Are You Medically Prepared for Hurricane Season?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Listening Patterns – 2 About the Study Creating the Format Groups
SSRRGG PPuubblliicc RRaaddiioo PPrrooffiillee TThhee PPuubblliicc RRaaddiioo FFoorrmmaatt SSttuuddyy LLiisstteenniinngg PPaatttteerrnnss AA SSiixx--YYeeaarr AAnnaallyyssiiss ooff PPeerrffoorrmmaannccee aanndd CChhaannggee BByy SSttaattiioonn FFoorrmmaatt By Thomas J. Thomas and Theresa R. Clifford December 2005 STATION RESOURCE GROUP 6935 Laurel Avenue Takoma Park, MD 20912 301.270.2617 www.srg.org TThhee PPuubblliicc RRaaddiioo FFoorrmmaatt SSttuuddyy:: LLiisstteenniinngg PPaatttteerrnnss Each week the 393 public radio organizations supported by the Corporation for Public Broadcasting reach some 27 million listeners. Most analyses of public radio listening examine the performance of individual stations within this large mix, the contributions of specific national programs, or aggregate numbers for the system as a whole. This report takes a different approach. Through an extensive, multi-year study of 228 stations that generate about 80% of public radio’s audience, we review patterns of listening to groups of stations categorized by the formats that they present. We find that stations that pursue different format strategies – news, classical, jazz, AAA, and the principal combinations of these – have experienced significantly different patterns of audience growth in recent years and important differences in key audience behaviors such as loyalty and time spent listening. This quantitative study complements qualitative research that the Station Resource Group, in partnership with Public Radio Program Directors, and others have pursued on the values and benefits listeners perceive in different formats and format combinations. Key findings of The Public Radio Format Study include: • In a time of relentless news cycles and a near abandonment of news by many commercial stations, public radio’s news and information stations have seen a 55% increase in their average audience from Spring 1999 to Fall 2004. -

LOUISIANA NETWORK DMA Full State Plus Affiliate List
LOUISIANA NETWORK DMA Full State Plus Affiliate List MARKET STATION PARISH SIZE FREQ POWER FORMAT Alexandria DMA Alexandria KEDG-FM Rapides A 106.9 MHZ 6,000 Adult AC Alexandria KZMZ-FM Rapides C 96.9 MHZ 98,000 Rock Alexandria/Tioga KBKK-FM Rapides A 105.5 MHZ 6,000 Classic Country Alexandria/Tioga KLAA-FM Rapides A 103.5 MHZ 6,000 Country Bunkie KEZP-FM Avoyelles C 104.3 MHZ 19,200 Classic Rock Jena KJNA-FM LaSalle D 102.7 MHZ 6,000 Country Leesville KJAE-FM Vernon C 93.5 MHZ 7,500 Country Mansura KZLG-FM Avoyelles C 95.9 MHZ 6,000 AC Marksville KAPB-FM Avoyelles C 97.7 MHZ 6,000 Country Moreauville/Marksville KLIL-FM Avoyelles C 92.1 MHZ 6,000 Oldies Baton Rouge DMA Baton Rouge **** WXOK East Baton Rouge B 1460 KHZ 5,000 Gospel Baton Rouge WPFC East Baton Rouge D 1550 KHZ 5,000 Religious Hammond **** WCDV-FM Tangipahoa C 103.3 MHZ 100,000 AC Morgan City KQKI-FM St. Mary C 95.3 MHZ 16,500 Country New Roads KCLF Pointe Coupee C 1500 KHZ 1,000 Urban White Castle KKAY Iberville D 1590 KHZ 1,000 Variety Lafayette DMA Abbeville KROF Vermilion D 960 KHZ 1,000 Variety Crowley KSIG Acadia C 1450 KHZ 1,000 Easy Listening Erath ****** KRKA-FM Vermilion C 107.9 MHZ 97,000 Urban Eunice KEUN St. Landry C 1490 KHZ 1,000 News/Talk Lafayette KJCB Lafayette B 770 KHZ 1,000 Urban Lafayette ***** KPEL-FM Lafayette B 105.1 MHZ 25,000 News/Talk New Iberia KANE Iberia D 1240 KHZ 1,000 Oldies New Iberia **** KRDJ-FM Iberia C 93.7 MHZ 100,000 Classic Rock Opelousas KSLO St. -

Public Notice >> Licensing and Management System Admin >>
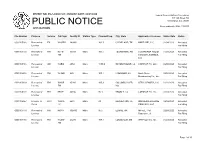
REPORT NO. PN-1-200204-01 | PUBLISH DATE: 02/04/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. 20554 News media info. (202) 418-0500 APPLICATIONS File Number Purpose Service Call Sign Facility ID Station Type Channel/Freq. City, State Applicant or Licensee Status Date Status 0000104614 Renewal of FM WZYQ 191535 Main 101.7 MOUND BAYOU, FENTY FUSS 02/03/2020 Accepted License MS For Filing 0000104644 Renewal of FM WLAU 52618 Main 99.3 HEIDELBERG, MS TELESOUTH 02/03/2020 Accepted License COMMUNICATIONS, For Filing INC. 0000104223 Renewal of FM WKIS 64001 Main 99.9 BOCA RATON, FL ENTERCOM 01/31/2020 Received License LICENSE, LLC Amendment 0000104700 Renewal of FM KQKI-FM 64675 Main 95.3 BAYOU VISTA, LA Teche Broadcasting 02/03/2020 Accepted License Corporation For Filing 0000104619 Renewal of AM KAAY 33253 Main 1090.0 LITTLE ROCK, AR RADIO LICENSE 02/03/2020 Accepted License HOLDING CBC, LLC For Filing 0000103459 Renewal of FX K237GR 154564 95.3 JOHNSON, AR HOG RADIO, INC. 01/31/2020 Accepted License For Filing 0000103767 Renewal of AM WGSV 25675 Main 1270.0 GUNTERSVILLE, GUNTERSVILLE 01/31/2020 Received License AL BROADCASTING Amendment COMPANY, INC. 0000104204 Renewal of FM WQMP 73137 Main 101.9 DAYTONA BEACH ENTERCOM 01/31/2020 Received License , FL LICENSE, LLC Amendment Page 1 of 33 REPORT NO. PN-1-200204-01 | PUBLISH DATE: 02/04/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. 20554 News media info. (202) 418-0500 APPLICATIONS File Number Purpose Service Call Sign Facility ID Station Type Channel/Freq. -
Public Notice >> Licensing and Management System Admin >>
REPORT NO. PN-1-200207-01 | PUBLISH DATE: 02/07/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. 20554 News media info. (202) 418-0500 APPLICATIONS File Number Purpose Service Call Sign Facility ID Station Type Channel/Freq. City, State Applicant or Licensee Status Date Status 0000105266 Renewal of FX W267BI 140992 101.3 CLEVELAND, TN HARTLINE, LLC 02/04/2020 Accepted License For Filing 0000101150 Renewal of FM KTFS- 33541 Main 107.1 TEXARKANA, AR TEXARKANA RADIO 01/28/2020 Accepted License FM CENTER LICENSES, For Filing LLC 0000105186 Renewal of AM WJBO 4054 Main 1150.0 BATON ROUGE, LA CAPSTAR TX, LLC 02/03/2020 Accepted License For Filing 0000104916 Renewal of FM WHMD 680 Main 107.1 HAMMOND, LA North Shore 02/03/2020 Accepted License Broadcasting Co., Inc. For Filing 0000103393 Renewal of FM WACR- 65200 Main 105.3 COLUMBUS AFB, GTR LICENSES, LLC 01/31/2020 Accepted License FM MS For Filing 0000105191 Renewal of FM KRVE 40866 Main 96.1 BRUSLY, LA CAPSTAR TX, LLC 02/03/2020 Accepted License For Filing 0000105367 License To DTV WXPX- 6601 Main 29 BRADENTON, FL ION MEDIA LICENSE 02/04/2020 Accepted Cover TV COMPANY, LLC For Filing 0000105159 Renewal of FM KOYH 190430 Main 95.5 ELAINE, AR Alfred L. 'Pat' 02/03/2020 Accepted License Roberson , III . For Filing 0000101180 Renewal of FM WLSM- 26238 Main 107.1 LOUISVILLE, MS WH Properties, Inc. 01/28/2020 Accepted License FM For Filing Page 1 of 30 REPORT NO. PN-1-200207-01 | PUBLISH DATE: 02/07/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. -

Candidate's Report
CANDIDATE’S REPORT (to be filed by a candidate or his principal campaign committee) 1.Qualifying Name and Address of Candidate 2. Office Sought (Include title of office as OFFICE USE ONLY well MICHAEL J. (MICKEY) MURPHY Report Number: 55622 State Senator 810 N. Columbia Street Date Filed: 1/4/2016 Bogalusa, LA 70427-2916 District 51 Report Includes Schedules: Schedule A-1 Schedule A-2 Schedule B Schedule E-1 3. Date of Primary 10/24/2015 This report covers from 11/2/2015 through 12/21/2015 4. Type of Report: X 180th day prior to primary 40th day after general 90th day prior to primary Annual (future election) 30th day prior to primary Supplemental (past election) 10th day prior to primary 10th day prior to general Amendment to prior report 5. FINAL REPORT if: Withdrawn Filed after the election AND all loans and debts paid Unopposed 6. Name and Address of Financial Institution 7. Full Name and Address of Treasurer (You are required by law to use one or more JOY MURPHY banks, savings and loan associations, or money 810 N. Columbia Street market mutual fund as the depository of all Bogalusa, LA 70427-2916 CITIZENS SAVINGS BANK 1725 Sullivan Drive Bogalusa, LA 70427 9. Name of Person Preparing Report VERNON E DAWSON, JR. Daytime Telephone 225-335-2289 10. WE HEREBY CERTIFY that the information contained in this report and the attached 8. FOR PRINCIPAL CAMPAIGN COMMITTEES ONLY schedules is true and correct to the best of our knowledge, information and belief, and that no a. -

Committee's Election Day Expenditures Report
COMMITTEE’S ELECTION DAY EXPENDITURES REPORT (filed by committees that support or oppose one or more candidates and/or propositions and that are not candidate committees) This report is required to be filed by all committees participating in an election, only if election day expenditures were made. The report is due not later than 10 days after the primary election, and, again, not later than 10 days after the general election if the committee participates in the general election. This form is used to report payments by the political committee (1) for advertising that is broadcast or published on election day, (2) for the services of election day workers, and (3) to organizations for election day activities in support of the committee. NOTE: This report is required in addition to all other required reports. Therefore, the expenditures reported on this report must be reported in subsequent “Committee’s Reports” for this election. 1. Name and Address of Political Committee OFFICE USE ONLY CITIZENS FIGHTING CRIME PAC Report Number: 84250 8680 Bluebonnet Blvd Suite D Baton Rouge, LA 225.7 Date Filed: 11/27/2019 Report Includes Schedules: Schedule A 2. Date of Election 11/16/2019 Primary General X (Check one) 3. Total Expenditures by Category a. Television Advertising (Schedule A) $2,000.00 b. Radio Advertising (Schedule A) $2,227.00 c. Newspaper Advertising (Schedule A) d. Services of Election Day Workers (Schedule B) e. Payments to Organizations for Election Day Activities/Services (Schedule C) For any category in which no election day expenditures were made, write -0- next to the category in Item 5. -
Class C4 Allocation
Friday, January 18, 2013 Ms. Marlene H. Dortch, Secretary Federal Communications Commission 9300 East Hampton Drive Aeeelved & ln:5~eeted Capitol Heights, Maryland 20743 JAN 2 2 2013 Regarding: Petition for Rulemaking FCC Mail Room Ms. Dortch- I am sending to the Commission this original Petition for Rulemaking with four copies with respect to the creation of a broadcast FM C4 allotment class, as well as revisions to certain sections ofthe Commission's Rules, most notably Section 73.215. I certify that everything contained herein is correct to the best of my knowledge. If you have any questions, then please do not hesitate to call me at 601-201-2789, by email at [email protected], or by mail at SSR Communications, Inc., 740 Highway 49 North, Suite R, Flora, MS 39071. Respectfully, -u/,;Pf~· .J~hew K. Wesolowski Chief Executive Officer SSR Communications, Inc. 740 Highway 49 North SuiteR Flora, Mississippi 39071 601-201-2789 .. Received & ln~pected JAN 2 2 2013 Before the FCC Mail Room FEDERAL COMMUNICATIONS COMMISSION Washington, D.C. 20554 In the Matter of ) ) Docket No. MB ----- Amendment of Sections 73.207, 73.210, ) RM------ 73.211, 73.215, and 73.3573 ofthe ) Commission's Rules related to Minimum ) Distance Separation Between Stations, ) Station Classes, Power and Antenna Height ) Requirements, Contour Protection for Short ) Spaced FM Assignments, and Processing ) FM Broadcast Station Applications ) To the Commission PETITION FOR RULEMAKING Matthew K. Wesolowski Chief Executive Officer SSR Communications, Inc. 740 U.S. Highway 49 North SuiteR Flora, MS 39071 (601) 201-2789 [email protected] January 18, 2013 i :,J. -
Public Notice >> Licensing and Management System Admin >>
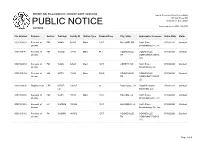
REPORT NO. PN-2-200803-01 | PUBLISH DATE: 08/03/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. 20554 News media info. (202) 418-0500 ACTIONS File Number Purpose Service Call Sign Facility ID Station Type Channel/Freq. City, State Applicant or Licensee Status Date Status 0000104839 Renewal of FM WAKH 58935 Main 105.7 MCCOMB, MS North Shore 07/30/2020 Granted License Broadcasting Co., Inc. 0000109147 Renewal of FM WGSQ 13819 Main 94.7 COOKEVILLE, COOKEVILLE 07/30/2020 Granted License TN COMMUNICATIONS, LLC 0000104834 Renewal of FM WAZA 82529 Main 107.7 LIBERTY, MS North Shore 07/30/2020 Granted License Broadcasting, Inc. 0000109134 Renewal of AM WPTN 13820 Main 780.0 COOKEVILLE, COOKEVILLE 07/30/2020 Granted License TN COMMUNICATIONS, LLC 0000116390 Displacement LPD WEAZ- 190207 26 Baton rouge, LA Digital Networks- 07/30/2020 Granted LD Southeast, LLC 0000105003 Renewal of FM WJSH 19616 Main 104.7 FOLSOM, LA North Shore 07/30/2020 Granted License Broadcasting Co., Inc. 0000104888 Renewal of FX W279DB 152562 103.7 HAMMOND, LA North Shore 07/30/2020 Granted License Broadcasting, Co., Inc. 0000109112 Renewal of FX W299BY 140072 107.7 COOKEVILLE, COOKEVILLE 07/30/2020 Granted License TN COMMUNICATIONS, LLC Page 1 of 4 REPORT NO. PN-2-200803-01 | PUBLISH DATE: 08/03/2020 Federal Communications Commission 445 12th Street SW PUBLIC NOTICE Washington, D.C. 20554 News media info. (202) 418-0500 ACTIONS File Number Purpose Service Call Sign Facility ID Station Type Channel/Freq. City, State Applicant or Licensee Status Date Status 0000105928 Renewal of FM WJLE- 37052 Main 101.7 SMITHVILLE, CENTER HILL 07/30/2020 Granted License FM TN BROADCASTING CORP., INC. -

MF01/N06 Plus Postage
DOCUMENT RESUME ED 292 440 IR 013 191 TITLE A Report to the People. 20Years of Your National Commitment to Public Broadcasting, 1967-1987. 1986 Annual Report. INSTITUTION Corporation for Public Broadcasting, Washington, D.C. REPORT NO ISBN-0-89776-100-6 PUB DATE [15 May 87] NOTE 129p.; Photographs will not reproduce well. PUB TYPE Reports Descriptive (141) EDRS PRICE MF01/n06 Plus Postage. DESCRIPTORS Annual Reports; Cultural Enrichment; Educational Radio; *Educational Television; *Financial Support; *Programing (Broadcast); *Public Television; *Television Viewing IDENTIFIERS *Annenberg CPB Project; *Corporation for Public Broadcasting ABSTRACT This annual report for the Corporation for Public Broadcasting (CPB) for fiscal year 1986 also summarizes the CPB's activities over the last 20 years. The front inside cover folds out to three pages and provides a chronology of the important events in CPB history from its inception in 1967 to 1987. A narrative report on the CPB's 20 years of operation highlights its beginnings, milestones, programming, and audiences; the broadcasting system; and funding. Comments in support of public television by a wide variety of public figures concludes this portion of the report. The 1986 annual report provides information on television programming, radio programming, community outreach, adult learning, program support activities, and system support activities for that fiscal year. The CPB Board of Directors and officers are also listed, and a financial accounting by the firm of Peat, Marwick, Mitchell & Co. is provided. The text is supplemented by a number of graphs, figures, and photographs. (EW) ********************************************************************** Reproductions supplied by EDRS are the best that can be made from the original document. -

US1 Distribution
1 US1 Distribution PR Newswire’s U.S. Distribution delivers your messages across the most trusted and comprehensive content distribution network in the industry, providing the broadest reach and sharpest targeting available. Business Alabama Monthly - Birmingham Bureau ALABAMA (Birmingham) Magazine Cherokee County Herald (Centre) Cullman Times (Cullman) Coastal Living Magazine (Birmingham) Decatur Daily (Decatur) Southern Living (Birmingham) Dothan Eagle (Dothan) Southern Breeze (Gulf Shores) Enterprise Ledger (Enterprise) Civil Air Patrol News (Maxwell AFB) Fairhope Courier (Fairhope) Business Alabama Monthly (Mobile) Courier Journal (Florence) Prime Montgomery (Montgomery) Florence Times Daily (Florence) Fabricating & Metalworking Magazine (Pinson) Times Daily (Florence) News Service Fort Payne Times-Journal (Fort Payne) Gadsden Times, The (Gadsden) Associated Press - Birmingham Bureau (Birmingham) Latino News (Gadsen) Associated Press - Mobile Bureau (Mobile) News-Herald (Geneva) Associated Press - Montgomery Bureau Huntsville Times, The (Huntsville) (Montgomery) Daily Mountain Eagle, The (Jasper) Newspaper Fairhope Courier, The (Mobile) Mobile Press-Register (Mobile) The Sand Mountain Reporter (Albertville) Montgomery Advertiser (Montgomery) The Outlook (Alexander) Opelika-Auburn News (Opelika) Anniston Star (Anniston) Pelican, The (Orange Beach) Athens News Courier (Athens) The Citizen of East Alabama (Phenix City) Atmore Advance (Atmore) Scottsboro Daily Sentinel (Scottsboro) Lee County Eagle, The (Auburn) Selma Times Journal (Selma) -
Go Viral 9-5.Pdf
Hello fellow musicians, artists, rappers, bands, and creatives! I’m excited you’ve decided to invest into your music career and get this incredible list of music industry contacts. You’re being proactive in chasing your own goals and dreams and I think that’s pretty darn awecome! Getting your awesome music into the media can have a TREMENDOUS effect on building your fan base and getting your music heard!! And that’s exactly what you can do with the contacts in this book! I want to encourage you to read the articles in this resource to help guide you with how and what to submit since this is a crucial part to getting published on these blogs, magazines, radio stations and more. I want to wish all of you good luck and I hope that you’re able to create some great connections through this book! Best wishes! Your Musical Friend, Kristine Mirelle VIDEO TUTORIALS Hey guys! Kristine here J I’ve put together a few tutorials below to help you navigate through this gigantic list of media contacts! I know it can be a little overwhelming with so many options and places to start so I’ve put together a few videos I’d highly recommend for you to watch J (Most of these are private videos so they are not even available to the public. Just to you as a BONUS for getting “Go Viral” TABLE OF CONTENTS What Do I Send These Contacts? There isn’t a “One Size Fits All” kind of package to send everyone since you’ll have a different end goal with each person you are contacting. -

Exhibit 2181
Exhibit 2181 Case 1:18-cv-04420-LLS Document 131 Filed 03/23/20 Page 1 of 4 Electronically Filed Docket: 19-CRB-0005-WR (2021-2025) Filing Date: 08/24/2020 10:54:36 AM EDT NAB Trial Ex. 2181.1 Exhibit 2181 Case 1:18-cv-04420-LLS Document 131 Filed 03/23/20 Page 2 of 4 NAB Trial Ex. 2181.2 Exhibit 2181 Case 1:18-cv-04420-LLS Document 131 Filed 03/23/20 Page 3 of 4 NAB Trial Ex. 2181.3 Exhibit 2181 Case 1:18-cv-04420-LLS Document 131 Filed 03/23/20 Page 4 of 4 NAB Trial Ex. 2181.4 Exhibit 2181 Case 1:18-cv-04420-LLS Document 132 Filed 03/23/20 Page 1 of 1 NAB Trial Ex. 2181.5 Exhibit 2181 Case 1:18-cv-04420-LLS Document 133 Filed 04/15/20 Page 1 of 4 ATARA MILLER Partner 55 Hudson Yards | New York, NY 10001-2163 T: 212.530.5421 [email protected] | milbank.com April 15, 2020 VIA ECF Honorable Louis L. Stanton Daniel Patrick Moynihan United States Courthouse 500 Pearl St. New York, NY 10007-1312 Re: Radio Music License Comm., Inc. v. Broad. Music, Inc., 18 Civ. 4420 (LLS) Dear Judge Stanton: We write on behalf of Respondent Broadcast Music, Inc. (“BMI”) to update the Court on the status of BMI’s efforts to implement its agreement with the Radio Music License Committee, Inc. (“RMLC”) and to request that the Court unseal the Exhibits attached to the Order (see Dkt.