Borno State Health Sector Bulletin Number 9
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chronologie Des Exactions À Maiduguri Et Gamboru Ngala (Etat De Borno) Entre 2011 Et 2015. NIGERIA
NIGERIA 14 juin 2018 Chronologie des exactions à Maiduguri et Gamboru Ngala (Etat de Borno) entre 2011 et 2015. Avertissement Ce document a été élaboré par la Division de l’Information, de la Documentation et des Recherches de l’Ofpra en vue de fournir des informations utiles à l’examen des demandes de protection internationale. Il ne prétend pas faire le traitement exhaustif de la problématique, ni apporter de preuves concluantes quant au fondement d’une demande de protection internationale particulière. Il ne doit pas être considéré comme une position officielle de l’Ofpra ou des autorités françaises. Ce document, rédigé conformément aux lignes directrices communes à l’Union européenne pour le traitement de l’information sur le pays d’origine (avril 2008) [cf. www.ofpra.gouv.fr/sites/default/files/atoms/files/lignes_directrices_europeennes.pdf], se veut impartial et se fonde principalement sur des renseignements puisés dans des sources qui sont à la disposition du public. Toutes les sources utilisées sont référencées. Elles ont été sélectionnées avec un souci constant de recouper les informations. Le fait qu’un événement, une personne ou une organisation déterminée ne soit pas mentionné(e) dans la présente production ne préjuge pas de son inexistence. La reproduction ou diffusion du document n’est pas autorisée, à l’exception d’un usage personnel, sauf accord de l’Ofpra en vertu de l’article L. 335-3 du code de la propriété intellectuelle. Chronologie : Maiduguri et Gamboru Ngala - 2011 à 2015 Table des matières 1. Maiduguri .................................................................................................................... -

Ngala Idp Camp
QUICK ASSESSMENT: NGALA IDP CAMP SIF / NIGERIA Date of the mission: 13th December, 2016. Location: Ngala IDP Camp (Ngala LGA, Borno State, North-East Nigeria) Coordinates a. Military HQ (3rd battalion): 12°21'28.68"N 14°10'49.60"E A: 291m b. Helipad: 12°21'24.70"N 14°10'42.40"E A: 292m c. IDP camp: 12°21'34.87"N 14°10'19.57"E A: 288m Ngala IDP Camp Quick Assessment Page 1/9 Security and logistics (source: SIF and UN Joint Security Assessment) Ngala has been liberated by NAF on March 2016. Fighting against insurgents has been ongoing until summer 2016. The road and the border are now open and UNHAS helicopters are currently serving Ngala since December 2016. LGA level: On June, a clearance operation has been conducted by 3rd Battalion from Ngala towards North of the LGA, along the Cameroonian border to push away insurgents groups present in this zone of Ngala LGA. This LGA is part of the Area of Operations of Islamic State West Africa Province (ISWAP). This group remains active in the North of Ngala – due to the presence of bases in Lake Chad area – and in Kala Balge LGA where it has a freedom of movement in the southern part of the LGA. ISWAP groups are very mobile and base their actions on guerrilla warfare (ambushes, IED’s, hit- and-run tactic). Skirmishes with NAF can occur during the patrols. The actual NAF deployment is centered on: The control of the road Dikwa – Ngala to keep it open for commercial convoys, The control of the LGA’s Headquarters, The capability to conduct combat patrols from bases in order to conduct a zone control deeply inside the LGA’s. -

Outcomes in Areas of Northeast Remain Heavily Dependent on Humanitarian Assistance
NIGERIA Food Security Outlook February to September 2018 Outcomes in areas of northeast remain heavily dependent on humanitarian assistance KEY MESSAGES Current food security outcomes, February 2018 • Boko Haram conflict has left approximately 1.8 million people displaced in northeastern Nigeria and has severely limited livelihoods options for many more. Although the area under military control has expanded in recent months, the number of conflict events has remained high, with 2017 registering the most fatal conflict events in Borno State since the beginning of the insurgency. The ongoing conflict is expected to severely limit area cultivated during the primary 2018 agricultural season. • Humanitarian agencies have provided sustained food assistance in the northeast and provided significant input support for 2018 dry season agricultural activities. Since March 2017, food assistance has reached 1.9 million people or more per month, including 2.3 million people reached in January Source: FEWS NET 2018. However, surveys of displaced populations receiving FEWS NET classification is IPC-compatible. IPC-compatible analysis follows assistance have indicated that food remains a primary need, key IPC protocols but does not necessarily reflect the consensus of national food security partners. highlighting the very limited livelihoods options and high dependence on humanitarian assistance. • In most of Borno State and parts of Adamawa and Yobe States, Crisis (IPC Phase 3) outcomes are ongoing. Areas surrounding the Sambisa Forest, as well as eastern Borno State and the area along Lake Chad, are likely to deteriorate to Emergency (IPC Phase 4) during the upcoming lean season, in the absence of further assistance. Significant areas within these regions remain inaccessible to humanitarian actors, and it is likely that outcomes are similar or worse than in adjoining accessible areas. -

Submission by Human Rights Watch to the Committee on the Elimination of Discrimination Against Women November 2016
Submission by Human Rights Watch to the Committee on the Elimination of Discrimination Against Women November 2016 We write in advance of your upcoming pre-sessional review of the Nigeria government’s compliance with the Convention on the Elimination of Discrimination Against Women. This submission relates to Articles 1, 2, 3, 6, 10, 11, 12, and 14 of the Convention on the Elimination of Discrimination Against Women. It proposes issues and questions that Committee members may wish to raise with the government while reviewing its compliance with these articles. Evidence included in this submission is based in part on Human Rights Watch’s research into Boko Haram violence against women and girls in northeast Nigeria. This research is based on interviews with more than 46 witnesses and victims of Boko Haram abductions in Borno, Yobe, and Adamawa states, including with girls who escaped the April 2014 abduction of 276 girls from Chibok secondary school, as well as social workers, members of Nigerian and international nongovernmental organizations, diplomats, journalists, religious leaders, and state and federal government officials.1 This submission is also based on research conducted into the use of schools for military purposes and attacks on students, teachers, education workers, and schools in northeast Nigeria. This research included interviews with 215 people–including 99 teachers, 31 students, 36 parents, and 25 school administrators in Borno, Yobe, and Kano states between 2009 and February 2016.2 This submission is also based on Human -

“Global Terrorism Index: 2015.” Institute for Economics and Peace
MEASURING AND UNDERSTANDING THE IMPACT OF TERRORISM Quantifying Peace and its Benefits The Institute for Economics and Peace (IEP) is an independent, non-partisan, non-profit think tank dedicated to shifting the world’s focus to peace as a positive, achievable, and tangible measure of human well-being and progress. IEP achieves its goals by developing new conceptual frameworks to define peacefulness; providing metrics for measuring peace; and uncovering the relationships between business, peace and prosperity as well as promoting a better understanding of the cultural, economic and political factors that create peace. IEP has offices in Sydney, New York and Mexico City. It works with a wide range of partners internationally and collaborates with intergovernmental organizations on measuring and communicating the economic value of peace. For more information visit www.economicsandpeace.org SPECIAL THANKS to the National Consortium for the Study of Terrorism and Responses to Terrorism (START) headquartered at the University of Maryland for their cooperation on this study and for providing the Institute for Economics and Peace with their Global Terrorism Database (GTD) datasets on terrorism. CONTENTS EXECUTIVE SUMMARY 2 ABOUT THE GLOBAL TERRORISM INDEX 6 1 RESULTS 9 Global Terrorism Index map 10 Terrorist incidents map 12 Ten countries most impacted by terrorism 20 Terrorism compared to other forms of violence 30 2 TRENDS 33 Changes in the patterns and characteristics of terrorist activity 34 Terrorist group trends 38 Foreign fighters in Iraq -

IOM Nigeria DTM Emergency Tracking Tool (ETT) Report No.74 (3
DISPLACEMENT TRACKING MATRIX - Nigeria DTM EMERGENCY TRACKING TOOL (ETT) Nigeria DTM Emergency Tracking Tool (ETT) is deployed to track and provide up-to-date information on sudden displacement and other population movements ETT Report: No. 74 3 – 9 July 2018 Within the period of 3 – 9 July 2018, a Movements Abadam total of 4,716 movements were recorded, Niger Chad Arrivals: including 3,749 arrivals, 874 departures Mobbar Lake Chad 3,749 individuals 49 and 93 transit movements at loca�ons in 152 Kukawa Departures: Askira/Uba, Bama, Biu, Chibok, Damboa, Guzamala 39 874 individuals Demsa, Dikwa, Fufore, Girei, Gombi, 70 Gubio 13 Guzamala, Gwoza, Hawul, Hong, Jere, Nganzai 107 Kaga, Kala/Balge, Konduga, Kukawa, Madagali, Mafa, Magumeri, 139 Magumeri Monguno Maiduguri, Maiha, Michika, Mobbar, Monguno, Mubi-North, Marte Ngala 240 15 Mubi-South, Ngala, Nganzai, Numan, Yola-North and Yola-South Local 191 Mafa Kala/Balge Jere Dikwa Government Areas (LGAs) of Adamawa and Borno States. 29 125 311 184 Assessments iden�fied the following main triggers of movements: poor Maiduguri18 Kaga living condi�ons (37%), voluntary reloca�on (22%), improved security Konduga Bama 2 63 (14%), military opera�ons (11%), ongoing conflict (10%), fear of a�acks 729 9 (4%), and IDPs scou�ng for farmlands/farming ac�vi�es (2%). Borno Gwoza 2 Damboa 686 Number of individuals by movement triggers 7 Chibok 9 5 15 Poor Living Condi�ons 1,756 Biu Madagali 43 93 170 Askira/Uba Michika Voluntary Reloca�on 1,026 138 Kwaya Kusar 122 21 Bayo Hawul Hong 19 Mubi North Improved Security -
H. Res. 617 in the House of Representatives, U
H. Res. 617 In the House of Representatives, U. S., June 12, 2014. Whereas, on the night of April 14, 2014, 276 female stu- dents, most of them between 15 and 18 years old, were abducted by Boko Haram from the Government Girls Secondary School, a boarding school located in the north- eastern province of Borno in the Federal Republic of Ni- geria; Whereas, all public secondary schools in Borno state were closed in March 2014 because of increasing attacks in the past year that have killed hundreds of students, but the young women at the Government Girls Secondary School were recalled to take their final exams; Whereas, Boko Haram burned down several buildings before opening fire on soldiers and police who were guarding the Government Girls Secondary School and forcing the stu- dents into trucks; Whereas, according to local officials in Borno state, 53 stu- dents were able to flee their captors, and the rest remain abducted; Whereas, there are reports that the abducted girls have been sold as brides to Islamist militants for the equivalent of $12 each; 2 Whereas, the group popularly known as ‘‘Boko Haram’’, which loosely translates from the Hausa language to ‘‘Western education is sin’’, is known to oppose the edu- cation of girls; Whereas, on April 14, 2014, hours before the kidnapping in Borno state, and on May 2, 2014, Boko Haram bombed bus stations in Abuja, Nigeria, killing at least 94 people and wounding over 160, making it the deadliest set of at- tacks ever in Nigeria’s capital; Whereas, Boko Haram has kidnapped girls in the past -

The Weekly Briefing | 1 September 2014 Political and Security Risk Updates
The weekly briefing | 1 September 2014 Political and security risk updates Africa: Escalation in conflict highlights rising cross-border threat from Nigerian militants. Americas: Marina Silva’s ‘third way’ gains momentum ahead of Brazil’s presidential election. Asia and Pacific: Calls for Pakistani prime minister to resign as violent clashes continue and army consolidates its position. Europe: West warns Russia of heightened economic sanctions following incursion of Russian armed forces into eastern Ukraine. Middle East: Al-Nusra Front holds Fijian peacekeepers hostage in Syrian side of Golan Heights. Polar regions: Canadian foreign minister visits Norway and Denmark to promote Arctic cooperation. Africa Escalation in conflict highlights rising cross-border threat from Nigerian militants In recent weeks, the Nigerian Islamist militant group Boko Haram augmented its offensive from northeast Nigeria into the far north of Cameroon, forcing the Cameroonian government to further increase its deployment of soldiers to the area. On 25 August, militants carried out a house-to-house raid of the twin towns of Gamboru and Ngala, seizing control of the military base and police station and ultimately the whole town. The offensive forced thousands of residents and Nigerian military personnel to flee across the border into Cameroon. The militants then set up operations and occupied dwellings abandoned by the towns’ inhabitants. On 25-26 August, as Boko Haram advanced into the north of Cameroon near Fotokol in pursuit of the fleeing residents and Nigerian military personnel, Cameroonian security forces engaged the militants, killing 27. On 27 August, Boko Haram suffered heavy casualties as Cameroon’s military increased its operational capacity, deploying tanks to Fotokol and shelling the militants’ camp in Gamboru-Ngala from across the border. -

II. Resources
PERSPECTIVES ON TERRORISM Volume 8, Issue 6 II. Resources Boko Haram Attacks in Nigeria and Neighbouring Countries: A Chronology of Attacks by Ioannis Mantzikos Introduction [1] Boko Haram’s insurgency which pitted neighbour against neighbour, cost more than 4,000 lives, displaced close to half a million people, destroyed hundreds of schools and government buildings and devastated an already ravaged economy in the north-east of Nigeria, one of the country’s poorest regions.Within less than five years (2010 – 2014) the Nigerian Islamist terrorists organization Boko Haram (BH) has evolved into the most lethal of all salafist jihadist organisations. Originally directing its attacks mainly at security forces and government officials, BH’s campaign has expanded to include attacks on Christians, critical Muslim clerics, traditional leaders, suspected collaborators, UN offices, bars and girl schools. Its campaign of terrorism, ranges from targeting students at state (secular) schools to health workers involved in polio vaccination campaigns. In the first half of 2014 BH even surpassed the Islamic State in Iraq in terms of lethality, according to statistics compiled by the Intel Center.[2] On Tuesday, April 15, 2014, Boko Haram attacked a girls’ school in Chibok, Borno state, in northern Nigeria, abducting between 250-300 young girls. Boko Haram’s leader, Abubakar Shekau, released a video on May 5, threatening to sell the girls as “wives” while also expressing his ideological opposition to the idea of educating girls. The abduction of girls and subsequent developments have prompted several nations to send logistical support teamswhile the Nigerian government offered a $300,000 reward for information leading to the girls’ rescue. -

Latest Picture Small Map Or Picture
2017 Monthly Factsheet Reporting period: January to February 2017 *Data in this document does not include Partners Outside the HRP 2017. Latest Picture Small Map or Picture Mohammed Kyarimi camp, Dikwa Emergency shelters at 20 houses unit camp in Dikwa Overview:________________________________________________ Key figures (HRP 2017) There is continuous influx of IDPs to existing camps and to Local Government Areas accessible towns such as Mafa, Bama, Maiduguri MC, Population in need: 2,300,000 Konduga, Ngala, Gamboru Ngala, Banki, Chibok and Damboa. Sudden DMS Sector target population: 800,000 movements of populations are linked to better access, allowing people to Shelter Sector target population: 1,040,000 flee locations previously under Boko Haram control or due to attacks. After several years of displacement, IDPs in existing camps require support to maintain their shelters and for NFI. Urgent drainage work is needed in Shelter: several camps ahead of the rainy season, in order to mitigate the risks of Funding needs: $ 70.6M flooding, in particular in the LGAs of Borno where the shelter interventions are now being up-scaled. % of funds received: 4.5% Limited funding received in 2016 is being stretched to 2017 due to the low DMS/CCCM amount of resources allocated in this year. The lack of contingency stocks prepositioned in various LGAs has critically hampered the immediate Funding needs: $ 11.6M response in Mafa, Bama, Chibok, Pulka and other locations, indicating an % of funds received: 0% urgent need for the prepositioning of NFI stocks across the country. Logistic concerns remain in several areas, lack of land to resettle IDPs in planned camps and increased concerns regarding land situation ahead of the rainy season. -

AFRICA Boko Haram Still Able to Inflict Damage in Nigeria
AFRICA Boko Haram Still Able to Inflict Damage in Nigeria OE Watch Commentary: The Boko Haram insurgency in northeastern Nigeria has entered its tenth year, and the Nigerian army has had mixed results in fighting the group. Boko Haram is still able to inflict significant damage, especially on civilians, even as the military is winning battles elsewhere in northeastern Nigeria, as evidenced by the two accompanying excerpts from local sources. The first excerpted article in Punch, a popular Nigerian publication, discusses military attitudes after the military conducted several clearing operations in villages in northeastern Nigeria’s Borno State and some Boko Haram commanders surrendered to the military. The Nigerian soldiers recovered weapons from Boko Haram fighters and uncovered their hideouts. After the operations concluded, a Nigerian general stated that the army was moving toward final victory over the insurgents and more insurgent enclaves and hideouts would be struck with artillery. Despite this, the article also pointed out that the military found the insurgents had sophisticated battle trenches to ward off army offensives. Nigerian Army Boko Haram demonstration. Source: VOA/Nicolas Pinault via Wikimedia, https://commons.wikimedia.org/wiki/File:Nigerian_Army_Boko_Haram_demonstration.jpg CC by SA 2.0 On the other hand, just over one week after the article was published, Boko Haram carried out one of the largest massacres in years in Gubio, Borno State. According to another widely read Nigerian publication, Vanguard, more than 80 villagers were killed while others were injured and taken captive by Boko Haram’s Islamic State in Iraq and Syria (ISIS)-loyal faction. Cattle and other livestock were also stolen. -
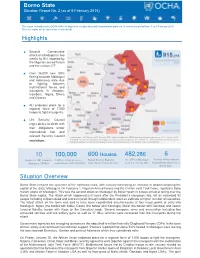
Borno State Situation Report No
Borno State Situation Report No. 2 (as of 6 February 2015) Situation Report No. 2 (as of 23 January 2015) Nigeria: This report is produced by OCHA Office in Nigeria in collaboration with humanitarian partners. It covers the period from 1 to 6 February 2015. The next report will be issued as events unfold. Highlights • Second Consecutive attack on Maiduguri in two weeks by BH, repelled by the Nigerian armed forces and the civilian JTF. • Over 36,000 new IDPs fleeing towards Maiduguri and Adamawa state due to fighting between multinational forces and insurgents in Abadam, Gamboru, Ngala, Dikwa and Gworza AU endorses plans for a • regional force of 7,500 troops to fight insurgents. • UN Security Council urges states, to abide with their obligations under international law and relevant Security Council Creation date: 05 February 2015 Sources: IDPs figures provided by NEMA and humanitarian partners as of 31 January 2015; . Feedback: Choice Ufuoma Okoro: [email protected] www.unocha.org/nigeria www.reliefweb.int. The boundaries and names shown resolutions and the designations used on this map do not imply official endorsement or acceptance by the United Nations. Houses 482 , 286 6 10 100,000 600 Number of IDP Camps in Children at risk of severe Razed down in Baga by est. IDPs in Maiduguri Number of International as at Jan. 15 (NEMA) Humanitarian Agencies in Maiduguri (NEMA) malnutrition in NE (UNICEF) Boko Haram (Amnesty Intl.) Borno State Situation Overview Borno State remains the epicenter of the northeast crisis, with January witnessing an increase in attacks targeting the capital of the state; Maiduguri.