Aviation Safety Investigation Report 200304282
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
LIGHTING WORKSHOP 2018 2018 Brisbane Airportconference Centre Tuesday 22May Brisbane Airportconference Centre Tuesday 22May
LIGHTING WORKSHOP Tuesday 22 May 2018 Brisbane Airport Conference Centre PAVEMENT TECHNOLOGY WORKSHOP Tuesday 22 May 2018 Brisbane Airport Conference Centre PROGRAM www.airports.asn.au THE AUSTRALIAN AIRPORTS ASSOCIATION The AAA facilitates co-operation among all member airports and their many and varied partners in Australian aviation, whilst The Australian Airports Association (AAA) The AAA represents the interests of over contributing to an air transport system that is a non-profit organisation that was 380 members. This includes more than is safe, secure, environmentally responsible 260 airports and aerodromes Australia and efficient for the benefit of all Australians founded in 1982 in recognition of the real wide – from the local country community and visitors. need for one coherent, cohesive, consistent landing strip to major international and vital voice for aerodromes and airports gateway airports. The AAA is the leading advocate for throughout Australia. appropriate national policy relating to The AAA also represents more than airport activities and operates to ensure 120 aviation stakeholders and regular transport passengers, freight, and organisations that provide goods and the community enjoy the full benefits of a services to airports. progressive and sustainable airport industry. CONTACT US P: 02 6230 1110 E: [email protected] w: www.airports.asn.au Welcome to the AAA Pavement Technology Workshop and Lighting Workshop. These are two new events for 2018, and form part of the commitment the AAA has to provide the aviation industry with comprehensive technical training and research updates. We know how important it is to meet your peers and share ideas at these occasions, so we hope you enjoy the opportunity to attend our Networking Drinks, overlooking Brisbane Airport runway, at the Sky Lounge, IBIS. -

Media Release
MEDIA RELEASE 24 December 2008 QUEENSLAND AIRPORTS LIMITED WELCOMES ANNOUNCEMENT ON CAIRNS AIRPORT Queensland Airports Limited (QAL) today welcomes the news of the sale of Cairns Airport to a purchasing consortium including JP Morgan, The Infrastructure Fund (TIF) and the Westpac Banking Corporation. QAL has been appointed to provide expert technical services to the consortium. QAL Managing Director Dennis Chant said Cairns Airport was a significant opportunity for the growth of the Group. “QAL has unique experience in managing regional airports in Queensland and we welcome the announcement today that our shareholders in partnership with JP Morgan have secured this vital piece of infrastructure. “Cairns is a world renowned tourism destination and we are very keen to connect with local industry stakeholders to maintain Cairns International Airport’s pivotal role in facilitating visitation to Tropical North Queensland. “As the owner operator of Gold Coast Airport, QAL management is well versed in the need to develop cooperative marketing alliances with state and local tourism industry stakeholders to attract visitors in a fiercely competitive leisure market,” he said. “Working together, Cairns, Gold Coast and Queensland Tourism will present a formidable competitor to the newly emerging Asian destinations that have been successfully making inroads into our traditional source markets. “QAL also owns and operates Townsville and Mount Isa Airports, and provides technical services expertise to Mackay Airport, all of which have a strong business and resource sector. We look forward to working with the local Cairns business sector to ensure the Far North Queensland region continues to grow. …/2 “QAL is already a significant employer in regional Queensland. -

Mackay Airport Aerodrome Manual
MACKAY AIRPORT AERODROME MANUAL Reference No: 9000MKY Version 11 26 Feb 2021 ACN 132 228 534 AERODROME MANUAL PART 0 SECTION 01 FOREWORD Mackay Airport Pty Ltd owns and manages Mackay Airport which includes all airside and landside operations, terminals, car parking and associated land holdings and is part of the North Queensland Airports (NQA) group. NQA is owned by a consortium comprising of IIF Cairns Mackay Investment Ltd (an entity advised by JP Morgan Asset Management), The Infrastructure Fund (TIF) and Perron Investments. For quality control purposes, this document is only valid on the day it is printed. Official versions are stored on the intranet. This copy was last saved: 01/03/2021 , last printed: 02/03/2021 9000_MKY_Aerodrome Manual_Effective Date: 26/02/2021 Review Date: 25/02/2022 Page 2 of 102 AERODROME MANUAL The Aerodrome Manual contains details of the airside operating procedures that we importantly need to adopt to ensure the safety and viability of our airport. The Aerodrome Manual also satisfies our legal obligations under the Civil Aviation Safety Regulations (CASR) Part 139, in particular CASR 139.090. Any items under CASR 139.0959(a) that are not applicable to Mackay Airport, are not included within this manual. Mackay Airport is transitioning to its Aerodrome Manual line with Part 139 (Aerodromes) Manual of Standards 2019. Mackay Airport has received written approval from CASA for the Aerodrome Manual to consist of more than one document. All separate documents referenced throughout this manual are readily available from Mackay Airport and each staff member is responsible for ensuring that they can access these documents. -
Airport Categorisation List
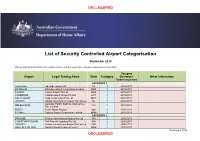
UNCLASSIFIED List of Security Controlled Airport Categorisation September 2018 *Please note that this table will continue to be updated upon new category approvals and gazettal Category Airport Legal Trading Name State Category Operations Other Information Commencement CATEGORY 1 ADELAIDE Adelaide Airport Ltd SA 1 22/12/2011 BRISBANE Brisbane Airport Corporation Limited QLD 1 22/12/2011 CAIRNS Cairns Airport Pty Ltd QLD 1 22/12/2011 CANBERRA Capital Airport Group Pty Ltd ACT 1 22/12/2011 GOLD COAST Gold Coast Airport Pty Ltd QLD 1 22/12/2011 DARWIN Darwin International Airport Pty Limited NT 1 22/12/2011 Australia Pacific Airports (Melbourne) MELBOURNE VIC 1 22/12/2011 Pty. Limited PERTH Perth Airport Pty Ltd WA 1 22/12/2011 SYDNEY Sydney Airport Corporation Limited NSW 1 22/12/2011 CATEGORY 2 BROOME Broome International Airport Pty Ltd WA 2 22/12/2011 CHRISTMAS ISLAND Toll Remote Logistics Pty Ltd WA 2 22/12/2011 HOBART Hobart International Airport Pty Limited TAS 2 29/02/2012 NORFOLK ISLAND Norfolk Island Regional Council NSW 2 22/12/2011 September 2018 UNCLASSIFIED UNCLASSIFIED PORT HEDLAND PHIA Operating Company Pty Ltd WA 2 22/12/2011 SUNSHINE COAST Sunshine Coast Airport Pty Ltd QLD 2 29/06/2012 TOWNSVILLE AIRPORT Townsville Airport Pty Ltd QLD 2 19/12/2014 CATEGORY 3 ALBURY Albury City Council NSW 3 22/12/2011 ALICE SPRINGS Alice Springs Airport Pty Limited NT 3 11/01/2012 AVALON Avalon Airport Australia Pty Ltd VIC 3 22/12/2011 Voyages Indigenous Tourism Australia NT 3 22/12/2011 AYERS ROCK Pty Ltd BALLINA Ballina Shire Council NSW 3 22/12/2011 BRISBANE WEST Brisbane West Wellcamp Airport Pty QLD 3 17/11/2014 WELLCAMP Ltd BUNDABERG Bundaberg Regional Council QLD 3 18/01/2012 CLONCURRY Cloncurry Shire Council QLD 3 29/02/2012 COCOS ISLAND Toll Remote Logistics Pty Ltd WA 3 22/12/2011 COFFS HARBOUR Coffs Harbour City Council NSW 3 22/12/2011 DEVONPORT Tasmanian Ports Corporation Pty. -
MINUTES AAA QLD Division
MINUTES AAA QLD Division Wednesday 21 March 2018 Brisbane Airport Conference Centre, Brisbane Chair: Rob Porter – General Manager Mackay Airport Attendees: List of Attendees Attached Apologies: Rob MacTaggart (The Airport Group) 1. CONFIRMATION OF MINUTES FROM PREVIOUS MEETING: Noted minutes from last meeting. 2. WELCOME AND INTRODUCTIONS: Rob Porter (General Manager Mackay Airport) opened the meeting, welcomed members and thanked Smiths Detection for sponsoring the meeting. Also thanked our division dinner sponsors Trident Services and Airport Equipment. Noted the excellent presentation from Neil Scales at the dinner, noting that we will invite him back in 12 months’ time to share his experiences. Rob Porter (General Manager Mackay Airport) encouraged members to provide feedback to the AAA team on the recent communications innovations (airport professional, the centre line, social media, etc.) The hot topics section at the end of the agenda was noted and the Chair, encouraged members to share their thoughts. Rob Porter (General Manager Mackay Airport) encouraged members to provide feedback on the number and structure of division meetings. Noted ‘out of the box’ topic suggestions are always welcome. Rob Porter (General Manager Mackay Airport) provided members with an overview of the agenda. Noting the ‘around the tarmacs’ section and encouraged members share their activity. QLD Overview Rob Porter (General Manager Mackay Airport) noted increase pressure across the state in access to aircraft, this has put upwards pressure on regional airfares in particular. 1 3. AAA UPDATE Simon Bourke (Policy Director AAA) noted key topics that the AAA had been working on over the past 6 months. Security Changes Proposed changes to Aviation Security will have an impact on all aviation sectors. -

North Queensland Airports (NQA)
Invest & Manage Airports 2011 London December 9th, 2011 North Queensland Airports (NQA) In January 2009, a consortium led by institutional investors advised by J.P.Morgan Asset Management bought Cairns & Mackay airports from the Queensland government NQA owns and manages Cairns and Mackay airports under 99-year leases – Cairns is Australia's 7th largest airports with c. 4.0m pax in FY11 and the gateway to World Heritage Great Barrier Reef and Tropical Rainforests of Northern Queensland – Mackay airport, with c. 1m pax in FY11, is the main airport serving the Bowen Basin, which contains one of the largest deposits of coal in the world 2 NQA - Overview Cairns Airport Cairns Airport 758 ha site located c.8 km from the CBD Separate domestic & international terminals Two runways: main runway (3,197m) & cross runway (925m) Curfew free Mackay Airport Mackay Airport 274 ha site located c.5 km from the CBD Single terminal Two runways: main runway (1,981m), cross runway (1,344m) Curfew free 3 NQA – Passenger Profile Cairns Mackay 6% 6% 12% 25% 44% 11% 64% NQA 25% 6% 16% 17% 61% Leisure Business VFR Other 4 NQA – Strong Traffic performance since Acquisition FY 2011/2010 Passenger growth 9.9% 9.5% 7.7% 6.9% 4.3% 4.1% 3.6% NQA Perth Airport APAC MAp QAL Sydney Airport NT Airports 5 Continued route expansion and carrier diversification 81 new services and new routes introduced since acquisition equating to over 1.4m new seats Both Cairns and Mackay have experienced strong volumes growth as a result of: – Strategically marketing the airport -

Mackay Airport Land Use Plan – August 2014
Central Queensland’s Multimodal Integrated Transport Hub LAND USE PLAN August 2014 Citation and commencement This Land use plan may be cited as the Mackay Airport Land use plan. Corporate vision and mission Mackay Airport Pty Ltd’s vision is to be a valued partner in Central Queensland’s progress and development. Our mission is to be respected members of our host community who deliver a positive memorable gateway experience to passengers and contribute to the economic growth of our stakeholders, the region and the State. Our values are to: MACKAY AIRPORT Central Queensland’s Multimodal Integrated Transport Hub • prioritise safety and security; • engage with users and stakeholders; • operate as a commercial business; ii • promote co-operation and accountability; • leverage our combined expertise; and • embrace our responsibilities. Editor’s note - the Corporate vision and mission statement is extrinsic material to the Land use plan. LAND USE PLAN August 2014 PREPARED BY: This Land use plan has been prepared by Brett Rose, North Queensland Airports General Manager Property Development, PO Box 57, Airport Administration Centre, Cairns Airport, Cairns Qld 4870 on behalf of and for the exclusive use of Mackay Airport Pty Ltd (MAPL). COPYRIGHT: © Mackay Airport Pty Ltd (MAPL) - August 2014. Copyright protects this document. Except for purposes permitted by the Copyright Act 1968 (Cth), no part may be reproduced by any means whatsoever, electronic or otherwise, without the prior written permission of MAPL. Request for permission should be directed to the Chief Executive Officer at North Queensland Airports Pty Ltd, PO Box 57, Airport Administration Centre, Cairns Airport, Cairns Qld 4870. -
Appendix D - Regional Airport Survey
D Appendix D - Regional Airport Survey Survey aims 1.1 As described in the submissions and evidence, many councils expressed varying degrees of difficulty in managing their airports. The committee therefore decided to conduct a survey of councils that own and operate regional airports, in order to gain an understanding of: The variation in fees charged by airports; How much it costs to operate and maintain an airport; How much income is generated from airport operations; and Which councils were struggling to operate and maintain their airports. Who was surveyed 1.2 The committee chose to survey all of the councils that had made submissions to the inquiry, and added another 30 or so councils whose passenger statistics up until 2001 appeared in Bureau of Transport and Regional Economics’ Avstats data. The number of surveys was considered representative of councils that own airports, and was also manageable given the time available. Councils surveyed included those with large populations and viable air services, through to smaller councils that have no current air services. 240 REGIONAL AVIATION AND ISLAND TRANSPORT SERVICES: MAKING ENDS MEET Survey design 1.3 A simple survey was designed and mailed to 89 councils. The survey featured 16 simple questions. A copy of the survey can be found in Appendix E. The survey was approved through the Statistical Clearing House at the Australian Bureau of Statistics. Results 1.4 The committee received 69 responses from the total of 89 surveys sent out to councils. A total of 63 surveys provided data for analysis. The committee was disappointed that 20 councils could not find the time to respond to the survey. -

Avis Australia Tour Programme Participating Locations
AVIS AUSTRALIA TOUR PROGRAMME IMPORTANT NOTICE Tour Rates are available PARTICIPATING LOCATIONS at these locations only. QUEENSLAND NEW SOUTH WALES METROPOLITAN AREAS TOWNSVILLE METROPOLITAN AREAS WOLLONGONG BRISBANE Townsville Airport (TSV) (07) 4762 7400 GOSfORD Main Office (WLL) (02) 4251 1311 Terminal Building 47 Flinders St 2500 fortitude Valley (BN1) (07) 3406 5188 Main Office (GOS) (02) 4323 2222 728 Ann St (cnr Warner St), Fortitude Valley 4006 Townsville (TV4) (07) 4799 2022 322 Mann St, Gosford 2250 COUNTRY AREAS 81-83 Flinders St East 4810 Brisbane City (BN0) (07) 3247 0577 NEWCASTLE Albury/Wodonga (ABx) (02) 6021 5399 53 Albert St, cnr Albert & Margaret St 4000 PORT DOUGLAS Airport Drive, Albury Airport 2640 Mayfield (NWS) (02) 4904 4411 Brisbane Airport (BNE) (07) 3633 8666 Port Douglas (PD7) (07) 4099 4331 50 Clyde St, Hamilton North 2292 Albury Downtown (L4y) (02) 6021 5399 All terminals 4007 7 Warner St 4871 24 Airport Drive, Albury 2640 Newcastle Airport (NTL) (02) 4965 1451 BRISBANE NORTH SUNSHINE COAST Airport Terminal, Williamtown 2318 Ballina (BNK) (02) 6686 7650 Terminal Building, Southern Cross Dr, Ballina 2478 All reservations via Boondall Maroochydore (MD4) (07) 5453 1999 SYDNEY Coffs Harbour Airport (CfS) (02) 6651 3600 Boondall (Bx8) (07) 3131 3922 74A Aerodrome Rd 4558 Artarmon (U10) (02) 9438 9955 Airport Terminal 2450 131 Zillmere Rd, Boondall 4034, Boondall 4034 Noosa (NSA) (07) 5473 8955 75-77 Carlotta St 2064 Coffs Harbour (C6H) (02) 6651 3600 Strathpine (SP7) (07) 3131 3922 Shop 1 Ocean Breeze Resort, -

Europcar Participating Locations AU4.Xlsx
Canberra Airport All Terminals, Terminal Building Canberra Airport Canberra ACT Canberra City Novotel City, 65 Northbourne Avenue Canberra ACT Alexandria 1053 Bourke Street Waterloo NSW Artarmon 1C Clarendon Street Artarmon NSW Blacktown 231 Prospect Highway Seven Hills NSW Coffs Harbour Airport Terminal Building Airport Drive Coffs Harbour NSW Coffs Harbour City 194 Pacific Highway Corner Bailey Avenue Coffs Harbour NSW Darling Harbour 320 Harris Street Pyrmont NSW Milperra 299-301 Milperra Road Milperra NSW Newcastle Airport Terminal Building, Williamtown Drive Williamtown NSW Newcastle City 20 Denison Street West NSW Parramatta 78-84 Parramatta Road Granville NSW Penrith 6-8 Doonmore Street Penrith NSW Sydney Airport All Terminals, Terminal Building, Sydney Airport Mascot NSW Sydney Central Inside Mercure Hotel, 818-820 George Street Sydney NSW Sydney City Pullman Hotel, 36 College Street Sydney NSW Wollongong 8A Flinders Street Wollongong NSW A&G Laverton 105 William Angliss Drive Laverton North VIC Albion 2/ 590 Ballarat Road Albion VIC Avalon 81 Beach Road Avalon VIC Bayswater 244 Canterbury Road Bayswater VIC Blackburn 110 Whitehorse Road Blackburn VIC Clayton 2093-2097 Princess Highway Clayton VIC Epping 18 Yale Drive Epping VIC Knox Woods Accident Repair Centre, 34 Gilbert Park Drive Knoxfield VIC Melbourne Airport All Terminals, Terminal Building, Melbourne Airport Tullamarine VIC Melbourne City 89-91 Franklin Street Melbourne VIC Moorabbin 245-247 Wickham Road Moorabbin VIC Preston 580 High Street Preston VIC Richmond 26 Swan -
Un-Fare, Un-Australian - Why Is It So? Submission from the Mount Isa City Council
Un-Fare, Un-Australian - Why is it so? Submission from the Mount Isa City Council Australian Senate Inquiry into Regional Air Services 1 February 2018 1 Contact Sharon Ibardolaza Acting Chief Executive Officer Mount Isa City Council Phone 07 4747 3200 | Fax 07 4747 3209 Email [email protected] PO BOX 815 | Mount Isa Qld 4825 2 / 32 Table of Contents EXECUTIVE SUMMARY ............................................................................................................................ 4 RECOMMENDED ACTIONS ...................................................................................................................... 5 INTRODUCTION ........................................................................................................................................ 6 ABOUT MOUNT ISA ................................................................................................................................... 6 IMPACTS OF HIGH AIRFARES ................................................................................................................. 8 Poor service standards ............................................................................................................................... 9 Airfares ........................................................................................................................................................ 9 NATIONAL TRENDS IN AUSTRALIAN AVIATION .................................................................................. 10 Trends at Mount Isa ..................................................................................................................................12 -
Submission 49
North Queensland Airports Submission Productivity Commission Inquiry Into Economic Regulation of Airports 7 September 2018 1. EXECUTIVE SUMMARY 3 ABOUT NORTH QUEENSLAND AIRPORTS 3 NQA’S PRIMARY POSITION 3 2. CAIRNS AND MACKAY AIRPORTS 8 CAIRNS AIRPORT 8 MACKAY AIRPORT 11 3. MARKET POWER IN THE PRICING OF AERONAUTICAL SERVICES 14 TESTS OF MARKET POWER 14 PRICING OF INTERNATIONAL SERVICES AT CAIRNS AIRPORT 19 PRICING OF REGIONAL SERVICES AT CAIRNS AIRPORT 20 PRICING OF SERVICES AT MACKAY AIRPORT 20 4. COUNTERVAILING POWER OF USERS 21 SHORT PAYING 21 DOMESTIC AIRLINE INDUSTRY STRUCTURE 23 CAIRNS AND MACKAY MARKET DYNAMICS 24 5. EXERCISE OF MARKET POWER 26 6. LAND TRANSPORT 30 MODE SHARE 30 TAXIS AND RIDE SHARE 30 PUBLIC PICK-UP AND DROP-OFF 31 CAR RENTAL 31 CAR PARKING 32 BUSES 32 PUBLIC TRANSPORT 33 TRIP COST BY MODE 33 7. PROVISION OF SECURITY SERVICES 35 GLOSSARY 36 2 1. Executive Summary North Queensland Airports (NQA) is pleased to have the opportunity to make this submission to the Productivity Commission. This submission focusses on items contained in the Economic Regulation of Airport Services, Productivity Commission Issues Paper of July 2018, specifically: • Market power in the provision of aeronautical services • Countervailing power of users • Exercise of market power, and • Land transport arrangements as relating to airports leased and operated by NQA. About North Queensland Airports NQA operates Cairns and Mackay Airports under long term leases from the State of Queensland. Cairns Airport serves domestic and international airlines and has a large General Aviation (GA) presence. Mackay Airport serves domestic airlines only.