It Is Well- from Surgical Consideration
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nail Anatomy and Physiology for the Clinician 1
Nail Anatomy and Physiology for the Clinician 1 The nails have several important uses, which are as they are produced and remain stored during easily appreciable when the nails are absent or growth. they lose their function. The most evident use of It is therefore important to know how the fi ngernails is to be an ornament of the hand, but healthy nail appears and how it is formed, in we must not underestimate other important func- order to detect signs of pathology and understand tions, such as the protective value of the nail plate their pathogenesis. against trauma to the underlying distal phalanx, its counterpressure effect to the pulp important for walking and for tactile sensation, the scratch- 1.1 Nail Anatomy ing function, and the importance of fi ngernails and Physiology for manipulation of small objects. The nails can also provide information about What we call “nail” is the nail plate, the fi nal part the person’s work, habits, and health status, as of the activity of 4 epithelia that proliferate and several well-known nail features are a clue to sys- differentiate in a specifi c manner, in order to form temic diseases. Abnormal nails due to biting or and protect a healthy nail plate [1 ]. The “nail onychotillomania give clues to the person’s emo- unit” (Fig. 1.1 ) is composed by: tional/psychiatric status. Nail samples are uti- • Nail matrix: responsible for nail plate production lized for forensic and toxicology analysis, as • Nail folds: responsible for protection of the several substances are deposited in the nail plate nail matrix Proximal nail fold Nail plate Fig. -

Medical Glossary
medical glossary AC Joint — Acromioclavicular joint; joint of the Bone Scan — An imaging procedure in which a Edema — Accumulation of fluid in organs and tis- shoulder where acromion process of the scapula radioactive-labeled substance is injected into the sues of the body (swelling). and the distal end of the clavicle meet; most shoul- body to determine the status of a bony injury. If the Effusion — Accumulation of fluid, in various der separations occur at this point. radioactive substance is taken up the bone at the spaces in the body, or the knee itself. Commonly, Abduct — Movement of any extremity away from injury site, the injury will show as a “hot spot” on the knee has an effusion after an injury. the midline of the body. This action is achieved by the scan image. The bone scan is particularly use- ful in the diagnosis of stress fractures. Electrical Galvanic Stimulation (EGS) — An elec- an abductor muscle. trical therapeutic modality that sends a current to Abrasion — Any injury which rubs off the surface Brachial Plexus — Network of nerves originating the body at select voltages and frequencies in of the skin. from the cervical vertebrae and running down to order to stimulate pain receptors, disperse edema, the shoulder, arm, hand, and fingers. Abscess — An infection which produces pus; can or neutralize muscle spasms among other function- be the result of a blister, callus, penetrating wound Bruise — A discoloration of the skin due to an al applications. or laceration. extravasation of blood into the underlying tissues. Electromyogran (EMG) — Test to determine nerve Adduct — Movement of an extremity toward the Bursa — A fluid-filled sac that is located in areas function. -

Dignity on Trial RIGHTS India’S Need for Sound Standards for Conducting and Interpreting Forensic Examinations of Rape Survivors WATCH
India HUMAN Dignity on Trial RIGHTS India’s Need for Sound Standards for Conducting and Interpreting Forensic Examinations of Rape Survivors WATCH Dignity on Trial India’s Need for Sound Standards for Conducting and Interpreting Forensic Examinations of Rape Survivors Copyright © 2010 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 1-56432-681-0 Cover design by Rafael Jimenez Human Rights Watch 350 Fifth Avenue, 34th floor New York, NY 10118-3299 USA Tel: +1 212 290 4700, Fax: +1 212 736 1300 [email protected] Poststraße 4-5 10178 Berlin, Germany Tel: +49 30 2593 06-10, Fax: +49 30 2593 0629 [email protected] Avenue des Gaulois, 7 1040 Brussels, Belgium Tel: + 32 (2) 732 2009, Fax: + 32 (2) 732 0471 [email protected] 64-66 Rue de Lausanne 1202 Geneva, Switzerland Tel: +41 22 738 0481, Fax: +41 22 738 1791 [email protected] 2-12 Pentonville Road, 2nd Floor London N1 9HF, UK Tel: +44 20 7713 1995, Fax: +44 20 7713 1800 [email protected] 27 Rue de Lisbonne 75008 Paris, France Tel: +33 (1)43 59 55 35, Fax: +33 (1) 43 59 55 22 [email protected] 1630 Connecticut Avenue, N.W., Suite 500 Washington, DC 20009 USA Tel: +1 202 612 4321, Fax: +1 202 612 4333 [email protected] Web Site Address: http://www.hrw.org September 2010 1-56432-681-0 Dignity on Trial India’s Need for Sound Standards for Conducting and Interpreting Forensic Examinations of Rape Survivors I. Summary and Recommendations ..................................................................................... 1 The Finger Test .............................................................................................................. -

A Study of Finger Length Relation (Ring Finger & Little Finger Ie 4D5D)
A Study of Finger Length Relation (Ring finger & little finger i.e. 4D5D) with Human Personality. Dr Devasis Ghosh, Dept. of Psychiatry, Dane Garth, Furness General Hospital, UK. Abstract: Several studies in the past have demonstrated a strong correlation of finger lengths ratio and human personality. This current prospective study attempts to correlate the finger length ratio of the 4th to 5th finger in males and females with the human personality traits --Psychoticism, Neuroticism & Extraversion using EPQ (Eysenck Personality Questionnaire). The hypothesis in this study is that males and females having the tip of the little fingers below the distal finger mark on the adjacent ring fingers in both their outstretched hands (arbitrarily named Group C) will have higher Neuroticism scores (i.e. they will be more anxious, worried, moody, and unstable), compared to the males and females who have the tip of the little fingers above the distal finger mark on the adjacent ring fingers in both their outstretched hands (arbitrarily named Group A). The results of this study shows that Group C females have a significantly higher Neuroticism and Psychoticism scores compared to Group A females. Similarly in case of males the results show that Group C males have a significantly higher Neuroticism and Extraversion scores compared to Group A males. So, there is a genetically predetermined physical marker i.e. whether the tips of the little fingers are above or below the distal finger mark on the adjacent ring fingers in both hands that determines the characteristic personality traits of a person. Key words: Personality; Finger lengths(4D&5D) Introduction: The disproportionate length of human fingers has generated much interest among researchers. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Cubital Tunnel Syndrome)
DISEASES & CONDITIONS Ulnar Nerve Entrapment at the Elbow (Cubital Tunnel Syndrome) Ulnar nerve entrapment occurs when the ulnar nerve in the arm becomes compressed or irritated. The ulnar nerve is one of the three main nerves in your arm. It travels from your neck down into your hand, and can be constricted in several places along the way, such as beneath the collarbone or at the wrist. The most common place for compression of the nerve is behind the inside part of the elbow. Ulnar nerve compression at the elbow is called "cubital tunnel syndrome." Numbness and tingling in the hand and fingers are common symptoms of cubital tunnel syndrome. In most cases, symptoms can be managed with conservative treatments like changes in activities and bracing. If conservative methods do not improve your symptoms, or if the nerve compression is causing muscle weakness or damage in your hand, your doctor may recommend surgery. This illustration of the bones in the shoulder, arm, and hand shows the path of the ulnar nerve. Reproduced from Mundanthanam GJ, Anderson RB, Day C: Ulnar nerve palsy. Orthopaedic Knowledge Online 2009. Accessed August 2011. Anatomy At the elbow, the ulnar nerve travels through a tunnel of tissue (the cubital tunnel) that runs under a bump of bone at the inside of your elbow. This bony bump is called the medial epicondyle. The spot where the nerve runs under the medial epicondyle is commonly referred to as the "funny bone." At the funny bone the nerve is close to your skin, and bumping it causes a shock-like feeling. -

Pedicure: Nail Enhancements
All Hair Services Include Shampoo All Services Based on Student Availability Long Hair is Extra & Senior Price Available Hair Cuts: Color: (Does Not Include Cut & Style) Hair Cut (Hood dryer) $6.50 Retouch/Tint/PM Shine $14.50 With Blowdry $13.50 Additional Application $8.00 With Blowdry & Flat Iron $21.50 Color (All over color) $20.00 Foils Each $4.00 Hair Styles: Hair Length to Collar $38.00 Shampoo/Set $6.75 Hair Length to Shoulder $48.00 Spiral Rod Set $20.00 Hair Length past Shoulder $58.00 Shampoo/ Blowdry $9.00 Frosting with Cap $17.50 With Thermal Iron $13.00 Men’s Comb Highlight with Cut $15.00 With Flat Iron $15.00 With Press & Curl $18.00 Perms & Relaxers: (Includes Cut & Style) Wrap Only $6.50 Regular or Normal Hair $20.95 Wrap with Roller Set $10.50 Resistant or Tinted Hair $26.00 Fingerwaves with Style $17.50 Spiral or Piggyback $36.00 Twists $3.00 Relaxer $35.00 Straight Back $20.00 Curled $15.00 Other Hair Services: Spiral $20.00 Shampoo Only $2.00 French Braids with Blowdry $15.00 Line-up $3.00 Under 10 Braids $20.00 Deep Condition $5.00 Over 10 Braids $25.00 Keratin Treatment $15.00 Braid Removal $15.00 Updo or French Roll $20.00 Manicure: Spa Manicure $9.50 Waxing: French Manicure $8.00 Brow $6.00 Manicure $6.42 Lip $5.00 Chin $5.00 Pedicure: Full Face $15.00 Spa Pedicure $20.00 Half Leg $15.00 French Pedicure $17.00 Full Leg $30.00 Pedicure $15.00 Underarm $15.00 Half Arm $10.00 Nail Enhancements: Full Arm $15.00 Shellac (French $2) $15.00 Mid Back & Up $15.00 Overlay (Natural Nail) $12.00 Full Back $25.00 Acrylic Full Set $16.50 Bikini $25.00 Gel Full Set $18.00 Fill-in Gel & Acrylic $12.00 Massages: Nail Repair( Per Nail) $2.00 Relaxation $15.00 Soak Off $3.00 Deep Tissue $19.95 Nail Art (Per Nail) $1.00 Other Nail Services: Nails & Waxing Services Taxable Polish Change $4.00 Nails Clipped $5.00 Paraffin Dip Wax $5.00 . -

Palm Reading
Palm Reading Also known as palmistry or chiromancy, palm reading is practiced all over the world with roots in Indian astrology and gypsy fortune-telling. The objective is to evaluate a person’s character and aspects of their life by studying the palm of their hand. There is no substantiate evidence of correlation between palm features and psychological traits; palm reading is for entertainment purposes. Getting Started Which hand to read? There are two main practices: For males, the left hand is what you’re born with, and the right is what you’ve accumulated throughout your life. For females, it’s the opposite. Your dominant hand (the hand you use most often) determines your future and your other, non-dominant hand, is used to determine the past or hidden traits Take these into consideration when choosing which hand to read. Reading the Primary Lines of your Hand 1. Interpret the Heart Line This line is believed to indicate emotional stability, romantic perspectives, depression, and cardiac health. Begins below the index finger = content with love life Begins below the middle finger = selfish when it comes to love Begins in-between the middle and index fingers = caring and understanding Is straight and short = less interest in romance Touches life line = heart is broken easily Is long and curvy = freely expresses emotions and feelings Is straight and parallel to the head line = good handle on emotions Is wavy = many relationships, absence of serious relationships Circle on the line = sad or depressed Broken line = emotional trauma 2. Examine the Head Line This line represents learning style, communication style, intellectualism, and thirst for knowledge. -
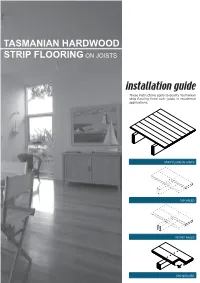
Tasmanian Hardwood Strip Flooring on Joists Guide for Installing
TASMANIAN HARDWOOD STRIP FLOORING ON JOISTS installation guide These instructions apply to quality Tasmanian strip flooring fixed over joists in residential applications. STRIP FLOOR ON JOISTS TOP NAILED SECRET NAILED END MATCHED TOOLS Simple tools are adequate in most applications. Necessary tools are: Tool Requirement Checklist Pencil, tape measure and square Hammer, punch and nail bag Stringline, spirit level and straight edge Hand saw and jig saw Safety glasses, dust mask and knee pads Spacers (about 100mm long and 2 mm thick) Rubber mallet, broom and vacuum cleaner Framing chisel For specialist applications, a drop saw, an air power staple gun, a power actuated fastener system and a cramping system may be useful. MATERIALS Use quality boards of the correct thickness. Grade descriptions for strip flooring are set out in the Australian Standard AS 2796 and are available at: www.tastimber.tas.gov.au. Boards at least 19 mm thick are needed to span 450 mm. Board width - Only secret nail boards up to 85 mm cover width. Secret nailed flooring is fixed through the tongue of specially profiled boards. Since they are only secured with one fastener per joist or batten, their width is limited to 85 mm cover. Board over 85 cover must be top nailed with two fasteners per joist. Use the correct nails for the job. The nail sizes required by Australian Standard 1684 are: Nail sizes for T & G flooring to joists* Nail sizes for T & G flooring to plywood substrate* Nailing Softwood Hardware & Strip flooring Rec. nailing (min.15mm substrate) joists cypress joists thicknes (mm) Hand 65 x 2.8 mm 50 x 2.8 mm 38 x 16 guage chisel point staples or driven bullet head bullet head 19 or 20 38 x 2.2 mm nails at 300mm spacing 32 x 16 guage chisel point staples or Machine 12,19 or 20 driven 65 x 2.5 mm 50 x 2.5 mm 30 x 2.2 mm nails at 200mm spacing *Alternative fasteners can be used for substrates types not listed subject to manufacturers’ recommendation. -

(2004) Does Size Matter? Dominant Discourses About Penises in Western Culture
QUT Digital Repository: http://eprints.qut.edu.au/ McKee, Alan (2004) Does size matter? Dominant discourses about penises in Western culture. Cultural Studies Review 10(2):pp. 168-182. © Copyright 2004 Alan McKee Does size matter? Page 1 Does size matter? Dominant discourses about penises in Western culture Alan McKee Creative Industries Queensland University of Technology Kelvin Grove QLD 4059 Australia [email protected] Alan McKee is consulting editor of Continuum: Journal of Media and Cultural Studies. His most recent book is An Introduction to the Public Sphere (Cambridge University Press, s2004) Does size matter? Page 2 Does size matter? Dominant discourses about penises in Western culture Abstract Does size matter? That is, the size of penises, for women, for their sexual pleasure in lovemaking? This article argues that in Western cultures, the answer to this question has an interesting status. Everybody knows that 'size doesn't matter'; and everybody knows that this is a joke, because it really means that size does matter. The article traces the importance of this ambivalent 'dominant discourse' for thinking about bodies and power. Popular culture presents a complicated and nuanced set of relationships between penises and (various kinds of) power. The presence of these dominant discourses opens up feminist possibilities for commonsense ways of denying power on the basis of morphological characteristics. Keywords: penis; dominant discourses; feminism; sexology; pornography; phallus The joys of a large penis Ally McBeal and her friends are discussing the massive penis of a nude model at their sculpting class. Georgia's husband Billy is not happy about this. -

Regional Handwashing Policy
SOUTHERN CALIFORNIA GRADUATE MEDICAL EDUCATION POLICY AND PROCEDURE POLICY INFECTION PREVENTION AND CONTROL POLICIES EFFECTIVE DATE: SECTION: AND PROCEDURES 7/1/2014 TITLE: Hand Health & Hygiene Page: 1 of 8 BACKGROUND Studies have shown that handwashing causes a reduction in the carriage of potential pathogens on the hands. Microorganisms proliferate on the hands within the moist environment of gloves. Handwashing results in the reduction of patient morbidity and mortality from health care associated infections. The Centers for Disease Control and Prevention states that handwashing is the single most important procedure for preventing health-care associated infections. Artificial nails are more likely than natural nails to harbor pathogens that can lead to health care associated infections. There are four types of hand washing (see body of policy for detailed instructions): TYPE PURPOSE METHOD Routine Handwashing To remove soil and transient Wash hands with soap and microorganisms. water for at least 15 seconds. Hand antisepsis To remove soil and remove or Wash hands with antimicrobial destroy transient soap and water for at least 15 microorganisms. seconds. Hand rub/degerming To destroy transient and Rub alcohol-based hand resident microorganisms on degermer into hands vigorously UNSOILED hands. until dry. Surgical hand scrub To remove or destroy transient Wash hands and forearms with microorganisms and reduce antimicrobial soap and water resident flora. with brush to achieve friction. Or alcohol-based preparation rubbed vigorously -

White Nail As a Static Physical Finding: Revitalization of Physical Examination
Case Report White Nail as a Static Physical Finding: Revitalization of Physical Examination Ryuichi Ohta 1,* and Chiaki Sano 2 1 Community Care, Unnan City Hospital, 699-1221 96-1 Iida, Daito-cho, Unnan 699-1221, Shimane Prefecture, Japan 2 Department of Community Medicine Management, Faculty of Medicine, Shimane University, 89-1 Enya cho, Izumo 693-8501, Shimane Prefecture, Japan; [email protected] * Correspondence: [email protected]; Tel.: +81-9050605330 Abstract: Physical examinations are critical for diagnosis and should be differentiated into static and dynamic categories. One of the static findings is white nail, such as Terry’s and Lindsay’s nails. Here, we report the cases of two older patients with acute diseases who had nail changes that aided evaluation of their clinical course. Two elderly women who presented with acute conditions were initially thought to have normal serum albumin levels. They were found to have white nail with differences in nail involvement of the first finger, which subsequently revealed their hypoalbuminemia. The clinical courses were different following the distribution of nail whitening. Our findings show that examination of a white nail could indicate the previous clinical status more clearly than laboratory data. It can be useful for evaluating preclinical conditions in patients with acute diseases. Further evaluation is needed to establish the relationship between clinical outcomes and the presence of white nail in acute conditions among older patients. Citation: Ohta, R.; Sano, C. White Keywords: Lindsay’s nail; nail findings; nutritional assessment; physical examination; Terry’s nail; Nail as a Static Physical Finding: white nail Revitalization of Physical Examination.