Community Based Seroprevalence of HBV and HCV Infection in Bauchi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

325013-Eng.Pdf (602.0Kb)
,I I BIUGIII SMIT PROGNI$S NHllRI illarch 2000 - fG[,2001 SUBilIIIEII MIRGH 20ll1 r0 fi]RrGlil Pn08n[ililt ron ONGilIIGTNGNSF GOilIROl NPllSI For Actica 0ufiGfft0u80u BURmlilm$0 l1 '{{ .,t t., jl t I : .{ 1i KEV @ cATt L.G,n,e ('6, ruofr/ r elit ns. [] SECTION ONE BACKGROUND Bauchi State project is located in the North-East of Nigerian. There are 20 local Govemment Ares in the State. The State shares boundaries with Plateau, Kano, Jigawa, Yobe, Borno, Taraba and Gombe States. The State lies in the Savannah region of Nigeria, with variation in ecological conditions with the southern and western parts being sudan or guinea Savannah, having a relatively higher rainfall, the northern part of the State is sahel Savannah with flat lands and fewer hills. Some major rivers traverse the State. These include the river Hadeja, Jama'are, Gongola and Dindima. Most of the endemic local government areas lies along these river systems. The State has two distinct seasons', dry and rain seasons. There are six months of rain, beginning in May and ending in October. The farming season is from May to December. Most of the onchocerciasis endemic communities are not accessible all year round; the dirt and laterite roads to these communities are usually not motor-able during the height of the rainy season. Even in dry season, where the roads are sandy, four-wheel drive vehicles may be required in some instances along with motorcycles and bicycles. The settlement pattern varies in different part of the State. Generally, there is a pattern of nuclear settlements, with surrounding farmlands. -

Inventory of Existing Rural Water Supply Sources Using Model Nigerian Communities Vis a Vis Household Access to Improved Water
IOSR Journal of Mechanical and Civil Engineering (IOSR-JMCE) e-ISSN: 2278-1684,p-ISSN: 2320-334X, Volume 11, Issue 4 Ver. VII (Jul- Aug. 2014), PP 16-23 www.iosrjournals.org Inventory Of Existing Rural Water Supply Sources Using Model Nigerian Communities Vis a Vis Household Access to Improved Water NDUBUBA, Olufunmilayo I. Civil Engineering Dept. Abubakar Tafawa Balewa University, Bauchi, Nigeria Abstract: A household is considered to have access to basic services required by a family unit in Nigeria if the household has water supply and sanitation facilities, which are used appropriately at all times. A comprehensive inventory of all water sources was conducted in 12 Local Government Areas (LGAs) of four States of Bauchi, Benue, Jigawa and Katsina States between 2011 and 2012; the data was used to relate access to basic services of the people to the population living within the communities studied. It was found that Katsina State had the largest number of solar powered water supply systems (40.3% of all motorized water sources in the State) followed by Bauchi with 36.4%. The most common improved rural water source in the LGAs was bore-holes with hand-pumps (82.28%). Functionality was also monitored. For hand-pumps, there was a relationship between community ownership and functionality (Dass-Bauchi 77.17%; Warji-Bauchi 75.15%; Oju-Benue 82.09%). Population data on each LGA used to analyse the percentage number of household using the improved water sources showed that all the four LGAs still fall short of the basic access of 30 litres per capita per day within 250 metres radius of the water source. -

Nigeria Hotspots Location by State Platform Cholera Bauchi State West and Central Africa
Cholera - Nigeria hotspots location by state Platform Cholera Bauchi State West and Central Africa Katagum Jigawa Gamawa Zaki Gamawa Yobe Itas Itas/Gadau Hotspots typology in the State Jama'are Jamao�oareAzare Damban Hotspot type T.1: High priority area with a high frequency Katagum Damban and a long duration. Kano Shira Shira Giade Hotspot type T.2: Giade Misau Misau Medium priority area with a moderate frequency and a long duration Warji Darazo Warji Ningi Darazo Ningi Hotspots distribution in the State Ganjuwa Ganjuwa 10 8 Bauchi Hotspots Type 1 Hotspots Type 2 Kirifi Toro Kirfi Gombe Bauchi Ningi Alkaleri Itas/Gadau Alkaleri Dass Shira Damban Katagum Kaduna Bauchi Ganjuwa Toro Darazo Misau Jama'are Warji Gamawa Toro Dass Kirfi Tafawa-Balewa Giade Dass Tafawa-Balewa Alkaleri Legend Tafawa-Balewa Bogoro Countries State Main roads Bogoro Plateau XXX LGA (Local Governmental Area) Hydrography Taraba XXX Cities (State capital, LGA capital, and other towns) 0 70 140 280 420 560 Kilometers Date of production: January 21, 2016 Source: Ministries of Health of the countries members of the Cholera platform Contact : Cholera project - UNICEF West and Central Africa Regionial Office (WCARO) Feedback : Coordination : Julie Gauthier | [email protected] Information management : Alca Kuvituanga | [email protected] : of support the With The epidemiological data is certified and shared by national authorities towards the cholera platform members. Geographical names, designations, borders presented do not imply any official recognition nor approval from none of the cholera platform members . -

Redalyc.Characteristics of Irrigation Tube Wells on Major River Flood
Ambiente & Água - An Interdisciplinary Journal of Applied Science ISSN: 1980-993X [email protected] Universidade de Taubaté Brasil Abubakar Sadiq, Abdullahi; Abubakar Amin, Sunusi; Ahmad, Desa; Gana Umara, Baba Characteristics of irrigation tube wells on major river flood plains in Bauchi State, Nigeria Ambiente & Água - An Interdisciplinary Journal of Applied Science, vol. 9, núm. 4, octubre-diciembre, 2014, pp. 603-609 Universidade de Taubaté Taubaté, Brasil Available in: http://www.redalyc.org/articulo.oa?id=92832359004 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Ambiente & Água - An Interdisciplinary Journal of Applied Science ISSN 1980-993X – doi:10.4136/1980-993X www.ambi-agua.net E-mail: [email protected] Characteristics of irrigation tube wells on major river flood plains in Bauchi State, Nigeria doi: 10.4136/ambi-agua.1314 Received: 12 Feb. 2014; Accepted: 05 Sep. 2014 Abdullahi Abubakar Sadiq1*; Sunusi Abubakar Amin1; Desa Ahmad2; Baba Gana Umara3 1Abubakar Tafawa Balewa University (ATB), PMB 0248 Bauchi, Nigeria Agricultural and Bioresource Engineering Department 2Universiti Putra Malaysia, 43400 Selangor, DE, Malaysia Department of Biological and Agricultural Engineering 3University of Maiduguri, Nigeria Department of Agricultural and Environmental Engineering *Corresponding author: e-mail: [email protected], [email protected], [email protected], [email protected] ABSTRACT Water for traditional irrigation on flood-plains in Bauchi State is obtained from the Jama’are, Gongola and Komadugu river systems. -

Local Government Areas of Bauchi State
International Journal of Engineering and Modern Technology ISSN 2504-8848 Vol. 1 No.8 2015 www.iiardpub.org An Overview of Lignocellulose in Twenty (20) Local Government Areas of Bauchi State 1Mustapha D. Ibrahim and 2Ahmad Abdurrazzaq 1Department of Chemical Engineering, Abubakar Tafawa Balewa University, Bauchi, Bauchi State, Nigeria 2Department of Chemical Engineering Technology, Federal Polytechnic Mubi, Mubi, Adamawa State, Nigeria 1E-mail: [email protected], 2E-mail: [email protected] ABSTRACT In the past few decades, there has been an increasing research interest in the value of lignocellulosic material. Lignocellulose biomass abundant holds remarkable high potentials that will go a long way in solving environmental, domestic and industrial problems if harnessed. The overview looked into only six (6) types of lignocellulose which comprised of sugar cane bagasse, corn stover, groundnut shell, sorghum residue, millet residue, and rice straw in Bauchi State. Research method adopted was by analysis of variance and percentile. The quantity of lignocelluloses studied i.e. Sugarcane bagasse, corn stover, groundnut shell, millet residue, sorghum residue and rice straw were found to be (936.7; 539,079.9; 144,352.0; 784,419.5; 905,370.6; and 73,335.5) tones/annum respectively. However, lignocellulose as a source of bioenergy in form of ethanol, the findings further revealed the estimated quantity of ethanol from sugarcane bagasse, corn stover, rice straw, sorghum, groundnut shell and millet to be at 142,462.7; 78,317,527.9; 9,339,055.9; 147,973,770.9; 18,022,347.2; and 62,322,129.3 liters/annum respectively. Keywords: lignocellulose; production capacity; energy; biomass; Bauchi INTRODUCTION Bauchi State; a state located between latitudes 9° 3´ and 12° 3´ north and longitudes 8° 50´ and 11° 0´ in the north-eastern part of Nigeria has a total land area of 49,119 km2 representing about 5.3% of the country’s total land mass and extents two distinct vegetation zones, namely the Sudan savannah and the Sahel savannah. -

Abia Adamawa Akwa Ibom
INDEPENDENT NATIONAL ELECTORAL COMMISSION 2019 GENERAL ELECTIONS HOUSE OF REPRESENTATIVES ELECTIONS HELD ON 23RD FEBRUARY AND 9TH MARCH 2019 LIST OF MEMBERS-ELECT OF THE HOUSE OF REPRESENTATIVES STATE SN CONSTITUENCY CANDIDATE GENDER PARTY REMARKS ABIA 1 ABA NORTH / ABA SOUTH OSSY EHIRIODO OSSY PRESTIGE M APGA CHINEDU 8 2 AROCHUKWU / OHAFIA NKOLE UKO NDUKWE M PDP 3 BENDE BENJAMIN OKEZIE KALU M APC 4 IKWUANO / UMUAHIA SAMUEL IFEANYI ONUIGBO M PDP NORTH / UMUAHIA SOUTH 5 ISIALA NGWA NORTH / DARLINGTON NWOKOCHA M PDP SOUTH 6 ISUIKWUATO / NKEIRUKA C. ONYEJEOCHA F APC UMUNEOCHI 7 OBINGWA / OSISIOMA / SOLOMON ADAELU M PDP UGWUNAGBO 8 UKWA EAST / UKWA WEST UZOMA NKEM ABONTA M PDP ADAMAWA 8 9 DEMSA / LAMURDE / KWAMOTI BITRUS LAORI M PDP NUMAN 10 FUFORE / SONG MUHAMMED MUSTAFA SAIDU M PDP 11 GANYE / JADA / MAYO ABDULRAZAK SA’AD NAMDAS M APC BELWA / TOUNGO 12 YOLA NORTH / YOLA ABDULRAUF ABDULKADIR MODIBBO M APC SOUTH/ GIREI 13 GOMBI / HONG YUSUF BUBA YAKUB M APC 14 GUYUK / SHELLENG GIBEON GOROKI M PDP 15 MADAGALI / MICHIKA ZAKARIA DAUDA NYAMPA M PDP 16 MAIHA / MUBI NORTH / JAAFAR ABUBAKAR MAGAJI M APC MUBI SOUTH AKWA IBOM 10 17 ABAK / ETIM EKPO / IKA ANIEKAN JOHN UMANAH M PDP 18 EKET / ESIT EKET / IBENO IFON PATRICK NATHAN M PDP / ONNA 19 IKOT EKPENE / ESSIEN IKONG NSIKAK OKON M PDP UDIM / OBOT AKARA 20 ETINAN / NSIT IBOM / NSIT ONOFIOK AKPAN LUKE M PDP UBIUM 21 UYO / URUAN /NSIT ATAI / ENYONG MICHAEL OKON M PDP ASUTAN / IBESIKPO 22 ITU /IBIONO IBOM ARCHIBONG HENRY OKON M PDP 23 IKONO / INI EMMANUEL UKPONG-UDO EFFIONG M PDP 24 IKOT ABASI / MKPAT -

OCHA Northeast Region UPDATED
NIGERIA - Northeast States: Reference Map 8.595113 9.595113 10.595113 11.595113 12.595113 13.595113 14.595113 14.009199 14.009199 NIGER CHAD Malumfatori Yusufari Abadam Yusufari Machina Kanamga Machina Yunusari Nguru Damasak Guzamala Kukawa Lake Chad Nguru Jajimaji Karasuwa Mobbar Gudumbali Geidam Kukawa Bade Gashua Bursari Gubio Bade Geidam Monguno Dapchi Gubio Gajiram Monguno JIGAWA Jakusko Nganzai Katagum Marte Magumeri Gambara Ngala Jakusko Marte Rann Gamawa Tarmua Baban Magumeri o gida YOBE Mafa Ngala Zaki Gamawa Jere Kala/Balge Fune BORNO Khaddamari Mafa Dikwa 12.009199 12.009199 Itas Itas/ Sabon Gari o Dikwa Gadau Nanger Benisheikh Maiduguri Dutse Nangere Damaturu Jama'are Azare Damban Potiskum Damagun Maiduguri Damaturu Jama'are Katagum Potiskum Kaga Konduga Damban Konduga Bama Shira Buniyadi Yana Giade Misau Bama Misau Fika Giade Fika Gujba Warji Darazo Damboa Gwoza Nafada Gwoza Ningi Warji Damboa Ningi Darazo Nafada Gulani Bara Bajoga Chibok Madagali Dukku Gulak Kafin-Madaki Biu Chibok BAUCHI Dukku Funakaye Ganjuwa Biu Askira Michika GOMBE Kwami Mallam Kwaya Askira/Uba Sidi -Kusar Biriyel Michika Kirfi Kwaya Azare Hong Toro o Mubi Kirfi Gombe Kusar Hawul o Gombe Mubi North Bauchi Bayo Hong Deba Alkaleri Shani Gombi Gella Dass Yamaltu Gombi Toro Bauchi Akko Kumo /Deba Shani Mubi South Dass Maiha Joso Balanga Shelleng 10.009199 Kaltungo Guyuk 10.009199 Billiri Shelleng Alkaleri Kaltungo Song Tafawa- Tallase Maiha Tafawa-Balewa Billiri Song Balewa Boh Guyuk Bogoro Shomgom Larmurde ADAMAWA Bogoro Lamurde Numan Girei Lac de Lere -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -

Final Report Nigeria: Yellow Fever
Final Report Nigeria: Yellow Fever DREF operation Operation n° MDRNG027 Date of Issue: 21 May 2020 Glide number: EP-2019-000112-NGA Date of disaster: 1 August, 2019 Operation start date: 20 September 2019 Operation end date: 20 December 2019 Host National Society: Nigerian Red Cross Society Operation budget: CHF 165,635 Number of people affected: Number of people assisted: 1,669,757 (278,292 HHs) - Katsina: 1,055,535 (Male: 578,239, Female: 477,296) - Bauchi: 1,044,546 persons (174,091 - 614,222 Male: 298,072 Female: 316,150) households) Bauchi: ( , - Katsina: 4,975,400 (pop of 20 LGAs) N° of National Societies involved in the operation: 01 (Nigerian RC) N° of other partner organizations involved in the operation: Federal Ministry of Health - National Primary Health Care Development Agency (FMOH-NPHCDA), State Ministry of Health (SMOH), Nigerian Centre for Disease Control (NCDC), State Primary Health Care Development Agency (SPHCDA), MSF, WHO and UNICEF The major donors and partners of the Disaster Relief Emergency Fund (DREF) include the Red Cross Societies and governments of Belgium, Britain, Canada, Denmark, Germany, Ireland, Italy, Japan, Luxembourg, New Zealand, Norway, Republic of Korea, Spain, Sweden and Switzerland, as well as DG ECHO and Blizzard Entertainment, Mondelez International Foundation, and Fortive Corporation and other corporate and private donors. DG ECHO, the Belgian Government and the Canadian Government contributed in replenishing the DREF for this operation. On behalf of Nigerian Red Cross Society (NRCS), the IFRC would like to extend gratitude to all for their generous contributions. A. SITUATION ANALYSIS Description of the disaster In August 2019, the country had recorded an increase in the number of yellow fever cases in Katsina, Bauchi and Benue States. -
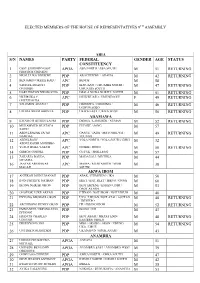
List of the Elected House of Representatives Members for the 9Th Assembly
ELECTED MEMBERS OF THE HOUSE OF REPRESENTATIVES 9TH ASSEMBLY ABIA S/N NAMES PARTY FEDERAL GENDER AGE STATUS CONSTITUENCY 1 OSSY EHIRIODO OSSY APGA ABA NORTH / ABA SOUTH M 51 RETURNING PRESTIGE CHINEDU 2 NKOLE UKO NDUKWE PDP AROCHUKWU / OHAFIA M 42 RETURNING 3 BENJAMIN OKEZIE KALU APC BENDE M 58 4 SAMUEL IFEANYI PDP IKWUANO / UMUAHIA NORTH / M 47 RETURNING ONUIGBO UMUAHIA SOUTH 5 DARLINGTON NWOKOCHA PDP ISIALA NGWA NORTH / SOUTH M 51 RETURNING 6 NKEIRUKA C. APC ISUIKWUATO / UMUNEOCHI F 49 RETURNING ONYEJEOCHA 7 SOLOMON ADAELU PDP OBINGWA / OSISIOMA / M 46 RETURNING UGWUNAGBO 8 UZOMA NKEM ABONTA PDP UKWA EAST / UKWA WEST M 56 RETURNING ADAMAWA 9 KWAMOTI BITRUS LAORI PDP DEMSA / LAMURDE / NUMAN M 52 RETURNING 10 MUHAMMED MUSTAFA PDP FUFORE / SONG M 57 SAIDU 11 ABDULRAZAK SA’AD APC GANYE / JADA / MAYO BELWA / M 49 RETURNING NAMDAS TOUNGO 12 ABDULRAUF APC YOLA NORTH / YOLA SOUTH/ GIREI M 32 ABDULKADIR MODIBBO 13 YUSUF BUBA YAKUB APC GOMBI / HONG M 50 RETURNING 14 GIBEON GOROKI PDP GUYUK / SHELLENG M 57 15 ZAKARIA DAUDA PDP MADAGALI / MICHIKA M 44 NYAMPA 16 JAAFAR ABUBAKAR APC MAIHA / MUBI NORTH / MUBI M 38 MAGAJI SOUTH AKWA IBOM 17 ANIEKAN JOHN UMANAH PDP ABAK / ETIM EKPO / IKA M 50 18 IFON PATRICK NATHAN PDP EKET / ESIT EKET / IBENO / ONNA M 60 19 IKONG NSIKAK OKON PDP IKOT EKPENE / ESSIEN UDIM / M 53 OBOT AKARA 20 ONOFIOK LUKE AKPAN PDP ETINAN / NSIT IBOM / NSIT UBIUM M 40 21 ENYONG MICHAEL OKON PDP UYO / URUAN /NSIT ATAI / ASUTAN M 48 RETURNING / IBESIKPO 22 ARCHIBONG HENRY OKON PDP ITU /IBIONO IBOM M 52 RETURNING 23 EMMANUEL UKPONG-UDO -

OCHA Northeast Region UPDATED Copy
NIGERIA - Northeast States: Reference Map 8.595113 9.595113 10.595113 11.595113 12.595113 13.595113 14.595113 14.009199 14.009199 NIGER CHAD Malumfatori Yusufari Abadam Yusufari Machina Kanamga Machina Yunusari Nguru Damasak Guzamala Kukawa Lake Chad Nguru Jajimaji Karasuwa Mobbar Gudumbali Geidam Kukawa Bade Gashua Bursari Gubio Bade Geidam Monguno Dapchi Gubio Gajiram Monguno JIGAWA Jakusko Nganzai Katagum Marte Magumeri Gambara Ngala Jakusko Marte Rann Gamawa Tarmua Baban Magumeri o gida YOBE Mafa Ngala Zaki Gamawa Jere Kala/Balge Fune BORNO Khaddamari Mafa Dikwa 12.009199 12.009199 Itas Itas/ Sabon Gari o Dikwa Gadau Nanger Benisheikh Maiduguri Dutse Nangere Damaturu Jama'are Azare Damban Potiskum Damagun Maiduguri Damaturu Jama'are Katagum Potiskum Kaga Konduga Damban Konduga Bama Shira Buniyadi Yana Giade Misau Bama Misau Fika Giade Fika Gujba Warji Darazo Damboa Gwoza Nafada Gwoza Ningi Warji Damboa Ningi Darazo Nafada Gulani Bara Bajoga Chibok Madagali Dukku Gulak Kafin-Madaki Biu Chibok BAUCHI Dukku Funakaye Ganjuwa Biu Askira Michika GOMBE Kwami Mallam Kwaya Askira/Uba Sidi -Kusar Biriyel Michika Kirfi Kwaya Azare Hong Toro o Mubi Kirfi Gombe Kusar Hawul o Gombe Mubi North Bauchi Bayo Hong Deba Alkaleri Shani Gombi Gella Dass Yamaltu Gombi Toro Bauchi Akko Kumo /Deba Shani Mubi South Dass Maiha Joso Balanga Shelleng 10.009199 Kaltungo Guyuk 10.009199 Billiri Shelleng Alkaleri Kaltungo Song Tafawa- Tallase Maiha Tafawa-Balewa Billiri Song Balewa Boh Guyuk Bogoro Shomgom Larmurde ADAMAWA Bogoro Lamurde Numan Girei Lac de Lere