Research Article the Use of Multiple Correspondence Analysis to Explore Associations Between Categories of Qualitative Variables in Healthy Ageing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Correspondence Analysis
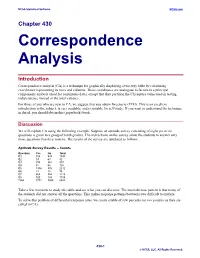
NCSS Statistical Software NCSS.com Chapter 430 Correspondence Analysis Introduction Correspondence analysis (CA) is a technique for graphically displaying a two-way table by calculating coordinates representing its rows and columns. These coordinates are analogous to factors in a principal components analysis (used for continuous data), except that they partition the Chi-square value used in testing independence instead of the total variance. For those of you who are new to CA, we suggest that you obtain Greenacre (1993). This is an excellent introduction to the subject, is very readable, and is suitable for self-study. If you want to understand the technique in detail, you should obtain this (paperback) book. Discussion We will explain CA using the following example. Suppose an aptitude survey consisting of eight yes or no questions is given to a group of tenth graders. The instructions on the survey allow the students to answer only those questions that they want to. The results of the survey are tabulated as follows. Aptitude Survey Results – Counts Question Yes No Total Q1 155 938 1093 Q2 19 63 82 Q3 395 542 937 Q4 61 64 125 Q5 1336 876 2212 Q6 22 14 36 Q7 864 354 1218 Q8 920 185 1105 Total 3772 3036 6808 Take a few moments to study this table and see what you can discover. The most obvious pattern is that many of the students did not answer all the questions. This makes response patterns between rows difficult to analyze. To solve this problem of differential response rates, we create a table of row percents (or row profiles as they are called in CA). -

A Correspondence Analysis of Child-Care Students' and Medical
International Education Journal Vol 5, No 2, 2004 http://iej.cjb.net 176 A Correspondence Analysis of Child-Care Students’ and Medical Students’ Knowledge about Teaching and Learning Helen Askell-Williams Flinders University School of Education [email protected] Michael J. Lawson Flinders University School of Education [email protected] This paper describes the application of correspondence analysis to transcripts gathered from focussed interviews about teaching and learning held with a small sample of child-care students, medical students and the students’ teachers. Seven dimensions emerged from the analysis, suggesting that the knowledge that underlies students’ learning intentions and actions is multi-dimensional and transactive. It is proposed that the multivariate, multidimensional, discovery approach of the correspondence analysis technique has considerable potential for data analysis in the social sciences. Teaching, learning, knowledge, correspondence analysis INTRODUCTION The purpose of this paper is to describe the application of correspondence analysis to rich text- based data derived from interviews with teachers and learners about their knowledge about teaching and learning. Correspondence analysis is a non-linear, multidimensional technique of multivariate descriptive analysis that “specialises in ‘discovering,’ through detailed analysis of a given data set” (Nishisato, 1994 p.7). A description of what teachers and learners know about teaching and learning will assist in developing the educational community’s understanding about teaching and learning. If researchers, designers and policy makers are well informed about teachers’ and learners’ knowledge, they will be better equipped to design and recommend educational programs that meet students’ learning needs. If teachers possess high quality knowledge about their own, and their students’, knowledge then they will be better equipped to design and deliver high quality teaching. -

449, 468 Across-Stage Inferencing 568, 57
xxxv Index 6 Cs 1254, 1258 Apriori-based Graph Mining (AGM) 13 6 Ps 1253 Apriori with Subgroup and Constraint (ASC) 948 Arabidopsis thaliana 205, 227 A ArM32 operations 458 ArnetMiner 331 abnormal alarm 2183 Arterial Pressure (AP) 902 academic theory 1678 ArTex with Resolutions (ARes) 1047 Access Methods (AM) 449, 468 arthrokinetics restrictions 653 across-stage inferencing 568, 575-576, 580, 583 Artificial Intelligence (AI) 991, 1262 Active Learning (AL) 67, 69 Artificial Neural Networks (ANN) 250, 299, 367, 704, ADaMSoft 1315 1114, 1573, 2253 Adaptive Modulation and Coding (AMC) 345 Art of War 477 Adaptive Neuro Fuzzy Inference System (ANFIS) Asset Management (AM) 1607 1114-1115, 1124, 2250, 2252, 2254-2255, 2268 Association Rule Mining (ARM) 28, 47, 108, 148, Additive White Gaussian Noise (AWGN) 2084 684, 856, 974, 989, 1740 advanced search 1314, 1317, 1338 ANGEL data 846-847 Adverse Drug Events (ADEs) 1942 approaches 1739-1740, 1743, 1748-1749 Agglomerative Hierarchical Clustering (AHC) 1435 association rules 57, 65, 587 aggregate constraint 1842 calendric 594 aggregate function 681-682, 686, 1434, 1842, 2028- maximal 503-509, 512-514 2029 quality measures 130 agrometeorological agents 1625 Association rules for Textures (ArTex) 1047 agrometeorological methods 1625-1626 Associative Classification (AC) 975 agrometeorological variables 1626 atomic condition 285-287 ambiguity-directed sampling 71 Attention Deficit Hyperactivity Disorder (ADHD) American Bureau of Shipping (ABS) 2175 1463 American National Election Studies (ANES) 30, 42 -

Correspondence Analysis and Classification Gilbert Saporta, Ndeye Niang Keita
Correspondence analysis and classification Gilbert Saporta, Ndeye Niang Keita To cite this version: Gilbert Saporta, Ndeye Niang Keita. Correspondence analysis and classification. Michael Greenacre; Jörg Blasius. Multiple Correspondence Analysis and Related Methods, Chapman and Hall/CRC, pp.371-392, 2006, 9781584886280. hal-01125202 HAL Id: hal-01125202 https://hal.archives-ouvertes.fr/hal-01125202 Submitted on 23 Mar 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. CORRESPONDENCE ANALYSIS AND CLASSIFICATION Gilbert Saporta, Ndeye Niang The use of correspondence analysis for discrimination purposes goes back to the “prehistory” of data analysis (Fisher, 1940) where one looks for the optimal scaling of categories of a variable X in order to predict a categorical variable Y. When there are several categorical predictors a commonly used technique consists in a two step analysis: multiple correspondence on the predictors set, followed by a discriminant analysis using factor coordinates as numerical predictors (Bouroche and al.,1977). However in banking applications (credit scoring) logistic regression seems to be more and more used instead of discriminant analysis when predictors are categorical. One of the reasons advocated in favour of logistic regression, is that it gives a probabilistic model and it is often claimed among econometricians that the theoretical basis is more solid, but this is arguable. -

Implementing and Interpreting Canonical Correspondence Analysis in SAS Laxman Hegde, Frostburg State University, Frostburg, MD
NESUG 2012 Statistics, Modeling and Analysis Implementing and Interpreting Canonical Correspondence Analysis in SAS Laxman Hegde, Frostburg State University, Frostburg, MD ABSTRACT Canonical Correspondence Analysis (CCPA)1 is a popular method among ecologists to study species environmental correlations using Generalized Singular Value Decomposition (GSVD) of a proper matrix. CCPA is not so popular among researchers in other fields. Given two matrices Y( n by m) and Z( n by q), CCPA involves computing GSVD of another matrix A( m by q) which can be thought of as a weighted averages for the columns of Z using the frequencies (the row totals) in Y matrix. The SAS output for CCPA has several interesting parts (algebraically, numerically and graphically) that require interpretations to end users. In our presentation, we like to show how to perform CCPA in SAS/IML and interpret a few important results. The climax of this program is about constructing a Biplot of the A matrix. Keywords: Canonical Correspondence Analysis, Singular Value Decomposition, Biplot, Species Scores, Sample Scores, Species-Environmental Correlations. INTRODUCTION Principal component analysis (PCA), Canonical Correlation Analysis(CCA), and Correspondence Analysis (CA) are the well known multivariate data reduction techniques. The first two methods deal with an analysis of a correlation or variance-covariance matrix of a multivariate quantitative data set and the correspondence analysis deals with an analysis of data in a contingency table. It is well known that the general theory of all these methods is essentially based on the Singular Value Decomposition (SVD) of a real rectangular data matrix that is being processed. For various applications of SVD in CA and other multivariate methods, see Greenacre (1984). -

Measuring Explained Variance in Multiple Correspondence Analysis
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Research Papers in Economics 1 Biplots of fuzzy coded data Zerrin Aşan1 and Michael Greenacre2 1Department of Statistics, Anadolu University, Eskişehir, Turkey Email: [email protected] 2Department of Economics and Business, Universitat Pompeu Fabra, Barcelona, Spain Email: [email protected] Abstract A biplot, which is the multivariate generalization of the two-variable scatterplot, can be used to visualize the results of many multivariate techniques, especially those that are based on the singular value decomposition. We consider data sets consisting of continuous-scale measurements, their fuzzy coding and the biplots that visualize them, using a fuzzy version of multiple correspondence analysis. Of special interest is the way quality of fit of the biplot is measured, since it is well-known that regular (i.e., crisp) multiple correspondence analysis seriously under-estimates this measure. We show how the results of fuzzy multiple correspondence analysis can be defuzzified to obtain estimated values of the original data, and prove that this implies an orthogonal decomposition of variance. This permits a measure of fit to be calculated in the familiar form of a percentage of explained variance, which is directly comparable to the corresponding fit measure used in principal component analysis of the original data. The approach is motivated initially by its application to a simulated data set, showing how the fuzzy approach can lead to diagnosing nonlinear relationships, and finally it is applied to a real set of meteorological data. Key words: defuzzification, fuzzy coding, indicator matrix, measure of fit, multivariate data, multiple correspondence analysis, principal component analysis. -

Correspondence Analysis
Title: Correspondence Analysis Name: Herv´eAbdi1, Michel B´era2 Affil./Addr. 1: School of Behavioral and Brain Sciences The University of Texas at Dallas Richardson, TX 75080, USA [email protected] Affil./Addr. 2: Centre d'Etude´ et de Recherche en Informatique et Communica- tions Conservatoire National des Arts et M´etiers F-75141 Paris Cdex 03, France [email protected] Correspondence Analysis Synonyms Dual Scaling, optimal scaling, homogeneity analysis. Glossary CA: Correspondence analysis component: A linear combination of the variables of a data table dimension: see component factor: see component GSVD: Generalized singular value decomposition PCA: Principal component analysis SVD: Singular value decomposition 2 Introduction Correspondence analysis [ca; see 11; 22; 21; 13; 16; 17; 7; 20; 1; 9] is an extension of principal component analysis (pca, for details, see [8]) tailored to handle nominal variables. Originally, ca was developed to analyze contingency tables in which a sam- ple of observations is described by two nominal variables, but it was rapidly extended to the analysis of any data matrices with non-negative entries. The origin of ca can be traced to early work of Pearson ([24]) or Fisher, but the modern version of corre- spondence analysis and its geometric interpretation comes from the 1960s in France and is associated with the French school of \data analysis" (analyse des donn ´ees) and was developed under the leadership of Jean-Paul Benz´ecri.As a technique, it was often discovered (and re-discovered) and so variations of ca can be found under several different names such as \dual-scaling," \optimal scaling," \homogeneity analysis," or \reciprocal averaging," The multiple identities of correspondence analysis are a conse- quence of its large number of properties: Correspondence analysis can be defined as an optimal solution for a lot of apparently different problems. -

The Geometric Interpretation of Correspondence Analysis Author(S): Michael Greenacre and Trevor Hastie Source: Journal of the American Statistical Association, Vol
The Geometric Interpretation of Correspondence Analysis Author(s): Michael Greenacre and Trevor Hastie Source: Journal of the American Statistical Association, Vol. 82, No. 398 (Jun., 1987), pp. 437-447 Published by: Taylor & Francis, Ltd. on behalf of the American Statistical Association Stable URL: https://www.jstor.org/stable/2289445 Accessed: 26-01-2020 22:24 UTC JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at https://about.jstor.org/terms Taylor & Francis, Ltd., American Statistical Association are collaborating with JSTOR to digitize, preserve and extend access to Journal of the American Statistical Association This content downloaded from 171.66.12.245 on Sun, 26 Jan 2020 22:24:02 UTC All use subject to https://about.jstor.org/terms The Geometric Interpretation of Correspondence Analysis MICHAEL GREENACRE and TREVOR HASTIE* Correspondence analysis is an exploratory multivariate technique that indicator (or "dummy") variables. The correspondence converts a data matrix into a particular type of graphical display in which analysis of this indicator matrix is known as multiple cor- the rows and columns are depicted as points. The method has a long respondence analysis or homogeneity analysis (Gifi 1981). and varied history and has appeared in different forms in the psycho- metric and ecological literature, among others. -

Chapter 6 Correspondence Analysis
Chapter 6 Correspondence analysis {ch:corresp} Correspondence analysis provides visualizations of associations in a two-way contin- gency table in a small number of dimensions. Multiple correspondence analysis extends this technique to n-way tables. Other graphical methods, including mosaic matrices and biplots provide complementary views of loglinear models for two-way and n-way contin- gency tables. 6.1 Introduction Whenever a large sample of chaotic elements is taken in hand and marshalled in the order of their magnitude, an unsuspected and most beautiful form of regularity proves to have been latent all along. Sir Francis Galton (1822–1911) Correspondence analysis (CA) is an exploratory technique which displays the row and col- umn categories in a two-way contingency table as points in a graph, so that the positions of the points represent the associations in the table. Mathematically, correspondence analysis is related to the biplot, to canonical correlation, and to principal component analysis. This technique finds scores for the row and column categories on a small number of dimen- sions which account for the greatest proportion of the χ2 for association between the row and column categories, just as principal components account for maximum variance of quantitative variables. But CA does more— the scores provide a quantification of the categories, and have the property that they maximize the correlation between the row and column variables. For graphical display two or three dimensions are typically used to give a reduced rank approximation to the data. Correspondence analysis has a very large, multi-national literature and was rediscovered sev- eral times in different fields and different countries. -
Biplots in Practice
www.fbbva.es Biplots in Practice Biplots in Practice MICHAEL GREENACRE First published September 2010 © Michael Greenacre, 2010 © Fundación BBVA, 2010 Plaza de San Nicolás, 4. 48005 Bilbao www.fbbva.es [email protected] A digital copy of this book can be downloaded free of charge at http://www.fbbva.es The BBVA Foundation’s decision to publish this book does not imply any responsibility for its content, or for the inclusion therein of any supplementary documents or infor- mation facilitated by the author. Edition and production: Rubes Editorial ISBN: 978-84-923846-8-6 Legal deposit no: B- Printed in Spain Printed by S.A. de Litografía This book is produced with paper in conformed with the environmental standards required by current European legislation. In memory of Cas Troskie (1936-2010) CONTENTS Preface .............................................................................................................. 9 1. Biplots—the Basic Idea............................................................................ 15 2. Regression Biplots.................................................................................... 25 3. Generalized Linear Model Biplots .......................................................... 35 4. Multidimensional Scaling Biplots ........................................................... 43 5. Reduced-Dimension Biplots.................................................................... 51 6. Principal Component Analysis Biplots.................................................... 59 7. Log-ratio Biplots...................................................................................... -

Chapter 11 Correspondence Analysis
Chapter 11 Correspondence Software and Documentation by: Bee-LengAnalysis Lee This chapter describes ViSta-Corresp, the ViSta procedure for performing simple correspondence analysis, a way of analyzing a two-way table of data. ViSta-Cor- resp can analyze row or column profiles, or both. Its visualization includes a spin- plot and scatterplot of the row and column points, a residual plot and a fit plot. ViSta-Corresp supports model re-vision. ViSta-Corresp does not perform multiple Correspondence Analysis of multi-way data. 64 Correspondence Analysis ViSta: The Visual Statistics System Introduction to Correspondence Analysis 65 11.1 Introduction to Correspondence Analysis Correspondence analysis is a statistical visualization method for picturing the asso- ciations between the levels of a two-way contingency table. The name is a transla- tion of the French Analyses des Correspondances, where the term correspondance denotes a “system of associations” between the elements of two sets. In a two-way contingency table, the observed association of two traits is summa- rized by the cell frequencies, and a typical inferential aspect is the study of whether certain levels of one charactertistic are associated with some levels of another. Cor- respondence analysis is a geometric technique for displaying the rows and columns of a two-way contingency table as points in a low-dimensional space, such that the positions of the row and column points are consistent with their associations in the table. The goal is to have a global view of the data that is useful for interpretation. To illustrate correspondence analysis, consider the multidimensional time series on the number of science doctorates conferred in the USA from 1960 to 1975 that is shown in Table 1 (Greenacre, 1984). -

Multiple Correspondence Analysis
Multiple Correspondence Analysis Hervé Abdi1 & Dominique Valentin 1 Overview Multiple correspondence analysis (MCA) is an extension of corre- spondence analysis (CA) which allows one to analyze the pattern of relationships of several categorical dependent variables. As such, it can also be seen as a generalization of principal component anal- ysis when the variables to be analyzed are categorical instead of quantitative. Because MCA has been (re)discovered many times, equivalent methods are known under several different names such as optimal scaling, optimal or appropriate scoring, dual scaling, homogeneity analysis, scalogram analysis, and quantification me- thod. Technically MCA is obtained by using a standard correspon- dence analysis on an indicator matrix (i.e., a matrix whose entries are 0 or 1). The percentages of explained variance need to be cor- rected, and the correspondence analysis interpretation of inter- point distances needs to be adapted. 1In: Neil Salkind (Ed.) (2007). Encyclopedia of Measurement and Statistics. Thousand Oaks (CA): Sage. Address correspondence to: Hervé Abdi Program in Cognition and Neurosciences, MS: Gr.4.1, The University of Texas at Dallas, Richardson, TX 75083–0688, USA E-mail: [email protected] http://www.utd.edu/ herve » 1 H. Abdi & D. Valentin: Multiple Correspondence Analysis 2 When to use it MCA is used to analyze a set of observations described by a set of nominal variables. Each nominal variable comprises several lev- els, and each of these levels is coded as a binary variable. For ex- ample gender, (F vs. M) is one nominal variable with two levels. The pattern for a male respondent will be 0 1 and 1 0 for a female.