Vaccine Highlights
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

362.Full.Pdf
AMERICAN ACADEMY OF PEDIATRICS Committee on Infectious Diseases Policy Statement: Recommendations for the Prevention of Pneumococcal Infections, Including the Use of Pneumococcal Conjugate Vaccine (Prevnar), Pneumococcal Polysaccharide Vaccine, and Antibiotic Prophylaxis ABSTRACT. Heptavalent pneumococcal conjugate vac- lular pertussis; HbOC, Haemophilus influenzae type b conjugate cine (PCV7) is recommended for universal use in chil- vaccine; HIV, human immunodeficiency virus; AOM, acute otitis dren 23 months and younger, to be given concurrently media. with other recommended childhood vaccines at 2, 4, 6, and 12 to 15 months of age. For children 7 to 23 months he purpose of this report is to provide recom- old who have not received previous doses of PCV7, ad- ministration of a reduced number of doses is recom- mendations for use of the heptavalent pneumo- mended. Two doses of PCV7 are recommended for chil- Tcoccal conjugate vaccine (PCV7), Prevnar (Led- dren 24 to 59 months old at high risk of invasive erle Laboratories, Pearl River, NY; Wyeth-Ayerst pneumococcal infection—including children with func- Pharmaceuticals, Marietta, PA), and 23-valent pneumo- tional, anatomic, or congenital asplenia; infection with coccal polysaccharide (23PS) vaccines. In addition, rec- human immunodeficiency virus; and other predisposing ommendations for the continuing use of antibiotic pro- conditions—who have not been immunized previously phylaxis in children with sickle cell disease (SCD) and with PCV7. Recommendations have been made for use of asplenia will be given, and the use of antibiotics and 23-valent pneumococcal polysaccharide (23PS) vaccine in vaccines in children who attend out-of-home care will high-risk children to expand serotype coverage. -

Yellow Fever Vaccine See Hojas De Información Sobre Vacunas Están Disponibles En Español Y En Muchos Otros What You Need to Know Idiomas
VACCINE INFORMATION STATEMENT Many Vaccine Information Statements are available in Spanish and other languages. Yellow Fever Vaccine See www.immunize.org/vis Hojas de información sobre vacunas están disponibles en español y en muchos otros What You Need to Know idiomas. Visite www.immunize.org/vis 1 What is yellow fever? 3 Yellow fever vaccine Yellow fever is a serious disease caused by the yellow Yellow fever vaccine is a live, weakened virus. It is fever virus. It is found in certain parts of Africa and given as a single shot. For people who remain at risk, a South America. booster dose is recommended every 10 years. Yellow fever is spread through the bite of an infected Yellow fever vaccine may be given at the same time as mosquito. It cannot be spread person to person by direct most other vaccines. contact. Who should get yellow fever vaccine? People with yellow fever disease usually have to be • Persons 9 months through 59 years of age traveling hospitalized. Yellow fever can cause: to or living in an area where risk of yellow fever is • fever and flu-like symptoms known to exist, or traveling to a country with an entry • jaundice (yellow skin or eyes) requirement for the vaccination. • bleeding from multiple body sites • Laboratory personnel who might be exposed to yellow • liver, kidney, respiratory and other organ failure fever virus or vaccine virus. • death (20% - 50% of serious cases) Information for travelers can be found online through CDC (www.cdc.gov/travel), the World Health 2 How can I prevent yellow fever? Organization (www.who.int), and the Pan American Health Organization (www.paho.org). -

Recombivax HB , YF-Vax – Drug Shortages
Recombivax HB®, YF-Vax® – Drug shortages • The drug shortages of Recombivax HB (hepatitis B vaccine, recombinant) and YF-Vax (yellow fever virus strain 17d-204 live antigen) are ongoing. Recombivax HB and YF-Vax have been unavailable for at least 90 days. Product Description NDC # Recombivax HB (hepatitis B vaccine, recombinant) 0.5 mL (5 mcg) 0006-4981-00, 0006- pediatric/adolescent formulation 4093-02, 0006-4093-09 single-dose vials and prefilled syringes Recombivax HB (hepatitis B vaccine, 0006-4995-00, 0006- recombinant) 1 mL (10 mcg) adult 4995-41, 0006-4094-02, formulation single-dose vials and 0006-4094-09 prefilled syringes YF-Vax (yellow fever virus strain 17-d- 49281-0915-01, 49281- 2014 live antigen) single- and multi- 0915-05 dose vials — The shortage of Recombivax HB is due to increased global demand. — The Recombivax HB pediatric/adolescent and adult formulations are estimated to be available in the first half of 2018 and the first half of 2019, respectively. — The Recombivax HB dialysis formulation is available; however, the dose is different than the adult and pediatric/adolescent formulations. — YF-Vax is unavailable because the manufacturer, Sanofi Pasteur, is transitioning production to a new facility in 2018. YF-Vax is estimated to be available by mid-2018. • Recombivax HB is indicated for prevention of infection caused by all known subtypes of hepatitis B virus. — Engerix-B™ (hepatitis B vaccine, recombinant) is another currently available vaccine that carries the same indication as Recombivax HB. Engerix-B is not in shortage. — Heplisav-B™ (hepatitis B vaccine, recombinant) was recently approved and carries the same indication as Recombivax HB. -
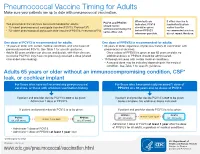
Pneumococcal Vaccine Timing for Adults Make Sure Your Patients Are up to Date with Pneumococcal Vaccination
Pneumococcal Vaccine Timing for Adults Make sure your patients are up to date with pneumococcal vaccination. When both are If either vaccine is PCV13 and PPSV23 Two pneumococcal vaccines are recommended for adults: indicated, PCV13 inadvertently given should not be 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar13®) should be given earlier than the administered during the ® before PPSV23 recommended window, 23-valent pneumococcal polysaccharide vaccine (PPSV23, Pneumovax 23) same office visit. whenever possible. do not repeat the dose. One dose of PCV13 is recommended for adults: One dose of PPSV23 is recommended for adults: 19 years or older with certain medical conditions and who have not 65 years or older, regardless of previous history of vaccination with previously received PCV13. See Table 1 for specific guidance. pneumococcal vaccines. Adults 65 years or older can discuss and decide, with their clinician, – Once a dose of PPSV23 is given at age 65 years or older, no to receive PCV13 if they have not previously received a dose (shared additional doses of PPSV23 should be administered. clinical decision-making). 19 through 64 years with certain medical conditions. – A second dose may be indicated depending on the medical condition. See Table 1 for specific guidance. Adults 65 years or older without an immunocompromising condition, CSF* leak, or cochlear implant For those who have not received any pneumococcal For those who have previously received 1 dose of vaccines, or those with unknown vaccination history PPSV23 at ≥ 65 years and no doses of PCV13 If patient and provider decide PCV13 is not to be given: If patient and provider decide PCV13 is not to be given: Administer 1 dose of PPSV23. -
Yellow Fever Vaccine Program Manual
Vaccine Preventable Disease Program Yellow Fever Vaccine Program Manual New Jersey Department of Health Vaccine Preventable Disease Program P.O. Box 369 Trenton, NJ 08625 Phone 609-826-4860 Table of Contents Yellow Fever Certification ......................................................... 1 Certified Uniform Yellow Fever Stamp Holder .......................... 1 Certified Yellow Fever Vaccine Uniform Stamp ........................ 1 Who Can Apply? ...................................................................... 2 Application Requirements ........................................................ 2 Responsibilities of Uniform Stamp Holder ................................ 3 Period of Certification/Recertification ........................................ 4 Responsibilities of Yellow Fever Vaccine Coordinator .............. 4 Registries ................................................................................. 4 Change Notifications ................................................................ 5 Replacement Stamp ................................................................. 5 Standards, Recordkeeping, and Storage .................................. 5 YEL LOW FEVER VACCINE PR OGRAM Yellow Fever Certification According to International Health Regulations, yellow fever vaccine must be administered at certified yellow fever vaccination centers. Healthcare providers are authorized to administer the vaccine by state health departments and the states then report certified providers to the Centers for Disease Control and Prevention -

Adults with DIABETES Are Among Those Who Need Pneumococcal
Patients with diabetes are at an increased risk for complications from pneumococcal disease. Diabetes may be a unique risk factor for increased incidence of sepsis associated with pneumococcal infection. One of the reasons people with diabetes are at greater risk for pneumococcal disease is that they may have abnormalities in immune function that affect their reaction to infection. Pneumococcal disease causes serious illnesses like pneumonia, meningitis, and sepsis. Pneumococcal disease is serious and deadly. In the US, pneumococcal pneumonia, meningitis, and sepsis kill tens of thousands each year. Pneumococcal disease survivors may suffer hearing loss, seizures, blindness, or paralysis. Pneumococcal vaccination is recommended for all adults with diabetes. Adults with DIABETES Are Among Those Who Need Pneumococcal Vaccination There are two types of pneumococcal vaccine recommended for US adults: a pneumococcal conjugate vaccine (PCV13) and a pneumococcal polysaccharide vaccine (PPSV23). Adults 65 and older, and adults age 19 to 64 years with any of the following need to receive both vaccines: immunocompromising conditions or treatments (e.g., HIV/AIDS, leukemia, lymphoma, Hodgkin disease, radiation therapy); a damaged or missing spleen; cochlear implants; or cerebrospinal fluid leaks. Other adults for whom pneumococcal vaccination is recommended only need PPSV23, but may need more than one dose and will need PCV13 when they, too, reach age 65. Please refer to the Adult Pneumococcal Vaccination Guide or visit cdc.gov/vaccines/vpd-vac/pneumo/ for details on timing of vaccine doses. For more information and resources to educate patients about pneumococcal disease, visit adultvaccination.org/professional-resources/pneumo This initiative is supported by unrestricted educational grants from Merck & Co., Inc. -

Yellow Fever Vaccine
Yellow Fever Vaccine: Current Supply Outlook UNICEF Supply Division May 2016 0 Yellow Fever Vaccine - Current Supply Outlook May 2016 This update provides revised information on yellow fever vaccine supply availability and increased demand. Despite slight improvements in availability and the return of two manufacturers from temporary suspension, a constrained yellow fever vaccine market will persist through 2017, exacerbated by current emergency outbreak response requirements. 1. Summary Yellow fever vaccine (YFV) supply through UNICEF remains constrained due to limited production capacity. Despite the return of two manufacturers from temporary suspension, the high demand currently generated from the yellow fever (YF) outbreak in Angola, in addition to potential increased outbreak response requirements in other geographic regions, outweigh supply. The demand in response to the current YF outbreak in Angola could negatively impact the supply availability for some routine immunization programme activities. UNICEF anticipates a constrained global production capacity to persist through 2017. UNICEF has long-term arrangements (LTAs) with four YFV suppliers to cover emergency stockpile, routine immunization, and preventative campaign requirements. During 2015, UNICEF increased total aggregate awards to suppliers to reach approximately 98 million doses for 2016- 2017. However, whereas supply can meet emergency stockpile and routine requirements, it is insufficient to meet all preventive campaign demands, which increased the total demand through UNICEF to 109 million doses. The weighted average price (WAP) per dose for YFV increased 7% a year on average since 2001, from US$ 0.39 to reach US$ 1.04 in 2015. Given the continued supply constraints, UNICEF anticipates a YFV WAP per dose of US$1.10 in the near-term. -

2021 Medicare Vaccine Coverage Part B Vs Part D
CDPHP® Medicare Advantage Vaccine Coverage Guide Part B (Medical) vs. Part D (Pharmacy) Medicare Part B (Medical): Medicare Part D (Pharmacy): Vaccinations or inoculations Vaccinations or inoculations are included when the administration is (except influenza, pneumococcal, reasonable and necessary for the prevention of illness. and hepatitis B for members at risk) are excluded unless they are directly related to the treatment of an injury or direct exposure to a disease or condition. • Influenza Vaccine (Flu) • BCG Vaccine • Pneumococcal Vaccine • Diphtheria/Tetanus/Acellular Pertussis Vaccine (ADACEL, (Pneumovax, Prevnar 13) BOOSTRIX, DAPTACEL, INFANRIX) • Hepatitis B Vaccine • Diphtheria/Tetanus/Acellular Pertussis/Inactivated Poliovirus (Recombivax, Engerix-B) Vaccine (KINRIX, QUADRACEL) for members at moderate • Diphtheria/Tetanus Vaccine (DT, Td, TDVAX, TENIVAC) to high risk • Diphtheria/Tetanus/Acellular Pertussis/Inactivated Poliovirus Vac • Other vaccines when directly cine/ Haemophilus Influenzae Type B Conjugate Vaccine (PENTACEL) related to the treatment of an • Diphtheria/Tetanus/Acellular Pertussis/Inactivated Poliovirus injury or direct exposure to a Vaccine/Hepatitis B Vaccine (PEDIARIX) disease or condition, such as: • Haemophilus Influenzae Type B Conjugate Vaccine (ActHIB, PedvaxHIB, • Antivenom Sera Hiberix) • Diphtheria/Tetanus Vaccine • Hepatitis A Vaccine, Inactivated (VAQTA) (DT, Td, TDVAX, TENIVAC) • Hepatitis B Vaccine, Recombinant (ENGERIX-B, RECOMBIVAX HB) • Rabies Virus Vaccine for members at low risk (RabAvert, -

Global Immunization News 25 February 2011
Global Immunization News 25 February 2011 World Health Organization Global Immunization News Inside this issue: Technical Information Meeting of the Global Advisory 2 Committee on Vaccine Safety Polio eradication mourns loss of 2 NEW VACCINES, NEW true polio champion OPPORTUNITIES Announcements from The SIVAC 3 25/02/2011 from Hayatee Hasan, WHO/HQ Initiative In the past two months, four countries ― WHO position on pandemic influ- 3 Guyana, Kenya, Sierra Leone and Yemen ― enza vaccination following reports of narcolepsy subsequent to use of have introduced the pneumococcal conjugate Pandemrix vaccine. They represent the first of a series of countries introducing the vaccine in 2011. PHOTO Cold Chain and Logistics Taskforce 3 WHO concludes that quality issues 4 These introductions represent a major relating to Quinvaxem production milestone - the gap between access to new have been resolved vaccines between developed and developing AFRICA 4-6 countries is shortening; it is extraordinary to The launching of the Pneumococcal see a new vaccine launched in a developing conjugate vaccine (PCV-13) in Si- erra Leone country within one to two years of its introduction in the Americas and Europe, Kenya launches ten-valent pneumo- while in the past, it has taken several years coccal conjugate vaccine (PCV10) Vaccine carrier containing pneumococcal vaccine in (averaging 15 years) between the Kenya Meetings held in afro central introduction of new vaccines in developed and developing countries. AMERICAS 6-8 Peru introduces nationwide HPV vaccination; Argentina announces For more information regarding the launches in these countries, please see the articles on HPV vaccine introduction Kenya, Sierra Leone and Yemen. -

Optimizing Vaccine Allocation for COVID-19 Vaccines Shows The
ARTICLE https://doi.org/10.1038/s41467-021-23761-1 OPEN Optimizing vaccine allocation for COVID-19 vaccines shows the potential role of single-dose vaccination ✉ Laura Matrajt 1 , Julia Eaton 2, Tiffany Leung 1, Dobromir Dimitrov1,3, Joshua T. Schiffer1,4,5, David A. Swan1 & Holly Janes1 1234567890():,; Most COVID-19 vaccines require two doses, however with limited vaccine supply, policy- makers are considering single-dose vaccination as an alternative strategy. Using a mathe- matical model combined with optimization algorithms, we determined optimal allocation strategies with one and two doses of vaccine under various degrees of viral transmission. Under low transmission, we show that the optimal allocation of vaccine vitally depends on the single-dose efficacy. With high single-dose efficacy, single-dose vaccination is optimal, preventing up to 22% more deaths than a strategy prioritizing two-dose vaccination for older adults. With low or moderate single-dose efficacy, mixed vaccination campaigns with com- plete coverage of older adults are optimal. However, with modest or high transmission, vaccinating older adults first with two doses is best, preventing up to 41% more deaths than a single-dose vaccination given across all adult populations. Our work suggests that it is imperative to determine the efficacy and durability of single-dose vaccines, as mixed or single-dose vaccination campaigns may have the potential to contain the pandemic much more quickly. 1 Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center, Seattle, WA, USA. 2 School of Interdisciplinary Arts and Sciences, University of Washington, Tacoma, WA, USA. 3 Department of Applied Mathematics, University of Washington, Seattle, WA, USA. -

Vaccines-Pneumococcal- Influenza- Shingles Q and A
www.RxFiles.ca - July 2019 RxFiles Q&A Summary A Crawley BSP; J Bareham BSP VACCINES: Pneumococcal, Influenza, & Shingles Immunization Guidelines and Saskatchewan Health Coverage Considerations Vaccines prevent morbidity and mortality to various degrees. Many vaccines are publicly funded, especially if potentially life-saving. When guideline recommendations & public coverage differ, clinicians/patients must weigh the evidence for benefit versus the out-of-pocket patient cost. Note: vaccine costs listed in this document do not include markup, dispensing fees, or administration fees, which can vary depending on who is administering the vaccine. 1. Who may benefit from a PNEUMOCOCCAL vaccine in Saskatchewan? Available vaccines include the PNEUMOVAX 23-valent vaccine ($24) and the PREVNAR 13-valent vaccine ($103). Covered in Sask:1 Evidence for benefit Clinical Controversies 1 dose of PNEUMOVAX for anyone A single pneumococcal vaccination Immunization guidelinesNACI suggest that if ≥65 years old. appears to reduce the risk of PNEUMOVAX was given before the age of 65, a booster 1 dose of PNEUMOVAX for anyone community-acquired pneumonia by dose should be given 5 years later to all patients with specific medical conditions 30% (NNT = 55) and the risk of a COPD regardless of risk factors.18 This recommendation is (e.g. diabetes, COPD, others*). exacerbation by 40% (NNT = 8).2,19,20 based on the tendency for older adults to have a 2 doses of PNEUMOVAX spaced 5+ Benefits are consistent regardless of weakened immune system. years apart for anyone with which vaccine formulation is used.2-4 Immunization guidelines suggest that the theoretical specific high risk medical No trials have yet assessed the efficacy greater potency of PREVNAR over PNEUMOVAX may conditions (e.g. -

The Present and Future of Yellow Fever Vaccines
pharmaceuticals Review The Present and Future of Yellow Fever Vaccines Clairissa A. Hansen 1 and Alan D. T. Barrett 1,2,* 1 Department of Pathology, University of Texas Medical Branch, Galveston, TX 77555-4036, USA; [email protected] 2 Sealy Institute for Vaccine Sciences, University of Texas Medical Branch, Galveston, TX 77555-4036, USA * Correspondence: [email protected] Abstract: The disease yellow fever (YF) is prevented by a live-attenuated vaccine, termed 17D, which has been in use since the 1930s. One dose of the vaccine is thought to give lifelong (35+ years) protective immunity, and neutralizing antibodies are the correlate of protection. Despite being a vaccine-preventable disease, YF remains a major public health burden, causing an estimated 109,000 severe infections and 51,000 deaths annually. There are issues of supply and demand for the vaccine, and outbreaks in 2016 and 2018 resulted in fractional dosing of the vaccine to meet demand. The World Health Organization (WHO) has established the “Eliminate Yellow Fever Epidemics” (EYE) initiative to reduce the burden of YF over the next 10 years. As with most vaccines, the WHO has recommendations to assure the quality, safety, and efficacy of the YF vaccine. These require the use of live 17D vaccine only produced in embryonated chicken eggs, and safety evaluated in non- human primates only. Thus, any second-generation vaccines would require modification of WHO recommendations if they were to be used in endemic countries. There are multiple second-generation YF vaccine candidates in various stages of development that must be shown to be non-inferior to the current 17D vaccine in terms of safety and immunogenicity to progress through clinical trials to potential licensing.