Familial Multiple Coagulation Factor Deficiencies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Familial Multiple Coagulation Factor Deficiencies
Journal of Clinical Medicine Article Familial Multiple Coagulation Factor Deficiencies (FMCFDs) in a Large Cohort of Patients—A Single-Center Experience in Genetic Diagnosis Barbara Preisler 1,†, Behnaz Pezeshkpoor 1,† , Atanas Banchev 2 , Ronald Fischer 3, Barbara Zieger 4, Ute Scholz 5, Heiko Rühl 1, Bettina Kemkes-Matthes 6, Ursula Schmitt 7, Antje Redlich 8 , Sule Unal 9 , Hans-Jürgen Laws 10, Martin Olivieri 11 , Johannes Oldenburg 1 and Anna Pavlova 1,* 1 Institute of Experimental Hematology and Transfusion Medicine, University Clinic Bonn, 53127 Bonn, Germany; [email protected] (B.P.); [email protected] (B.P.); [email protected] (H.R.); [email protected] (J.O.) 2 Department of Paediatric Haematology and Oncology, University Hospital “Tzaritza Giovanna—ISUL”, 1527 Sofia, Bulgaria; [email protected] 3 Hemophilia Care Center, SRH Kurpfalzkrankenhaus Heidelberg, 69123 Heidelberg, Germany; ronald.fi[email protected] 4 Department of Pediatrics and Adolescent Medicine, University Medical Center–University of Freiburg, 79106 Freiburg, Germany; [email protected] 5 Center of Hemostasis, MVZ Labor Leipzig, 04289 Leipzig, Germany; [email protected] 6 Hemostasis Center, Justus Liebig University Giessen, 35392 Giessen, Germany; [email protected] 7 Center of Hemostasis Berlin, 10789 Berlin-Schöneberg, Germany; [email protected] 8 Pediatric Oncology Department, Otto von Guericke University Children’s Hospital Magdeburg, 39120 Magdeburg, Germany; [email protected] 9 Division of Pediatric Hematology Ankara, Hacettepe University, 06100 Ankara, Turkey; Citation: Preisler, B.; Pezeshkpoor, [email protected] B.; Banchev, A.; Fischer, R.; Zieger, B.; 10 Department of Pediatric Oncology, Hematology and Clinical Immunology, University of Duesseldorf, Scholz, U.; Rühl, H.; Kemkes-Matthes, 40225 Duesseldorf, Germany; [email protected] B.; Schmitt, U.; Redlich, A.; et al. -

Alterations of Genetic Variants and Transcriptomic Features of Response to Tamoxifen in the Breast Cancer Cell Line
Alterations of Genetic Variants and Transcriptomic Features of Response to Tamoxifen in the Breast Cancer Cell Line Mahnaz Nezamivand-Chegini Shiraz University Hamed Kharrati-Koopaee Shiraz University https://orcid.org/0000-0003-2345-6919 seyed taghi Heydari ( [email protected] ) Shiraz University of Medical Sciences https://orcid.org/0000-0001-7711-1137 Hasan Giahi Shiraz University Ali Dehshahri Shiraz University of Medical Sciences Mehdi Dianatpour Shiraz University of Medical Sciences Kamran Bagheri Lankarani Shiraz University of Medical Sciences Research Keywords: Tamoxifen, breast cancer, genetic variants, RNA-seq. Posted Date: August 17th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-783422/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/33 Abstract Background Breast cancer is one of the most important causes of mortality in the world, and Tamoxifen therapy is known as a medication strategy for estrogen receptor-positive breast cancer. In current study, two hypotheses of Tamoxifen consumption in breast cancer cell line (MCF7) were investigated. First, the effect of Tamoxifen on genes expression prole at transcriptome level was evaluated between the control and treated samples. Second, due to the fact that Tamoxifen is known as a mutagenic factor, there may be an association between the alterations of genetic variants and Tamoxifen treatment, which can impact on the drug response. Methods In current study, the whole-transcriptome (RNA-seq) dataset of four investigations (19 samples) were derived from European Bioinformatics Institute (EBI). At transcriptome level, the effect of Tamoxifen was investigated on gene expression prole between control and treatment samples. -

Mechanisms of Synaptic Plasticity Mediated by Clathrin Adaptor-Protein Complexes 1 and 2 in Mice
Mechanisms of synaptic plasticity mediated by Clathrin Adaptor-protein complexes 1 and 2 in mice Dissertation for the award of the degree “Doctor rerum naturalium” at the Georg-August-University Göttingen within the doctoral program “Molecular Biology of Cells” of the Georg-August University School of Science (GAUSS) Submitted by Ratnakar Mishra Born in Birpur, Bihar, India Göttingen, Germany 2019 1 Members of the Thesis Committee Prof. Dr. Peter Schu Institute for Cellular Biochemistry, (Supervisor and first referee) University Medical Center Göttingen, Germany Dr. Hans Dieter Schmitt Neurobiology, Max Planck Institute (Second referee) for Biophysical Chemistry, Göttingen, Germany Prof. Dr. med. Thomas A. Bayer Division of Molecular Psychiatry, University Medical Center, Göttingen, Germany Additional Members of the Examination Board Prof. Dr. Silvio O. Rizzoli Department of Neuro-and Sensory Physiology, University Medical Center Göttingen, Germany Dr. Roland Dosch Institute of Developmental Biochemistry, University Medical Center Göttingen, Germany Prof. Dr. med. Martin Oppermann Institute of Cellular and Molecular Immunology, University Medical Center, Göttingen, Germany Date of oral examination: 14th may 2019 2 Table of Contents List of abbreviations ................................................................................. 5 Abstract ................................................................................................... 7 Chapter 1: Introduction ............................................................................ -

Analysis of Newly Detected Mutations in the MCFD2 Gene Giving Rise to Combined Deficiency of Coagulation Factors V and VIII
Haemophilia (2011), 1–5 DOI: 10.1111/j.1365-2516.2011.02529.x ORIGINAL ARTICLE Analysis of newly detected mutations in the MCFD2 gene giving rise to combined deficiency of coagulation factors V and VIII H. ELMAHMOUDI,*1 E. WIGREN, 1 A. LAATIRI,à A. JLIZI,* A. ELGAAIED,* E. GOUIDER§ and Y. LINDQVISTà *Laboratory of Genetics, Immunology and Human Pathologies, Tunis, Tunisia; Department of Medical Biochemistry and Biophysics, Karolinska Institutet, Stockholm, Sweden; àDepartment of Hematology, Fattouma Bourguiba Hospital, Monastir, Tunisia; and §Hemophilia Treatment Center, Aziza Othmana Hospital, Tunis, Tunisia Summary. Combined deficiency of coagulation factor V uncharged asparagine. To elucidate the structural effect (FV) and factor VIII (FVIII) (F5F8D) is a rare autosomal of this mutation, we performed circular dichroism (CD) recessive disorder characterized by mild-to-moderate analysis of secondary structure and stability. In addi- bleeding and reduction in FV and FVIII levels in plasma. tion, CD analysis was performed on two missense F5F8D is caused by mutations in one of two different mutations found in previously reported F5F8D patients. genes, LMAN1 and MCFD2, which encode proteins Our results show that all analysed mutant variants that form a complex involved in the transport of FV and give rise to destabilized proteins and highlight the FVIII from the endoplasmic reticulum to the Golgi importance of a structurally intact and functional apparatus. Here, we report the identification of a novel MCFD2 for the efficient secretion of coagulation factors mutation Asp89Asn in the MCFD2 gene in a Tunisian V and VIII. patient. In the encoded protein, this mutation causes substitution of a negatively charged aspartate, involved Keywords: circular dichroism, combined FV and FVIII in several structurally important interactions, to an deficiency, LMAN1, MCFD2, mutations excessive bleeding during or after trauma, surgery, or Introduction labour. -

COPI Activity Coupled with Fatty Acid Biosynthesis Is Required for Viral Replication
COPI Activity Coupled with Fatty Acid Biosynthesis Is Required for Viral Replication Sara Cherry1*, Amit Kunte2, Hui Wang3, Carolyn Coyne4, Robert B. Rawson2, Norbert Perrimon3 1 University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania, United States of America, 2 University of Texas Southwestern Medical Center, Dallas, Texas, United States of America, 3 Harvard Medical School, Howard Hughes Medical Institute, Boston, Massachusetts, United States of America, 4 Children’s Hospital of Pennsylvania, Philadelphia, Pennsylvania, United States of America During infection by diverse viral families, RNA replication occurs on the surface of virally induced cytoplasmic membranes of cellular origin. How this process is regulated, and which cellular factors are required, has been unclear. Moreover, the host–pathogen interactions that facilitate the formation of this new compartment might represent critical determinants of viral pathogenesis, and their elucidation may lead to novel insights into the coordination of vesicular trafficking events during infection. Here we show that in Drosophila cells, Drosophila C virus remodels the Golgi apparatus and forms a novel vesicular compartment, on the surface of which viral RNA replication takes place. Using genome-wide RNA interference screening, we found that this step in the viral lifecycle requires at least two host encoded pathways: the coat protein complex I (COPI) coatamer and fatty acid biosynthesis. Our results integrate, clarify, and extend numerous observations concerning the cell biology of viral replication, allowing us to conclude that the coupling of new cellular membrane formation with the budding of these vesicles from the Golgi apparatus allows for the regulated generation of this new virogenic organelle, which is essential for viral replication. -

Combined Factor V and Factor VIII Deficiency in a Thai Patient
Haemophilia (2005), 11, 280–284 DOI: 10.1111/j.1365-2516.2005.01092.x CASE REPORT Combined factor V and factor VIII deficiency in a Thai patient: a case report of genotype and phenotype characteristics N. SIRACHAINAN,* B. ZHANG, A. CHUANSUMRIT,* S. PIPE,à W. SASANAKUL§ and D. GINSBURG *Department of Pediatrics, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; Department of Human Genetics; àDepartment of Pediatrics, University of Michigan, Ann Arbor, MI, USA; and §Research Center, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Summary. A Thai woman, with no family history of VIII concentrate, fresh frozen plasma and antifibrin- bleeding disorders, presented with excessive bleeding olytic agent.Gene analysis of the proband identified after minor trauma and tooth extraction. The two LMAN1 gene mutations; one of which is 823-1 screening coagulogram revealed prolonged activated G fi C, a novel splice acceptor site mutation that is partial thromboplastin time and prothrombin time. inherited from her father, the other is 1366 C fi T, The specific-factor assay confirmed the diagnosis a nonsense mutation that is inherited from her of combined factor V and factor VIII deficiency mother. Thus, the compound heterozygote of these (F5F8D). Her plasma levels of factor V and factor two mutations in LMAN1 cause combined F5F8D. VIII were 10% and 12.5% respectively. The medi- cations and blood product treatment to prevent Keywords: bleeding, combined factor V and factor bleeding from invasive procedure included 1-deami- VIII deficiency, ER-Golgi intermediate compartment no-8-d-arginine vasopressin, cryoprecipitate, factor protein, LMAN1 and 30% and the successful treatments in order to Introduction prevent bleeding from surgery include administration Combined factor V and factor VIII deficiency of 1-deamino-8-d-arginine vasopressin (DDAVP) and (F5F8D) is a rare autosomal recessive bleeding plasma transfusion [7,8]. -

Sec13 Safeguards the Integrity of the Endoplasmic Reticulum and Organogenesis of the Digestive System in Zebrafish
Developmental Biology 367 (2012) 197–207 Contents lists available at SciVerse ScienceDirect Developmental Biology journal homepage: www.elsevier.com/locate/developmentalbiology Sec13 safeguards the integrity of the endoplasmic reticulum and organogenesis of the digestive system in zebrafish Xubo Niu a,1, Chuan Gao b,1, Li Jan Lo a, Yue Luo a, Chunmei Meng c, Jian Hong c, Wanjin Hong d,e, Jinrong Peng a,n a Key Laboratory for Molecular Animal Nutrition, Ministry of Education, College of Animal Sciences, Zhejiang University, Hangzhou, PR China b Department of Biological Sciences, National University of Singapore, Singapore c Institute of Biotechnology, Zhejiang University, Hangzhou, PR China d School of Pharmaceutical Sciences, Xiamen University, Xiamen, PR China e Institute of Molecular and Cell Biology, Agency for Science and Technology Research (A*STAR), Singapore article info abstract Article history: The Sec13-Sec31 heterotetramer serves as the outer coat in the COPII complex, which mediates protein Received 25 October 2011 trafficking from the endoplasmic reticulum (ER) to the Golgi apparatus. Although it has been studied in Received in revised form depth in yeast and cultured cells, the role of COPII in organogenesis in a multicellular organism has not. 12 April 2012 We report here that a zebrafish sec13sq198 mutant, which exhibits a phenotype of hypoplastic digestive Accepted 4 May 2012 organs, has a mutation in the sec13 gene. The mutant gene encodes a carboxyl-terminus-truncated Available online 15 May 2012 Sec13 that loses its affinity to Sec31a, which leads to disintegration of the ER structure in various Keywords: differentiated cells in sec13sq198, including chondrocytes, intestinal epithelial cells and hepatocytes. -

SEC13 Antibody (Center) Affinity Purified Rabbit Polyclonal Antibody (Pab) Catalog # Ap10738c
苏州工业园区双圩路9号1幢 邮 编 : 215000 电 话 : 0512-88856768 SEC13 Antibody (Center) Affinity Purified Rabbit Polyclonal Antibody (Pab) Catalog # AP10738c Specification SEC13 Antibody (Center) - Product info Application WB, FC Primary Accession P55735 Other Accession NP_899195.1 Reactivity Human Host Rabbit Clonality Polyclonal Isotype Rabbit Ig Clone Names RB23825 Calculated MW 35541 SEC13 Antibody (Center) - Additional info Gene ID 6396 Other Names SEC13 Antibody (Center) (Cat. Protein SEC13 homolog, SEC13-like protein 1, SEC13-related #AP10738c) western blot analysis in protein, SEC13, D3S1231E, SEC13L1, SEC13R HepG2 cell line lysates (35ug/lane).This demonstrates the SEC13 antibody Target/Specificity detected the SEC13 protein (arrow). This SEC13 antibody is generated from rabbits immunized with a KLH conjugated synthetic peptide between 72-100 amino acids from the Central region of human SEC13. Dilution WB~~1:1000 FC~~1:10~50 Format Purified polyclonal antibody supplied in PBS with 0.09% (W/V) sodium azide. This antibody is purified through a protein A column, followed by peptide affinity purification. Storage Maintain refrigerated at 2-8°C for up to 2 weeks. For long term storage store at -20°C in small aliquots to prevent freeze-thaw cycles. SEC13 Antibody (Center) (Cat. #AP10738c) flow cytometric analysis of Precautions HepG2 cells (right histogram) compared SEC13 Antibody (Center) is for research use only and not for to a negative control cell (left use in diagnostic or therapeutic procedures. histogram).FITC-conjugated goat-anti-rabbit secondary antibodies were used for the analysis. SEC13 Antibody (Center) - Protein Information Name SEC13 Function Functions as a component of the nuclear pore complex (NPC) and the COPII coat. -
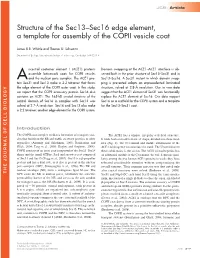
Structure of the Sec13–Sec16 Edge Element, a Template for Assembly of the COPII Vesicle Coat
JCB: Article Structure of the Sec13–Sec16 edge element, a template for assembly of the COPII vesicle coat James R.R. Whittle and Thomas U. Schwartz Department of Biology, Massachusetts Institute of Technology, Cambridge, MA 02139 ncestral coatomer element 1 (ACE1) proteins Domain swapping at the ACE1–ACE1 interface is ob- assemble latticework coats for COPII vesicles served both in the prior structure of Sec13–Sec31 and in A and the nuclear pore complex. The ACE1 pro- Sec13–Sec16. A Sec31 mutant in which domain swap- tein Sec31 and Sec13 make a 2:2 tetramer that forms ping is prevented adopts an unprecedented laminated the edge element of the COPII outer coat. In this study, structure, solved at 2.8-Å resolution. Our in vivo data we report that the COPII accessory protein Sec16 also suggest that the ACE1 element of Sec31 can functionally contains an ACE1. The 165-kD crystal structure of the replace the ACE1 element of Sec16. Our data support central domain of Sec16 in complex with Sec13 was Sec16 as a scaffold for the COPII system and a template solved at 2.7-Å resolution. Sec16 and Sec13 also make for the Sec13–Sec31 coat. a 2:2 tetramer, another edge element for the COPII system. Introduction The COPII coat complex mediates formation of transport vesi- The ACE1 has a unique, irregular -helical structure. cles that bud from the ER and traffic secretory proteins to other It folds back on itself to form a J shape, divided into three mod- organelles (Antonny and Schekman, 2001; Bonifacino and ules (Fig. -

ER-To-Golgi Trafficking and Its Implication in Neurological Diseases
cells Review ER-to-Golgi Trafficking and Its Implication in Neurological Diseases 1,2, 1,2 1,2, Bo Wang y, Katherine R. Stanford and Mondira Kundu * 1 Department of Pathology, St. Jude Children’s Research Hospital, Memphis, TN 38105, USA; [email protected] (B.W.); [email protected] (K.R.S.) 2 Department of Cell and Molecular Biology, St. Jude Children’s Research Hospital, Memphis, TN 38105, USA * Correspondence: [email protected]; Tel.: +1-901-595-6048 Present address: School of Life Sciences, Xiamen University, Xiamen 361102, China. y Received: 21 November 2019; Accepted: 7 February 2020; Published: 11 February 2020 Abstract: Membrane and secretory proteins are essential for almost every aspect of cellular function. These proteins are incorporated into ER-derived carriers and transported to the Golgi before being sorted for delivery to their final destination. Although ER-to-Golgi trafficking is highly conserved among eukaryotes, several layers of complexity have been added to meet the increased demands of complex cell types in metazoans. The specialized morphology of neurons and the necessity for precise spatiotemporal control over membrane and secretory protein localization and function make them particularly vulnerable to defects in trafficking. This review summarizes the general mechanisms involved in ER-to-Golgi trafficking and highlights mutations in genes affecting this process, which are associated with neurological diseases in humans. Keywords: COPII trafficking; endoplasmic reticulum; Golgi apparatus; neurological disease 1. Overview Approximately one-third of all proteins encoded by the mammalian genome are exported from the endoplasmic reticulum (ER) and transported to the Golgi apparatus, where they are sorted for delivery to their final destination in membrane compartments or secretory vesicles [1]. -

Whole Genome Sequencing of Familial Non-Medullary Thyroid Cancer Identifies Germline Alterations in MAPK/ERK and PI3K/AKT Signaling Pathways
biomolecules Article Whole Genome Sequencing of Familial Non-Medullary Thyroid Cancer Identifies Germline Alterations in MAPK/ERK and PI3K/AKT Signaling Pathways Aayushi Srivastava 1,2,3,4 , Abhishek Kumar 1,5,6 , Sara Giangiobbe 1, Elena Bonora 7, Kari Hemminki 1, Asta Försti 1,2,3 and Obul Reddy Bandapalli 1,2,3,* 1 Division of Molecular Genetic Epidemiology, German Cancer Research Center (DKFZ), D-69120 Heidelberg, Germany; [email protected] (A.S.); [email protected] (A.K.); [email protected] (S.G.); [email protected] (K.H.); [email protected] (A.F.) 2 Hopp Children’s Cancer Center (KiTZ), D-69120 Heidelberg, Germany 3 Division of Pediatric Neurooncology, German Cancer Research Center (DKFZ), German Cancer Consortium (DKTK), D-69120 Heidelberg, Germany 4 Medical Faculty, Heidelberg University, D-69120 Heidelberg, Germany 5 Institute of Bioinformatics, International Technology Park, Bangalore 560066, India 6 Manipal Academy of Higher Education (MAHE), Manipal, Karnataka 576104, India 7 S.Orsola-Malphigi Hospital, Unit of Medical Genetics, 40138 Bologna, Italy; [email protected] * Correspondence: [email protected]; Tel.: +49-6221-42-1709 Received: 29 August 2019; Accepted: 10 October 2019; Published: 13 October 2019 Abstract: Evidence of familial inheritance in non-medullary thyroid cancer (NMTC) has accumulated over the last few decades. However, known variants account for a very small percentage of the genetic burden. Here, we focused on the identification of common pathways and networks enriched in NMTC families to better understand its pathogenesis with the final aim of identifying one novel high/moderate-penetrance germline predisposition variant segregating with the disease in each studied family. -

MCFD2 Antibody
Catalog: OM213417 Scan to get more validated information MCFD2 Antibody Catalog: OM213417 100ug Product profile Product name MCFD2 Antibody Antibody Type Primary Antibodies Key Feature Clonality Polyclonal Isotype Ig Host Species Rabbit Tested Applications WB ,IHC ,FC Species Reactivity Human Concentration 1 mg/ml Purification Target Information Gene Synonyms SDNSF Alternative Names MCFD2; SDNSF; Multiple coagulation factor deficiency protein 2; Neural stem cell-derived neuronal surviv al protein Molecular Weight(MW) 16390 Da Function The MCFD2-LMAN1 complex forms a specific cargo receptor for the ER-to-Golgi transport of selected pr oteins. Plays a role in the secretion of coagulation factors Tissue Specificity This MCFD2 antibody is generated from rabbits immunized with a recombinant protein from human MCF D2. Cellular Localization Endoplasmic reticulum-Golgi intermediate compartment. Endoplasmic reticulum. Golgi apparatus Database Links Entrez Gene 90411 Entrez Gene 90411 Application Application Western blot analysis of MCFD2 Antibody in MDA-MB231 cell line lysates (35ug/lane). MCFD2 (arrow) was detected using the purified Pab. Application Formalin-fixed and paraffin-embedded human skin reacted with MCFD2 Antibody, which was peroxidase-conjugated to the secondary antibody, followed by DAB staining. This data demonstrates the use of this antibody for immunohistochemistry; clinical relevance has not been evaluated. Application MCFD2 Antibody flow cytometric analysis of MDA-MB231 cells (right histogram) compared to a negative control cell (left histogram).FITC-conjugated goat-anti- rabbit secondary antibodies were used for the analysis. Application Notes WB~~1:100~500 IHC~~1:50~100 FC~~1:10~50: Additional Information Form Liquid Storage Instructions For short-term storage, store at 4° C.