Sleep Debt and Social Jetlag Associated with Sleepiness, Mood, and Work Performance Among Workers in Japan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sleep Matters the Impact of Sleep on Health and Wellbeing Mental Health Awareness Week 2011
Sleep Matters The impact of sleep on health and wellbeing Mental Health Awareness Week 2011 Address Mental Health Foundation Sea Containers House 20 Upper Ground London SE1 9QB United Kingdom Telephone 020 7803 1100 Email [email protected] Website www.HowDidYouSleep.org £10 IBSN 978-1-906162-65-8 Registered charity number England 801130 Scotland SC039714 © Mental Health Foundation 2011 Contents 04 Executive summary 08 Introduction 12 Part 01 – Sleeping and sleep patterns 28 Part 02 – Poor sleep 48 Part 03 – Sleeping well 62 Conclusion 66 Useful resources 68 References 72 Appendix: Sleep diary 76 Acknowledgements 01 ‘The main facts in human life are five: E. M. Forster Executive We spend approximately a Poor sleep over a sustained period One of the most widely used and – The new Public Health Outcomes third of our lives asleep. Sleep leads to a number of problems which successful therapies is Cognitive Framework should include a specific Summary are immediately recognisable, including Behavioural Therapy (CBT). This is outcome on reducing sleep problems is an essential and involuntary fatigue, sleepiness, poor concentration, useful even for people who have across the whole population. process, without which we lapses in memory, and irritability. had insomnia for a long period of time. Sleep should also be reflected in cannot function effectively. A full course of such a therapy with new national mental health outcome It is as important to our Up to one third of the population may a sleep specialist is potentially costly, indicators, including improving bodies as eating, drinking suffer from insomnia (lack of sleep and is most appropriate for people sleep for people who experience and breathing, and is vital for or poor quality sleep). -

Sleep and Its Disorders: Is the Problem
38 ISSN 0049-6804. «Врачеб. дело». 2017, № 1–2 ОБЗОР ЛИТЕРАТУРЫ 43. Williams G. R., Duncan Bassett J. H. Local control of thyroid hormone action: role of type 2 deiodinase Deiodinases: the balance of thyroid hormone // J. of Endocrinol. – 2011. – Vol. 209. – P. 261–272. 44. Wittmann G., Harney J. W., Singru P. S. et al. Inflammation-inducible type 2 deiodinase expres- sion in the leptomeninges, choroid plexus, and at brain blood vessels in male rodents // Endocri- nology. – 2014. – Vol. 155. – P. 2009–2019. 45. Yu J., Koenig R. J. Induction of type 1 iodothyronine deiodinase to prevent the nonthyroidal illness syndrome in mice // Endocrinol. – 2006. – Vol. 147, N 7. – Р. 3580–3585. СУЧАСНІ УЯВЛЕННЯ ПРО СИНДРОМ НЕТИРЕОЇДНОЇ ПАТОЛОГІЇ В КЛІНІЧНІЙ ПРАКТИЦІ Н. О. Абрамова, Н. В. Пашковська (Чернівці) Будь-які гострі та хронічні захворювання, що втягують у патологічний процес весь організм, можуть викликати порушення обміну тиреоїдних гормонів на фоні відсутності супутньої патології щитоподібної залози, гіпофіза та (або) гіпоталамуса. Такі порушення називають «син- дромом нетиреоїдної патології» (СНТП), або «синдромом низького Т3», і зустрічаються у 70 % госпіталізованих. У даному огляді ми розглянули етіологію, патогенез та частково шляхи корекції синдрому нетиреоїдної патології. Ключові слова: синдром нетиреоїдної патології, синдром низького Т3, порушення обміну тиреоїдних гормонів. CURRENT VIEWS ON NONTHYROIDAL ILLNESS SYNDROME IN CLINICAL PRACTICE (REVIEW) N. O. Abramova, N. V. Pashkovska (Chernivtsi, Ukraine) Higher State Educational Establishment of Ukraine «Bukovinian State Medical University» Any acute and chronic diseases that involve the whole organism into pathological process, can cause violation of thyroid hormones metabolism against a background of absence of concomitant diseases of thyroid gland, pituitary gland or hypothalamus. -

Slow-Wave Sleep, Diabetes, and the Sympathetic Nervous System
COMMENTARY Slow-wave sleep, diabetes, and the sympathetic nervous system Derk-Jan Dijk* Surrey Sleep Research Centre, Faculty of Health and Medical Sciences, University of Surrey, Guildford, Surrey GU2 7XP, United Kingdom leep oscillates between two dif- of SWS that has accumulated. The latter less provides supportive evidence for the ferent states: non-rapid eye conclusion was derived from SWS depri- notion that SWS is restorative also for movement (NREM) sleep and vation experiments in which stimuli, usu- the body and that negative effects asso- rapid-eye movement (REM) ally acoustic stimuli [although early on ciated with disruption of this state may Ssleep. Slow-wave sleep (SWS) is a sub- in the history of SWS deprivation, mild extend to the body. state of NREM sleep, and its identifica- electric shocks were used (5)], are deliv- Many other physiological variables are tion is based primarily on the presence ered in response to the ongoing EEG. affected by the behavioral-state sleep, of slow waves, i.e., low-frequency, high- The drive to enter SWS is strong and is the NREM–REM cycle, and SWS. amplitude oscillations in the EEG. Upon the transition from wakefulness to Quantification of SWS is accomplished sleep, heart rate slows down. During by visual inspection of EEG records or Short habitual sleep sleep, the balance of sympathetic and computerized methods such as spectral parasympathetic tone oscillates in syn- analysis based on the fast Fourier trans- has been associated chrony with the NREM–REM cycle. form (FFT). Slow-wave activity (SWA; Analysis of autonomic control of the also referred to as delta power) is a with increased risk variability of heart rate demonstrates quantitative measure of the contribution that, within each NREM episode, as of both the amplitude and prevalence of for diabetes. -

Sleep 101: the Abcs of Getting Your Zzzs
Sleep 101: The ABCs of Getting Your ZZZs Steven D. Brass, MD MPH MBA Director of Neurology Sleep Medicine Clinic UC Davis Health System November 18, 2014 What you will learn: • Why do we sleep? • How much sleep do we need? • What are the effects of sleep deprivation? • What are the different stages of sleep? • What are the types of sleep problems? • What is sleep apnea and how is it treated? • How can we sleep better? Why do we sleep? • Each of us will spend about 1/3 of our lifetime sleeping! • Sleep helps us with: – Memory consolidation – Immune system – Recharge energy for the day – Growth and development How much sleep do we need? Infants : 14-15 hours National Sleep Foundation Secrets of Sleep; National Geographic Magazine . 2010 Adolescents: 8.5-9.25 hours National Sleep Foundation Secrets of Sleep; National Geographic Magazine . 2010 Adult/Elder Sleep: 7-9 hours National Sleep Foundation Secrets of Sleep; National Geographic Magazine . 2010 What are the different stages of sleep? • Non REM Sleep -75% of the night – Stage 1 – Stage 2 – Stage 3 – Stage 4 • REM Sleep -25% of the night – Dreaming Normal Sleep Patterns in Young Adults REM Stage AWAKE NREM REM 1 2 3 4 1 2 3 4 5 6 7 8 Hours of Sleep Adapted from Berger RJ. The sleep and dream cycle. In: Kales A, ed. Sleep Physiology & Pathology: A Symposium. Philadelphia: J.B. Lippincott; 1969. American Academy of Sleep Medicine Sleep Fragmentation Affects Sleep Quality NORMAL SLEEP = Paged ON CALL SLEEP © American Academy of Sleep Medicine, Westchester, IL Why do we dream? • Everyone -

Sleepiness the Wheel
SLEEPINESS AT THE WHEEL WHITE PAPER SLEEPINESS AT THE WHEEL WHITE PAPER Sleepiness at the Wheel WHITE PAPER PREFACE Improving road safety is a priority of the French Government. Among the various causes of road accidents, one of them is especially common on motorways: lack of alertness, which leads to inattention and sleepiness. Lack of alertness is responsible for one in three collisions resulting in deaths on the motorway network, although it is the safest of all road networks! This phenomenon is not fully grasped by the public. Therefore, it is essential to gain knowledge and raise the publics’ awareness as regards sleepiness at the wheel. In more general terms, sleepiness at the wheel remains underestimated both socially and culturally speaking, which is a major issue for road safety and public health. This white book, put together by the French Motorway Companies (ASFA) and the National Institute of Sleep and Vigilance (INSV), presents the most recent knowledge on the subject at both the French and European levels and provides a number of recommendations. By contributing to a better understanding of sleepiness at the wheel, this work will help promote the implementation of new prevention strategies, to further reduce the number of victims on the road. Our objective is to cut down to less than 2000 the number of deaths per year on French roads by 2020. Manuel VALLS French Minister of Interior ASFA and INSV would like to express their deep thanks to the panel of European sleep experts who author this book. Most of them also participate in the research on traffic accidents associated with sleepiness in their own country and thus have contributed to enrich our knowledge and proposals for preventing from the consequences of sleepiness at the wheel. -
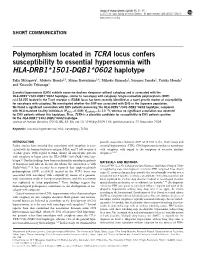
Polymorphism Located in TCRA Locus Confers Susceptibility to Essential Hypersomnia with HLA-DRB1&Ast;1501-DQB1&Ast;0602
Journal of Human Genetics (2010) 55, 63–65 & 2010 The Japan Society of Human Genetics All rights reserved 1434-5161/10 $32.00 www.nature.com/jhg SHORT COMMUNICATION Polymorphism located in TCRA locus confers susceptibility to essential hypersomnia with HLA-DRB1*1501-DQB1*0602 haplotype Taku Miyagawa1, Makoto Honda2,3, Minae Kawashima1,4, Mihoko Shimada1, Susumu Tanaka2, Yutaka Honda3 and Katsushi Tokunaga1 Essential hypersomnia (EHS) exhibits excessive daytime sleepiness without cataplexy and is associated with the HLA-DRB1*1501-DQB1*0602 haplotype, similar to narcolepsy with cataplexy. Single-nucleotide polymorphism (SNP) rs1154155 located in the T-cell receptor a (TCRA) locus has been recently identified as a novel genetic marker of susceptibility for narcolepsy with cataplexy. We investigated whether the SNP was associated with EHS in the Japanese population. We found a significant association with EHS patients possessing the HLA-DRB1*1501-DQB1*0602 haplotype, compared À4 with HLA-matched healthy individuals (Pallele¼0.008; Ppositivity¼5Â10 ), whereas no significant association was observed for EHS patients without this haplotype. Thus, TCRA is a plausible candidate for susceptibility to EHS patients positive for the HLA-DRB1*1501-DQB1*0602 haplotype. Journal of Human Genetics (2010) 55, 63–65; doi:10.1038/jhg.2009.118; published online 20 November 2009 Keywords: essential hypersomnia; HLA; narcolepsy; TCRA INTRODUCTION possible association between SNP rs1154155 in the TCRA locus and Earlier studies have revealed that narcolepsy with cataplexy is asso- essential hypersomnia (EHS), CNS hypersomnia similar to narcolepsy ciated with the human leukocyte antigen (HLA) and T-cell receptor a with cataplexy, with regard to the symptom of excessive daytime (TCRA) genes. -

Sleep Disorders Preeti Devnani
SPECIAL ISSUE 1: INVITED ARTICLE Sleep Disorders Preeti Devnani ABSTRACT Sleep disorders are an increasingly important and relevant burden faced by society, impacting at the individual, community and global level. Varied presentations and lack of awareness can make accurate and timely diagnosis a challenge. Early recognition and appropriate intervention are a priority. The key characteristics, clinical presentations and management strategies of common sleep disorders such as circadian rhythm disorders, restless legs syndrome, REM behavior disorder, hypersomnia and insomnia are outlined in this review. Keywords: Hypersomnia, Insomnia, REM behavior International Journal of Head and Neck Surgery (2019): 10.5005/jp-journals-10001-1362 INTRODUCTION Department of Neurology and Sleep Disorder, Cleveland Clinic, Abu Sleep disorders are becoming increasingly common in this modern Dhabi, United Arab Emirates era, resulting from several lifestyle changes. These complaints may Corresponding Author: Preeti Devnani, Department of Neurology present excessive daytime sleepiness, lack of sleep or impaired and Sleep Disorder, Cleveland Clinic, Abu Dhabi, United Arab Emirates, quality, sleep related breathing disorders, circadian rhythm disorder e-mail: [email protected] misalignment and abnormal sleep-related movement disorders.1 How to cite this article: Devnani P. Sleep Disorders. Int J Head Neck They are associated with impaired daytime functioning, Surg 2019;10(1):4–8. increased risk of cardiovascular and cerebrovascular disease, poor Source of support: Nil glycemic control, risk of cognitive decline and impaired immunity Conflict of interest: None impacting overall morbidity and mortality. Diagnosis of sleep disorders is clinical in many scenarios, The following circadian rhythm sleep–wake disorders adapted polysomnography is a gold standard for further evaluation of from the ICSD-3: intrinsic sleep disorder such as obstructive sleep apnea (OSA) • Delayed sleep–wake phase disorder and periodic limb movement disorder (PLMD). -

Ac 120-100 06/07/10
U.S. Department Advisory of Transportation Federal Aviation Administration Circular Date: 06/07/10 AC No: 120-100 Subject: Basics of Aviation Fatigue Initiated by: AFS-200 Change: 1. PURPOSE. This advisory circular (AC): • Summarizes the content of the FAA international symposium on fatigue, “Aviation Fatigue Management Symposium: Partnerships for Solutions”, June 17-19, 2008; • Describes fundamental concepts of human cognitive fatigue and how it relates to safe performance of duties by employees in the aviation industry; • Provides information on conditions that contribute to cognitive fatigue; and • Provides information on how individuals and aviation service providers can reduce fatigue and/or mitigate the effects of fatigue. 2. APPLICABILITY. This AC is not mandatory and does not constitute a regulation. 3. DEFINITIONS. a. Circadian Challenge. Circadian challenge refers to the difficulty of operating in opposition to an individual’s normal circadian rhythms or internal biological clock. This occurs when the internal biological clock and the sleep/wake cycle do not match the local time. For example, the sleep period is occurring at an adverse circadian phase when the body wants to be awake. Engaging in activities that are opposite of this natural biological system represents the circadian challenge (e.g., night work, shift work, jet lag). b. Cognitive Performance. Cognitive performance refers to the ability to process thought and engage in conscious intellectual activity, e.g., reaction times, problem solving, vigilant attention, memory, cognitive throughput. Various studies have demonstrated the negative effects of sleep loss on cognitive performance. c. Circadian Rhythm. A circadian rhythm is a daily alteration in a person’s behavior and physiology controlled by an internal biological clock located in the brain. -

Sleep Disorders and Sleep Deprivation: an Unmet Public Health Problem
REPORT BRIEF • APRIL 2006 SLEEP DISORDERS AND SLEEP DEPRIVATION: AN UNMET PUBLIC HEALTH PROBLEM It is estimated that 50 to 70 million Americans chronically suffer from a disorder of sleep and wakefulness, hindering daily functioning and adversely affecting their health and longevity. The cumulative effects of sleep loss and sleep disorders represent an under-recognized public health problem and have been associated with a wide range of health consequences including an increased risk of hypertension, diabetes, obesity, depression, heart attack, and stroke. Almost 20 percent of all serious car crash injuries in the general population are associated with driver sleepiness. Hundreds of billions of dollars a year are spent on direct medical costs related to sleep disorders such as doctor visits, hospital services, prescriptions, and over-the-counter medications. Recognizing the health consequences of sleep disorders and sleep deprivation, the American Academy of Sleep Medicine, the National Center on Sleep Disorders Research at the National Institutes of Health, the National Sleep Foundation, and the Sleep Research Society The cumulative requested that the Institute of Medicine review the public health effects of sleep loss significance of sleep, sleep loss, and sleep disorders; examine gaps and sleep disorders in research, education, and training in the public health system and academia; and provide a comprehensive plan for enhancing sleep represent an under- medicine and research. recognized public Sleep Disorders and Sleep Deprivation: An Unmet Public Health health problem and Problem concluded that although scientific opportunities and clinical have been associat- activities in the field are expanding, the available human resources and ed with a wide infrastructural capacity to improve patient care and expand scientific range of health research are insufficient. -
Somnology-Jr-Book.Pdf
1 To Grace Zamudio and Zoe Lee-Chiong. 2 Preface Carpe noctem. Teofilo Lee-Chiong MD Professor of Medicine Division of Sleep Medicine National Jewish Health Denver, Colorado University of Colorado Denver School of Medicine Denver, Colorado Chief Medical Liaison Philips Respironics Murrysville, Pennsylvania 3 Abbreviations AHI Apnea-hypopnea index BPAP Bi-level positive airway pressure CPAP Continuous positive airway pressure CSA Central sleep apnea ECG Electrocardiography EEG Electroencephalography EMG Electromyography EOG Electro-oculography FEV1 Forced expiratory volume in 1 second GABA Gamma-aminobutyric acid N1 NREM stage 1 sleep N2 NREM stage 2 sleep N3 NREM stages 3 (and 4) sleep NREM Non-rapid eye movement O2 Oxygen OSA Obstructive sleep apnea PaCO2 Partial pressure of arterial carbon dioxide PaO2 Partial pressure of arterial oxygen REM Rapid eye movement sleep SaO2 Oxygen saturation SOREMP Sleep onset REM period 4 Table of contents Introduction 15 Neurobiology of sleep 16 Neural systems generating wakefulness 16 Neural systems generating NREM sleep 16 Neural systems generating REM sleep 16 Main neurotransmitters 17 Acetylcholine 17 Adenosine 17 Dopamine 17 Gamma-aminobutyric acid 17 Glutamate 17 Glycine 17 Histamine 18 Hypocretin 18 Melatonin 18 Norepinephrine 18 Serotonin 18 Physiology during sleep 19 Autonomic nervous system 19 Respiratory system 19 Respiratory patterns 19 Cardiovascular system 19 Gastrointestinal system 20 Renal and genito-urinary systems 20 Endocrine system 20 Growth hormone 20 Thyroid stimulating hormone -

Sleep Manual
Sleep and Recovery An applicable approach to a lifestyle of recovery and rest for athletes 2 TABLE OF CONTENTS INTRODUCTION: WHY SLEEP?.................................................................................. 4 SLEEP AS A PREDICTOR OF PERFORMANCE............................................................ 5 EVIDENCE TO SUPPORT THE THEORY...................................................................... 7 WITHOUT SLEEP......................................................................................................... 8 HORMONES, SLEEP, AND RECOVERY....................................................................... 9 SLEEP IS TRAINING TOO! ........................................................................................ 10 THE IMPORTANCE OF TIMING................................................................................ 11 REM SLEEP................................................................................................................. 12 SOCIAL DRUGS AND SLEEP..................................................................................... 12 SLEEP NUTRITION.................................................................................................... 14 STIMULANTS AND DISTURBANCES TO SLEEP....................................................... 15 TECHNOLOGY AND SLEEP....................................................................................... 17 "STUDENT" ATHLETE............................................................................................... 19 SLEEP AND SOCIAL -

Learn About Obstructive Sleep Apnea
Trouble Staying Fully Charged? Learn About Obstructive Sleep Apnea Has someone told you that you snore loudly at night, keeping other people awake? Maybe someone has told you that they have seen you grunting and gasping for breath during sleep? Have you felt tired during the day no matter how much sleep you think you got the previous night? If you can answer yes to these questions then you may be experiencing the symptoms of Obstructive Sleep Apnea, or OSA for short. What is OSA? OSA is a sleep disorder that results in your breathing being repeatedly interrupted during sleep. OSA occurs when the muscles in the back of your throat relax when you fall asleep, and as a result your airway becomes obstructed. When your airway is partially obstructed you snore loudly. When your airway is completely obstructed you experience a pause in breathing called an “apnea”, which can last 10 seconds or much longer. During an apnea you are not getting any oxygen into your lungs! If you are experiencing an apnea you will eventually awaken from sleep just enough to regain muscle control, gasp and take a series of breaths before falling back to sleep. Once asleep, your throat muscles will relax and you will experience another apnea and oxygen will again be cut off. So you will come back up out of sleep to gasp for air, and this process repeats itself over and over again throughout the night. Each apnea restricts the amount of oxygen you get and each arousal, or short awakening out of sleep, reduces your sleep quality and quantity.