Dorsalis Pedis Artery As a Continuation of Peroneal Artery—Clinical and Embryological Aspects Seema Sehmi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Classification System of the Tibiofibular Syndesmosis Blood Supply and Its
www.nature.com/scientificreports OPEN Classifcation system of the tibiofbular syndesmosis blood supply and its clinical relevance Received: 16 February 2018 Izabela Mróz1, Piotr J. Bachul1,2, Krzysztof A. Tomaszewski1, Tomasz Bereza1, Krzysztof Gil3, Accepted: 7 June 2018 Jerzy A. Walocha1 & Artur Pasternak 1 Published: xx xx xxxx Due to the lack of anatomical studies concerning complexity of the tibiofbular syndesmosis blood supply, density of blood vessels with further organization of syndesmotic vascular variations is presented in clinically relevant classifcation system. The material for the study was obtained from cadaveric dissections. We dissected 50 human ankles observing diferent types of arterial blood supply. Our classifcation system is based on the vascular variations of the anterior aspect of tibiofbular syndesmosis and corresponds with vascular density. According to our study the mean vascular density of tibiofbular syndesmosis is relatively low (4.4%) and depends on the type of blood supply. The highest density was observed among ankles with complete vasculature and the lowest when lateral anterior malleolar artery was absent (5.8% vs. 3.5%, respectively). Awareness of various types of tibiofbular syndesmosis arterial blood supply is essential for orthopedic surgeons who operate in the ankle region and radiologists for the anatomic evaluation of this area. Knowledge about possible variations along with relatively low density of vessels may contribute to modifcation of treatment approach by the increase of the recommended time of syndesmotic screw stabilization in order to prevent healing complications. Tibiofbular syndesmosis is a fbrous connection localized between the fbular notch of the tibia and medial surface of the lateral ankle. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Reconstructive
RECONSTRUCTIVE Angiosomes of the Foot and Ankle and Clinical Implications for Limb Salvage: Reconstruction, Incisions, and Revascularization Christopher E. Attinger, Background: Ian Taylor introduced the angiosome concept, separating the M.D. body into distinct three-dimensional blocks of tissue fed by source arteries. Karen Kim Evans, M.D. Understanding the angiosomes of the foot and ankle and the interaction among Erwin Bulan, M.D. their source arteries is clinically useful in surgery of the foot and ankle, especially Peter Blume, D.P.M. in the presence of peripheral vascular disease. Paul Cooper, M.D. Methods: In 50 cadaver dissections of the lower extremity, arteries were injected Washington, D.C.; New Haven, with methyl methacrylate in different colors and dissected. Preoperatively, each Conn.; and Millburn, N.J. reconstructive patient’s vascular anatomy was routinely analyzed using a Dopp- ler instrument and the results were evaluated. Results: There are six angiosomes of the foot and ankle originating from the three main arteries and their branches to the foot and ankle. The three branches of the posterior tibial artery each supply distinct portions of the plantar foot. The two branches of the peroneal artery supply the anterolateral portion of the ankle and rear foot. The anterior tibial artery supplies the anterior ankle, and its continuation, the dorsalis pedis artery, supplies the dorsum of the foot. Blood flow to the foot and ankle is redundant, because the three major arteries feeding the foot have multiple arterial-arterial connections. By selectively performing a Doppler examination of these connections, it is possible to quickly map the existing vascular tree and the direction of flow. -

Vascular Anatomy of the Free Fibula Flap Including the Lateral Head of the Soleus Muscle Applied to Maxillo-Mandibular Reconstruction
Surgical and Radiologic Anatomy (2019) 41:447–454 https://doi.org/10.1007/s00276-018-2166-2 ORIGINAL ARTICLE Vascular anatomy of the free fibula flap including the lateral head of the soleus muscle applied to maxillo-mandibular reconstruction Lara Nokovitch1,2 · Julien Davrou2 · François Bidault4 · Bernard Devauchelle2 · Stéphanie Dakpé2 · Christian Vacher3,5 Received: 1 May 2018 / Accepted: 8 December 2018 / Published online: 14 December 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract Purpose Initially described by Baudet in 1982, the fibula flap including the lateral head of the soleus muscle allows a one- stage reconstruction for large maxillo-mandibular defects. The aim of this study was to evaluate the number of muscular branches destined to the soleus muscle and their distance from the origin of the fibular artery, to assess the vascular anatomy of the free fibula flap including the lateral head of the soleus muscle applied to maxillo-mandibular reconstruction. Methods We performed a cadaveric anatomic study on ten lower limbs, and a CT angiography anatomic study on 38 legs. The number of soleus branches originating from the fibular artery, and the distance between the origin of the fibular artery and each of the identified branches were measured. Results The number of soleus branches destined to the lateral head of the soleus muscle is variable, with in our study 1–3 branches found. Soleus branches destined to the lateral head of the soleus muscle emerged at a distance ranging between 0 and 2.9 cm (mean value = 1.82 cm) from the origin of the fibular artery in 40% of cases, between 3 and 5.9 cm (mean value = 4.27 cm) from the origin of the fibular artery in 37% of cases, and was at a distance of 6 cm or more (mean value = 6.93 cm) from the origin of the fibular artery in 20% of cases. -

Femoral Injecting Guide
FEMORAL INJECTING A GUIDE TO INJECTING IN THE GROIN USING THE FEMORAL VEIN (This is a restricted document NOT meant for general distribution) AUGUST 2006 1 INTRODUCTION INTRODUCTION This resource has been produced by some older intravenous drug users (IDU’s) who, having compromised the usual injecting sites, now inject into the femoral vein. We recognize that many IDU’s continue to use as they grow older, but unfortunately, easily accessible injecting sites often become unusable and viable sites become more dif- ficult to locate. Usually, as a last resort, committed IDU’s will try to locate one of the larger, deeper veins, especially when injecting large volumes such as methadone. ManyUnfortunately, of us have some had noof usalternat had noive alternative but to ‘hit butand to miss’ ‘hit andas we miss’ attempted as we attemptedto find veins to find that weveins couldn’t that we see, couldn’t but knew see, werebut knew there. were This there. was often This painful,was often frustrating, painful, frustrating, costly and, costly in someand, cases,in some resulted cases, inresulted permanent in permanent injuries such injuries as the such example as the exampleshown under shown the under the heading “A True Story” on pageheading 7. “A True Story” on page 7. CONTENTS CONTENTS 1) Introduction, Introduction, Contents contents, disclaimer 9) Rotating Injecting 9) Rotating Sites Injecting Sites 2) TheFemoral Femoral Injecting: Vein—Where Getting is Startedit? 10) Blood Clots 10) Blood Clots 3) FemoralThe Femoral Injecting: Vein— Getting Where -

Current Overview of Neurovascular Structures in Hip Arthroplasty
1mon.qxd 2/2/04 10:26 AM Page 73 REVIEW Current Overview of Neurovascular Structures in Hip Arthroplasty: Anatomy, Preoperative Evaluation, Approaches, and Operative Techniques to Avoid Complications John-Paul H. Rue, MD* Nozomu Inoue, MD, PhD* Michael A. Mont, MD† A major neurovascular injury during total hip arthroplasty (THA) is uncom- Educational Objectives mon. Nevertheless, these are worri- some due to their devastating conse- As a result of reading this article, physicians should be able to: quences. As more THAs are performed 1. Identify the bony, vascular, and neural anatomy that is relevant to the each year, the chances of this potential- surgeon performing total hip arthroplasty. ly life- or limb-threatening injury 2. Describe the common approaches to avoid neurovascular complica- increase.1 It is crucial for the orthope- tions. dic surgeon to have a thorough under- 3. Discuss the appropriate clinical work-up of these patients. standing of the anatomy of the region 4. Describe the various neurovascular complications and how to handle and the potential complications. them. This article reviews the exposures to the acetabulum for simple and complex primary THA, as well as revision cases, with particular attention to the neu- ischium, and pubis (Figure 1). The Damage to any of these vessels by rovascular anatomy of the region. acetabulum is located at the junction of retraction, drilling, reaming, or dissec- these three bones. These bones unite tion can cause massive hemorrhage, ANATOMY anteriorly at the pubic symphysis and which can lead to exsanguination with- Bone posteriorly to the sacrum to form a ring in minutes. -

The Inferior Epigastric Artery: Anatomical Study and Clinical Significance
Int. J. Morphol., 35(1):7-11, 2017. The Inferior Epigastric Artery: Anatomical Study and Clinical Significance Arteria Epigástrica Inferior: Estudio Anatómico y Significancia Clínica Waseem Al-Talalwah AL-TALALWAH, W. The inferior epigastric artery: anatomical study and clinical significance. Int. J. Morphol., 35(1):7-11, 2017. SUMMARY: The inferior epigastric artery usually arises from the external iliac artery. It may arise from different origin. The aim of current study is to provide sufficient date of the inferior epigastric artery for clinician, radiologists, surgeons, orthopaedic surgeon, obstetricians and gynaecologists. The current study includes 171 dissected cadavers (92 male and 79 female) to investigate the origin and branch of the inferior epigastric artery in United Kingdom population (Caucasian) as well as in male and female. The inferior epigastric artery found to be a direct branch arising independently from the external iliac artery in 83.6 %. Inferior epigastric artery arises from common trunk of external iliac artery with the obturator artery or aberrant obturator artery in 15.1 % or 1.3 %. Further, the inferior epigastric artery gives obturator and aberrant obturator branch in 3.3 % and 0.3 %. Therefore, the retropubic connection vascularity is 20 % which is more in female than male. As the retropubic region includes a high vascular variation, a great precaution has to be considered prior to surgery such as hernia repair, internal fixation of pubic fracture and skin flap transplantation. The radiologists have to report treating physicians to decrease intra-pelvic haemorrhage due to iatrogenic lacerating obturator or its accessory artery KEY WORDS: Inferior epigastric; Obturator; Aberrant Oburator; Accessory Obturator; Hernia; Corona Mortis; Pubic fracture. -
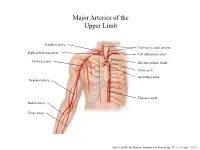
Major Arteries of the Upper Limb
Major Arteries of the Upper Limb Vertebral artery Common carotid arteries Right subclavian artery Left subclavian artery Axillary artery Brachiocephalic trunk Aortic arch Ascending aorta Brachial artery Thoracic aorta Radial artery Ulnar artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.23 Major Arteries of the Abdominal Region Renal artery Celiac trunk Abdominal aorta Superior mesenteric artery Gonadal artery Inferior mesenteric artery Common iliac artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.24 Common iliac artery Internal iliac artery Major Arteries of the External iliac artery Lower Limb Femoral artery Popliteal artery Anterior tibial artery Fibular artery Posterior tibial artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.25 Major Veins of the Upper Limb Internal jugular vein (left) Subclavian vein (right) External jugular vein (left) Axillary vein Brachiocephalic veins Cephalic vein Superior vena cava Brachial vein Basilic vein Median cubital vein Inferior vena cava Radial vein Ulnar vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.28 Major Veins of the Abdominal Cavity – Part 1 Hepatic veins Inferior vena cava Renal vein (left) Gonadal vein (left) Gonadal vein (right) Common iliac vein (left) Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Major Veins of the Abdominal Cavity – Part 2 (Hepatic portal circulation) Hepatic portal vein Splenic vein Inferior mesenteric vein Superior mesenteric vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Common iliac vein (left) Internal iliac vein Major Veins of the External iliac vein Lower Limb Great saphenous vein Femoral vein Popliteal vein Fibular vein Small saphenous vein Anterior tibial Posterior tibial vein vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.30 . -

Presence of the Dorsalis Pedis Artery in Young and Healthy Individuals
Wilson G. Hunt Russell H. Samson M.D Ravi K. Veeraswamy M.D Financial Disclosures I have no financial disclosures Objective To determine the presence of the dorsalis pedis in young healthy individuals To confirm antegrade flow into the foot Reason The dorsalis pedis artery has been reported absent, ranging from 2-10%, in most reported series (Clinical Method: The History, Physical, and Laboratory Examinations 3rd edition 1990 Dean Hill, Robert Smith III) Clinical relevance of an absent dorsalis pedis pulse Understanding the rates of absent dorsalis pedis provides a baseline for clinical examinations Following arterial trauma, an absent pulse may be mistaken for a congenitally absent pulse An absent dorsalis pedis in elderly patients may be mistaken as a sign of peripheral arterial disease Prior methods to determine presence of the Dorsalis Pedis Palpation(Stephens 1962) 4.5% Absent 40 year old men Issues Unreliable Subjective Prior methods to determine presence of the Dorsalis Pedis Dissection(Rajeshwari et. Al 2013) 9.5% Absent Issues Unhealthy subjects Prior methods to determine presence of the Dorsalis Pedis Doppler (Robertson et. Al 1990) Absent in 2% Age 15-30 Issues: Older technology Cannot determine direction of flow ○ Flow may be retrograde from the PT via the plantar arch Question Impalpable or truly absent? If absent, is it congenital or due to disease or trauma? Hypothesis A younger population along with improved technology should be more reliable to detect the dorsalis pedis artery Methods 100 young -

A Study of the Internal Diameter of Popliteal Artery, Anterior and Posterior Tibial Arteries in Cadavers
Original Research Article A study of the internal diameter of popliteal artery, anterior and posterior tibial arteries in cadavers Anjali Vishwanath Telang1,*, Mangesh Lone2, M Natarajan3 1Assistant Professor, 3Professor, Dept. of Anatomy, Seth GS Medical College, Parel, Mumbai, Maharashtra, 2Assistant Professor, Dept. of Anatomy, LTMMC, Sion, Mumbai, Maharashtra *Corresponding Author: Anjali Vishwanath Telang Assistant Professor, Dept. of Anatomy, Seth GS Medical College, Mumbai, Maharashtra Email: [email protected] Abstract Introduction: Popliteal artery is the continuation of femoral artery at adductor hiatus. It is one of the most common sites for peripheral aneurysms. It is also a common recipient site for above or below knee femoro-popliteal bypass grafts in cases of atherosclerosis. The aim was to study the internal diameter of popliteal artery, anterior tibial and posterior tibial arteries and to compare findings of the current study with previous studies and to find their clinical implications. Methods: Fifty cadavers (100 lower limbs) embalmed with 10% formalin were utilised in this study. Results: Internal diameter of popliteal artery was measured at its origin and at its termination. The diameter of popliteal artery at its origin was found to be (mean in mm ± SD) 4.7±0.9 & at its termination was 4.4±0.7. The diameter of anterior tibial artery at its origin was 3.5±1.1 & that of posterior tibial artery at its origin was 4.1±0.9. These findings were compared with the previous studies. Conclusion: Metric data of internal diameter of popliteal artery, anterior tibial artery & posterior tibial artery from the present study will be of help for vascular surgeons & radiologists. -

Intriguing Variations of Dorsalis Pedis Artery with Clinical Correlations P
Scholars International Journal of Anatomy and Physiology Abbreviated Key Title: Sch Int J Anat Physiol ISSN 2616-8618 (Print) |ISSN 2617-345X (Online) Scholars Middle East Publishers, Dubai, United Arab Emirates Journal homepage: https://scholarsmepub.com/sijap/ Original Research Article Intriguing Variations of Dorsalis Pedis Artery with Clinical Correlations P. J. Barot1, P. R. Koyani2* 1Tutor, Department of Anatomy, P. D. U. Medical College, Rajkot, Gujarat, India 2 Assistant Professor, Department of Anatomy, P. D. U. Medical College, Rajkot, Gujarat, India DOI: 10.36348/SIJAP.2019.v02i12.001 | Received: 24.11.2019 | Accepted: 04.12.2019 | Published: 06.12.2019 *Corresponding author: P. R. Koyani Abstract Objective: Dorsalis pedis artery represents the continuation of anterior tibial artery distal to level of ankle joint. The dorsalis pedis angiosome encompasses the entire dorsal aspect of foot through its branches eg. Medial tarsal, Lateral tarsal, Arcuate and 1st dorsal metatarsal arteries. Dorsalis pedis artery variation have been reported in past. Evaluation of dorsalis pedis artery pulsation is useful clinical test for assessing peripheral arterial diseases. Dorsalis pedis artery is the main source of blood supply to foot. Knowledge about origins, course, distribution and branching pattern is important for angiographers, vascular surgeons and reconstructive surgeons who operate upon these region. Method: Study of dorsalis pedis artery was done in forty dissected lower limbs of unknown sex and age from department of anatomy, PDUMC, RAJKOT. Result: In our study normal course and branching pattern of dorsalis pedis artery was found in 87.5% cases. Variation in branching pattern of dorsalis pedis artery was found in 12.5% cases. -

The Anatomy of the Plantar Arterial Arch
Int. J. Morphol., 33(1):36-42, 2015. The Anatomy of the Plantar Arterial Arch Anatomía del Arco Plantar Arterial A. Kalicharan*; P. Pillay*; C. Rennie* & M. R. Haffajee* KALICHARAN, A.; PILLAY, P.; RENNIE, C. & HAFFAJEE, M. R. The anatomy of the plantar arterial arch. Int. J. Morphol., 33(1):36-42, 2015. SUMMARY: The plantar arterial arch provides the dominant vascular supply to the digits of the foot, with variability in length, shape, and dominant blood supply from the contributing arteries. According to the standard definition, the plantar arterial arch is formed from the continuation of the lateral plantar artery and the anastomoses between the deep branch of dorsalis pedis artery. In this study, 40 adult feet were dissected and the plantar arch with variations in shape and arterial supply was observed. The standard description of the plantar arch was observed in 55% of the specimens with variations present in 45%. Variations in terms of shape were classified into three types: Type A (10%): plantar arterial arch formed a sharp irregular curve; type B (60%): obtuse curve; type C (3%): spiral curve. Variation in the dominant contributing artery was classified into six types: type A (25%), predominance in the deep branch of dorsalis pedis artery supplying all digits; type B (5%), predominance in the lateral plantar artery supplying digits 3 and 4; and type C (20%), predominance in the deep branch of dorsalis pedis artery supplying digits 2 to 4; type D (24%), equal dominance showed; type E (10%), predominance in the lateral plantar artery supplying digits 3 to 5; and type F (21%), predominance of all digits supplied by lateral plantar artery.