The Association Between Intron 4 VNTR, E298A and IVF 23+10 G/T
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Meat Curing and Sodium Nitrite
MEDIA MYTHCRUSHER Meat Curing and Sodium Nitrite The use of nitrite to produce cured meats like salami, ham, bacon and hot dogs, is a safe, regulated practice that has distinct public health benefits. However, much confusion and even mythology surrounds nitrite. Being mindful of key words and statistics and providing appropriate context can help reporters improve the accuracy of their coverage and the information that is passed on to readers and viewers. We’ve compiled ten tips to improve accuracy when writing about the use of sodium nitrite in cured meats. #1: Nitrite is not ‘unnatural’. Before the terms nitrate and nitrite are often used refrigeration was available, humans salted and interchangeably, meat companies mainly use dried meat to preserve it. It was discovered sodium nitrite to cure meat, not sodium nitrate. that the nitrate in saltpeter was extremely At the turn of the 20th century, German effective in causing a chemical reaction known scientists discovered nitrite (and not nitrate) as “curing.” Not only did this give meat a was the active form of these curing salts. When distinct taste and flavor, it also preserved it and added directly, rather than as nitrate, meat prevented the growth of Clostridium botulinum, processors can have better control of this which causes botulism. important curing ingredient and more closely manage how much they are adding. Later on, scientists came to understand that nitrate naturally found in the environment #3: Cured meats are a miniscule source of converts to nitrite when in the presence of total human nitrite intake. Scientists say that certain bacteria. -

Inhibition of Grb2‑Mediated Activation of MAPK Signal Transduction
566 ONCOLOGY LETTERS 4: 566-570, 2012 Inhibition of Grb2‑mediated activation of MAPK signal transduction suppresses NOR1/CB1954‑induced cytotoxicity in the HepG2 cell line RONG GUI1, DENGQING LI1, GUANNAN QI1,2, ALI SUHAD2 and XINMIN NIE1 1Clinical Laboratory Centre of the Third Xiangya Hospital, Central South University, Changsha, Hunan 410013, P.R. China; 2Hormones and Cancer Research Unit, Royal Victoria Hospital, McGill University, Quebec H3A 1A1, Canada Received March 12, 2012; Accepted June 22, 2012 DOI: 10.3892/ol.2012.774 Abstract. The nitroreductase oxidored-nitro domain Introduction containing protein 1 (NOR1) gene may be involved in the chemical carcinogenesis of hepatic cancer and nasopharyn- The oxidored-nitro domain containing protein 1 (NOR1) gene geal carcinoma (NPC). We have previously demonstrated that was previously cloned in our laboratory at the Third Xiangya NOR1 overexpression is capable of converting the monofunc- Hospital (Hunan, China) using suppression subtractive hybrid- tional alkylating agent 5-(aziridin-1-yl)-2,4-dinitrobenzamide ization and cDNA microarrays (1,2). By examining the human (CB1954) into a toxic form by reducing the 4-nitro group of genome working sequence, it has been identified that that the CB1954. Toxic CB1954 is able to enhance cell killing in the NOR1 gene is located on 1p34.3 and contains 10 exons and NPC cell line CNE1; however, the underlying mechanisms 9 introns. Additionally, the PROSITE database identified remain unknown. Using cDNA microarrays and quantitative two possible cAMP and cGMP-dependent protein kinase real-time PCR, we previously discovered that NOR1 increases phosphorylation sites, two tyrosine phosphorylation sites the expression of growth factor receptor-bound protein 2 and four N-myristoylation sites in NOR1. -

Role of Sodium/Calcium Exchangers in Tumors
biomolecules Review Role of Sodium/Calcium Exchangers in Tumors Barbora Chovancova 1, Veronika Liskova 1, Petr Babula 2 and Olga Krizanova 1,2,* 1 Institute of Clinical and Translational Research, Biomedical Research Center, Slovak Academy of Sciences, Dubravska cesta 9, 845 45 Bratislava, Slovakia; [email protected] (B.C.); [email protected] (V.L.) 2 Department of Physiology, Faculty of Medicine, Masaryk University, Kamenice 753/5, 625 00 Brno, Czech Republic; [email protected] * Correspondence: [email protected]; Tel.: +4212-3229-5312 Received: 6 August 2020; Accepted: 29 August 2020; Published: 31 August 2020 Abstract: The sodium/calcium exchanger (NCX) is a unique calcium transport system, generally transporting calcium ions out of the cell in exchange for sodium ions. Nevertheless, under special conditions this transporter can also work in a reverse mode, in which direction of the ion transport is inverted—calcium ions are transported inside the cell and sodium ions are transported out of the cell. To date, three isoforms of the NCX have been identified and characterized in humans. Majority of information about the NCX function comes from isoform 1 (NCX1). Although knowledge about NCX function has evolved rapidly in recent years, little is known about these transport systems in cancer cells. This review aims to summarize current knowledge about NCX functions in individual types of cancer cells. Keywords: sodium-calcium exchanger; cancer cells; calcium; apoptosis 1. Background Intracellular calcium ions are considered the most abundant secondary messengers in human cells, since they have a substantial diversity of roles in fundamental cellular physiology. Accumulating evidence has demonstrated that intracellular calcium homeostasis is altered in cancer cells and that this alteration is involved in tumor initiation, angiogenesis, progression and metastasis. -

Exisulind, a Novel Proapoptotic Drug, Inhibits Rat Urinary Bladder Tumorigenesis1
[CANCER RESEARCH 61, 3961–3968, May 15, 2001] Exisulind, a Novel Proapoptotic Drug, Inhibits Rat Urinary Bladder Tumorigenesis1 Gary A. Piazza, W. Joseph Thompson,2 Rifat Pamukcu, Hector W. Alila, Clark M. Whitehead, Li Liu, John R. Fetter, William E. Gresh, Jr., Andres J. Klein-Szanto, Daniel R. Farnell, Isao Eto, and Clinton J. Grubbs Cell Pathways, Inc., Horsham, Pennsylvania 19044 [G. A. P., W. J. T., R. P., H. W. A., C. M. W., L. L., J. R. F., W. E. G.]; Fox Chase Cancer Center, Philadelphia, Pennsylvania 19111 [A. J. K.]; Southern Research Institute, Birmingham, Alabama 35205 [D. R. F.]; and The University of Alabama at Birmingham, Birmingham, Alabama 35205-7340 [I. E., C. J. G.] ABSTRACT systemic or intravesical delivery of chemotherapeutic drugs, which produce relatively modest efficacy and are associated with serious Exisulind (Aptosyn) is a novel antineoplastic drug being developed for side effects and/or delivery complications. The high rate of mortality the prevention and treatment of precancerous and malignant diseases. In from urinary bladder cancer and the high incidence of disease recur- colon tumor cells, the drug induces apoptosis by a mechanism involving cyclic GMP (cGMP) phosphodiesterase inhibition, sustained elevation of rence emphasize the need for new therapeutic agents alone or in cGMP, and protein kinase G activation. We studied the effect of exisulind combination with existing therapies. Research to identify the specific on bladder tumorigenesis induced in rats by the carcinogen, N-butyl-N- molecular defects involved in bladder tumorigenesis has identified (4-hydroxybutyl) nitrosamine. Exisulind at doses of 800, 1000, and 1200 mutations in a number of genes (i.e., ras and p53) or altered expres- mg/kg (diet) inhibited tumor multiplicity by 36, 47, and 64% and tumor sion of proteins (cyclin D and p21 WAF1/CIP1), which are known to incidence by 31, 38, and 61%, respectively. -
Nitrosamines EMEA-H-A5(3)-1490
25 June 2020 EMA/369136/2020 Committee for Medicinal Products for Human Use (CHMP) Assessment report Procedure under Article 5(3) of Regulation EC (No) 726/2004 Nitrosamine impurities in human medicinal products Procedure number: EMEA/H/A-5(3)/1490 Note: Assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union © European Medicines Agency, 2020. Reproduction is authorised provided the source is acknowledged. Table of contents Table of contents ...................................................................................... 2 1. Information on the procedure ............................................................... 7 2. Scientific discussion .............................................................................. 7 2.1. Introduction......................................................................................................... 7 2.2. Quality and safety aspects ..................................................................................... 7 2.2.1. Root causes for presence of N-nitrosamines in medicinal products and measures to mitigate them............................................................................................................. 8 2.2.2. Presence and formation of N-nitrosamines -

Aspartame—True Or False? Narrative Review of Safety Analysis of General Use in Products
nutrients Review Aspartame—True or False? Narrative Review of Safety Analysis of General Use in Products Kamila Czarnecka 1,2,*, Aleksandra Pilarz 1, Aleksandra Rogut 1, Patryk Maj 1, Joanna Szyma ´nska 1, Łukasz Olejnik 1 and Paweł Szyma ´nski 1,2,* 1 Department of Pharmaceutical Chemistry, Drug Analyses and Radiopharmacy, Faculty of Pharmacy, Medical University of Lodz, Muszy´nskiego1, 90-151 Lodz, Poland; [email protected] (A.P.); [email protected] (A.R.); [email protected] (P.M.); [email protected] (J.S.); [email protected] (Ł.O.) 2 Department of Radiobiology and Radiation Protection, Military Institute of Hygiene and Epidemiology, 4 Kozielska St., 01-163 Warsaw, Poland * Correspondence: [email protected] (K.C.); [email protected] (P.S.); Tel.: +48-42-677-92-53 (K.C. & P.S.) Abstract: Aspartame is a sweetener introduced to replace the commonly used sucrose. It was discovered by James M. Schlatter in 1965. Being 180–200 times sweeter than sucrose, its intake was expected to reduce obesity rates in developing countries and help those struggling with diabetes. It is mainly used as a sweetener for soft drinks, confectionery, and medicines. Despite its widespread use, its safety remains controversial. This narrative review investigates the existing literature on the use of aspartame and its possible effects on the human body to refine current knowledge. Taking to account that aspartame is a widely used artificial sweetener, it seems appropriate to continue Citation: Czarnecka, K.; Pilarz, A.; research on safety. Studies mentioned in this article have produced very interesting results overall, Rogut, A.; Maj, P.; Szyma´nska,J.; the current review highlights the social problem of providing visible and detailed information about Olejnik, Ł.; Szyma´nski,P. -

(LC-HRMS) Method for the Determination of Six Nitrosamine Impurities in ARB Drugs
05/21/2019 Liquid Chromatography-High Resolution Mass Spectrometry (LC-HRMS) Method for the Determination of Six Nitrosamine Impurities in ARB Drugs Background: Angiotensin II receptor blocker (ARB) drug products are commonly used to treat high blood pressure and heart failure. In July 2018, it was found that some ARB drug products contained carcinogenic nitrosamine impurities. As this incident continues to evolve, it has resulted in numerous recalls and ARB drug shortages in the US. As a member of the FDA’s working group to address this continually-evolving incident, CDER/OPQ/OTR is responsible for testing for nitrosamine impurities in ARB drug products and drug substances of interest. OTR has successfully developed and implemented GC/MS methods to quantitate N- nitrosodimethylamine (NDMA) and N-nitrosodiethylamine (NDEA) at trace levels. However, these GC/MS methods cannot yet directly detect N-nitroso-N-methyl-4-aminobutyric acid (NMBA), another nitrosamine impurity that was found in certain ARB drug products by some firms. In addition, it is speculated that three other nitrosamine impurities may also be present in ARB drugs from reviews of manufacturing processes and published literature sources, namely N-nitrosoethylisopropylamine (NEIPA), N-nitrosodiisopropylamine (NDIPA), and N- nitrosodibutylamine (NDBA). Thus, a single method was developed that was capable of detecting and quantifying all of the six aforementioned impurities simultaneously. Herein, we report an LC-HRMS method that has been validated for the simultaneous determination of the six nitrosamine impurities in losartan drug substance and drug product at sub-ppm levels. The method may also be capable of testing for these six impurities in other ARB drug substances and drug products pending verification and/or validation. -

Drug Information Center Highlights of FDA Activities – 1/1/21
Drug Information Center Highlights of FDA Activities – 1/1/21 – 1/31/21 FDA Drug Safety Communications & Drug Information Updates: Risk of False Results with the Curative SARS‐Cov‐2 Test for COVID‐19 1/7/2021 The Curative SARS‐Cov‐2 test is real‐time RT‐PCR test used to detect SARS‐Cov‐2. There are concerns that the test may yield false negatives. To reduce the risk of false negatives. Ensure that testing is done in accordance with the authorized labeling. Providers should consider retesting patients by using a different test if an inaccurate result is suspected. Health professionals and patients are encouraged to report problems with test performance or results to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program. Vinca Alkaloid Labeling for Preparation in Intravenous Infusion Bags Only 1/15/21 The FDA alerted health care professionals to labeling updates for the preparation of vinca alkaloids including vincristine sulfate injection, vinblastine sulfate for injection, and vinorelbine tartrate injection. To avoid unintended intrathecal administration, labeling is being updated to remove instructions for preparation of these products in a syringe and to recommend preparation in intravenous infusion bags only. Import Alert – All Alcohol‐Based Hand Sanitizers from Mexico 1/26/21 The FDA has placed all alcohol‐based hand sanitizers from Mexico on an import alert to prevent products contaminated with methanol from reaching the market. Inspections will determine if products have been manufactured according to U.S. current good manufacturing practice requirements before allowing entry. Misbranded Active Pharmaceutical Ingredients – Drug Information Update 1/28/21 The FDA issued a warning to Professional Compounding Centers of America (PCCA) for receiving and distributing misbranded active pharmaceutical ingredients. -

Example of How Amehsi Specification Indicators Can Be Mapped to Health
Example of how Amehsi Specification Indicators can be Mapped to Health Conditions and Health Statuses The information presented here may be covered by copyrights and patents Some of the Amehsi Factors which can be alleviated using Amehsi Specification Recommendations and Demise Oncology Leukemia Lymphoma HIV Information. This document may be protected by copyrights and patents Choline Deficiency or Circumstantial Choline Deficiency from upregulated Choline Kinase Pathway or Kennedy Pathway Factors Causal Causal Causal Causal Causal Homocysteine Required as Symptom, Correlated and Incipiently Causal, inhibits PEMT Required Causal Causal Causal S-Adenosyl Homocysteine Downregulat Required as Symptom, Correlated and Incipiently Causal, inhibits PEMT Required Causal ed PEMT Causal Trimethylamine-N-Oxide Causal, inhibits PEMT Causal Causal Causal Incipient Enabler Choline Kinase Upregulation Causal Required Required uNOS Required Required as both PEMT1 or PEMT2 since Diagnostic Assay sometimes does not report if one of these is inhibited while the other is not. PEMT produces a Monomethylethanolamine that Phosphatidylethanolamine deteriorates PCBs, Dioxins, Aryl Methyltransferase Downregulation Cyclic Hydrocarbons, Alkyl Halides, other Carcinogens and produces Serine Proteases that catabolize Amino acids to thier most basic structures, resulting in purified cellular environment and embryonic Causal cellular plasticity Required Required Required Inducible Nitric Oxide Synthase, Required, inhibits PEMT and upregulated Choline kinase, as well as -

Profile of Michael A. Marletta
PROFILE Profile of Michael A. Marletta or more than three decades, largely in water, largely at a pH of 7.5, Michael Marletta has traveled and mostly at 37 degrees Celsius. Chem- a serpentine road, working to elu- ists would consider those conditions F ” cidate a molecule whose impor- about the worst to work with, he says. tance to human physiology is as well Marletta’s research during the next three recognized as his own contributions to his decades focused on the interface between field. Named “Molecule of the Year” in chemistry and biology. 1992 by Science, nitric oxide, a noxious Because of this work, he refuses to be atmospheric gas, plays a pivotal role in typecast. “At one time in my career, I biological functions as diverse as forming called myself a biochemist. Now, I call long-term memory and maintaining penile myself a chemical biologist, but I continue erections (1). Marletta, who was elected to do what I’ve always done—enzymol- to the National Academy of Sciences in ogy,” he says. 2006, has shed light on the biochemistry of When it came time to pick a Ph.D. nitric oxide and the cellular machinery program, Marletta was faced with a dearth through which the molecule performs of choices because there were not many its functions. chemistry departments during the early Marletta’s work on nitric oxide not only 1970s that were serious about biology. led to a fundamental understanding of However, a fortuitous tip from a professor enzyme reaction mechanisms, but it has at Fredonia, who had heard about a pro- informed the development of treatments. -
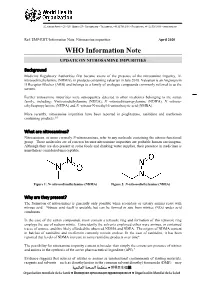
WHO Information Note UPDATE on NITROSAMINE IMPURITIES
20, AVENUE APPIA – CH-1211 GENEVA 27 – SWITZERLAND – TEL CENTRAL +41 22 791 2111 – FAX CENTRAL +41 22 791 3111 – WWW.WHO.INT Ref. EMP/RHT/Information Note_Nitrosamine impurities April 2020 WHO Information Note UPDATE ON NITROSAMINE IMPURITIES Background Medicine Regulatory Authorities first became aware of the presence of the nitrosamine impurity, N• nitrosodimethylamine (NDMA), in products containing valsartan in July 2018. Valsartan is an Angiotensin II Receptor Blocker (ARB) and belongs to a family of analogue compounds commonly referred to as the sartans. Further nitrosamine impurities were subsequently detected in other medicines belonging to the sartan family, including: N-nitrosodiethylamine (NDEA), N -nitrosodiisopropylamine (NDIPA), N -nitroso- ethylisopropylamine (NEIPA) and N -nitroso-N-methyl-4-aminobutyric acid (NMBA). More recently, nitrosamine impurities have been reported in pioglitazone, ranitidine and metformin containing products.1-5 What are nitrosamines? Nitrosamines, or more correctly N-nitrosoamines, refer to any molecule containing the nitroso functional group. These molecules are of concern because nitrosamine impurities are probable human carcinogens. Although they are also present in some foods and drinking water supplies, their presence in medicines is nonetheless considered unacceptable. Figure 1: N• nitrosodimethylamine (NDMA) Figure 2: N-nitrosodiethylamine (NDEA) Why are they present? The formation of nitrosamines is generally only possible when secondary or tertiary amines react with nitrous acid. Nitrous acid itself is unstable but can be formed in situ from nitrites (NO2) under acid conditions. In the case of the sartan compounds, most contain a tetrazole ring and formation of this tetrazole ring employs the use of sodium nitrite. Coincidently the solvents employed either were amines, or contained traces of amines, and this likely afforded the observed NDMA and NDEA. -

Retalac, Nitrosamines
To whom it may concern Dr. Stefan Dreiheller Quality Unit / Regulatory Affairs Date of issue: 31.03.2021 Page 1/3 Doc.-No. EIP-5036 Revision 5 Nitrosamines EMA/369136/2020; FDA Guidance for Industry „Control of Nitrosamine Impurities in Human Drugs“ MEGGLE Product: RetaLac® The formation of potent genotoxic nitrosamines as impurities is possible in the presence of secondary, tertiary, or quaternary amines and nitrite salts under acidic reaction conditions. Regarding the requests of EMA-CHMP and FDA-CDER that marketing authorisation holders for human medicines containing chemically synthesised active substances have to evaluate the risk for the possible presence of nitrosamines (e.g. NDMA, NDEA, NMBA, NMPA, NIPEA, NDIPA), a risk evaluation was conducted for the MEGGLE product to support the marketing authorisation holders. This evaluation (page 2 and 3) is based on the IPEC Questionnaire. The product is a co-processed, directly compressible spray agglomerate comprising 50 % Lactose Monohydrate (Ph. Eur. / USP-NF / JP) and 50 % Hypromellose (Ph. Eur. / USP-NF / JP). The compound lactose monohydrate produced at MEGGLE is not chemically synthesized. Organic solvents, catalysts and other reagents which might be a reason for the presence of secondary, tertiary, or quaternary amines and nitrite salts are not used. Furthermore, acidic conditions as necessary prerequisite for the formation of nitrosamines are not achieved during manufacturing process. Lactose monohydrate is isolated and purified from whey which is a by-product of cheese manufacturing. Whey does not contain relevant amounts of nitrates (as precursor of nitrites) and nitrites. Testing on nitrates and nitrites is conducted as part of incoming goods inspection.