia (披衣菌) • Moderate amount, white, curd-like discharge • Candida vulvovaginitis • CittithithiConsistent with itching • Birth control pills, steroid, antibiotic, chemotherapy • Thin white,,g green, ,g grey or brownish •BV • Also with fishly odor • Need microscopic exam to confirm the diagnosis 4 Lesion • Vesicle • Herpes • Papular on labia, perineum, and anal area • CdlCondyloma tlt(ta lata(扁平濕疣)dllt), condyllomata acuminata(尖型濕疣), • Malluscum contagiosum (傳染性軟疣) • Painless ulcer • Syphilis 5 Pelvic infection disease • Cervical motion tender (CMT) • Pain on palpation of uterus and adnexa • Purulent discharge • Need