Jyotiba Phule Nagar 2018.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Geoenvironmental Study of Alluvial Aquifer in Upper Gangetic Plain, a Case Study of J P Nagar, Uttar Pradesh, India
IOSR Journal of Environmental Science, Toxicology and Food Technology (IOSR-JESTFT) e-ISSN: 2319-2402,p- ISSN: 2319-2399.Volume 8, Issue 5 Ver. IV (May. 2014), PP 56-67 www.iosrjournals.org Geoenvironmental study of alluvial aquifer in Upper Gangetic plain, a case study of J P Nagar, Uttar Pradesh, India 1 1 1 1 Vikas Kamal , Saumitra Mukherjee , Deepika Srivastava , Naba Hazarika and Neha Singh1 1(School of Environmental Sciences, Jawaharlal Nehru University, New Delhi-110067, India) Abstract: Water quality is very important if we take into account the human paradigm in the environment. Groundwater constitutes the 30.1% of the freshwater reserves on earth. Gangetic plains in India have the highest density of groundwater extraction structures. 50 samples were taken in total from J P Nagar district of which there were 3 river water samples and 6 were groundwater samples falling just outside the district boundary. Using statistical and GIS analysis various indices were calculated. WQI or water quality index revealed a zone of high pollution across the district. Hydrochemical plots like Piper, Durov and Chaddha diagram brought out the information about the water type in the area. Mineralogy of the study area shows the dominance of feldspar minerals. Land cover change between 1998 and 2013 has been deciphered from supervised classification of Landsat data of USGS. Keywords: Ganga plain, J P Nagar, groundwater, interfluve, hydrochemical facies, stability diagram I. Introduction Groundwater reserves of the Ganga plain are so huge that even the GRACE (Gravity Recovery and Climate Experiment) satellite could detect it from hundreds of kilometres away. -

List of Class Wise Ulbs of Uttar Pradesh
List of Class wise ULBs of Uttar Pradesh Classification Nos. Name of Town I Class 50 Moradabad, Meerut, Ghazia bad, Aligarh, Agra, Bareilly , Lucknow , Kanpur , Jhansi, Allahabad , (100,000 & above Population) Gorakhpur & Varanasi (all Nagar Nigam) Saharanpur, Muzaffarnagar, Sambhal, Chandausi, Rampur, Amroha, Hapur, Modinagar, Loni, Bulandshahr , Hathras, Mathura, Firozabad, Etah, Badaun, Pilibhit, Shahjahanpur, Lakhimpur, Sitapur, Hardoi , Unnao, Raebareli, Farrukkhabad, Etawah, Orai, Lalitpur, Banda, Fatehpur, Faizabad, Sultanpur, Bahraich, Gonda, Basti , Deoria, Maunath Bhanjan, Ballia, Jaunpur & Mirzapur (all Nagar Palika Parishad) II Class 56 Deoband, Gangoh, Shamli, Kairana, Khatauli, Kiratpur, Chandpur, Najibabad, Bijnor, Nagina, Sherkot, (50,000 - 99,999 Population) Hasanpur, Mawana, Baraut, Muradnagar, Pilkhuwa, Dadri, Sikandrabad, Jahangirabad, Khurja, Vrindavan, Sikohabad,Tundla, Kasganj, Mainpuri, Sahaswan, Ujhani, Beheri, Faridpur, Bisalpur, Tilhar, Gola Gokarannath, Laharpur, Shahabad, Gangaghat, Kannauj, Chhibramau, Auraiya, Konch, Jalaun, Mauranipur, Rath, Mahoba, Pratapgarh, Nawabganj, Tanda, Nanpara, Balrampur, Mubarakpur, Azamgarh, Ghazipur, Mughalsarai & Bhadohi (all Nagar Palika Parishad) Obra, Renukoot & Pipri (all Nagar Panchayat) III Class 167 Nakur, Kandhla, Afzalgarh, Seohara, Dhampur, Nehtaur, Noorpur, Thakurdwara, Bilari, Bahjoi, Tanda, Bilaspur, (20,000 - 49,999 Population) Suar, Milak, Bachhraon, Dhanaura, Sardhana, Bagpat, Garmukteshwer, Anupshahar, Gulathi, Siana, Dibai, Shikarpur, Atrauli, Khair, Sikandra -

Amroha District, Uttar Pradesh
Central Ground Water Board AQUIFER MAPPING AND MANAGEMENT OF GROUND WATER RESOURCES AMROHA DISTRICT, UTTAR PRADESH REPORT ON AQUIFER MAPPING AND GROUND WATER MANAGEMENT PLAN IN AMROHA DISTRICT, UTTAR PRADESH (AAP: 2017-18) CONTENTS Chapter Title Page No. No. AMROHA DISTRICT AT A GLANCE 1 INTRODUCTION 1 2 DATA COLLECTION AND GENERATION 11 3 HYDROGEOLOGY 16 4 GROUND WATER RESOURCES 19 5 GROUND WATER MANAGEMENT IN SC AMROHA BLOCK 28 6 GROUND WATER MANAGEMENT IN OE JOYA BLOCK 36 7 GROUND WATER MANAGEMENT IN OE DHANAURA BLOCK 44 8 GROUND WATER MANAGEMENT IN OE GAJRAULA BLOCK 52 9 GROUND WATER MANAGEMENT IN OE HASANPUR BLOCK 60 10 GROUND WATER MANAGEMENT IN SC GANGESHWARI BLOCK 68 11 CONCLUSION 76 12 RECOMMENDATIONS 78 13 ACKNOWLEDGEMENTS LIST OF TABLES: 1. Details of the Cropping Pattern, Amroha District, U.P. 2. Details of Area under Different Crops, Amroha District, U.P. 3. Details of the distribution of Surface and Ground Water for Irrigation, Amroha District, U.P. 4. Water Level Data of GWMW’s of Amroha District, U.P. 5. Data availability of exploration wells in Amroha District, U.P. 6. Result of chemical analysis of water sample from GWOW in Amroha District, U.P. 7. Result of heavy metal analysis of water sample from GWOW in Amroha District, U.P. 8. Summary of exploration and hydraulic details in Amroha District, U.P. 9. Aquifer details in Amroha District, U.P. 10. Dynamic Ground Water Resources and Development Potential (as on 31.03.2017) in Amroha District, U.P. 11. Block-Wise In-Storage Ground Water Resources of Fresh Water in Unconfined Aquifer in Amroha District, U.P. -

Bhs&Ie, up Exam Year-2021 **** Final Centre Allotment
DATE:27-02-2021 BHS&IE, UP EXAM YEAR-2021 **** FINAL CENTRE ALLOTMENT REPORT **** DIST-CD & NAME :- 22 AMROHA PAGE:- 1 CENT-CODE & NAME EXAM SCH-STATUS SCHOOL CODE & NAME #SCHOOL-ALLOT SEX PART GROUP 1001 GOVT INTER COLLEGE AMROHA AUM HIGH BUF 1018 S D K I C AMROHA 75 F HIGH CRM 1035 JANTA H S S TAKHATPUR AMROHA 18 M HIGH CUM 1038 S R P I C AMROHA 11 F HIGH CUM 1085 MATLOOB M I C AMROHA AMROHA 3 F HIGH CUM 1094 H P I C AMROHA 20 F HIGH CUM 1102 NABI AHMAD MUSLIM INTER COLLEGE AMROHA 11 F HIGH CUM 1114 DR BR AMBEDKAR H S S AMROHA 21 F HIGH CUM 1131 RAM CHARAN SINGH B V M HIGH SCHOOL JOYA AMROHA 2 M HIGH CUM 1136 NEHRU CHILDREN H S S AMROHA 26 F HIGH CUM 1137 HASNAIN H S S AMROHA 6 F HIGH CUM 1146 SAIFI HIGH SCHOOL AMROHA 21 F HIGH CUF 1148 M Q M GIRLS H S S AMROHA 66 F HIGH CUM 1155 A R MUSLIM H S S AMROHA 4 F HIGH CUM 1189 SAKSHI DEVI I C AMROHA 23 F 307 INTER AUM 1001 GOVT INTER COLLEGE AMROHA 2 F SCIENCE INTER BUM 1005 A K K I C AMROHA 49 M OTHER THAN SCICNCE INTER BRM 1025 AKG I C JALALPUR DHANA AMROHA 25 M OTHER THAN SCICNCE INTER BRM 1025 AKG I C JALALPUR DHANA AMROHA 37 M SCIENCE INTER BRM 1031 K I C KOTHI KHIDMATPUR AMROHA 35 M ALL GROUP INTER CRM 1071 A S M BAL V M I C KHATA AMROHA 46 M OTHER THAN SCICNCE INTER CRM 1071 A S M BAL V M I C KHATA AMROHA 135 M SCIENCE 329 CENTRE TOTAL >>>>>> 636 1002 J S HINDU INTER COLLEGE AMROHA BUM HIGH BUM 1002 J S HINDU INTER COLLEGE AMROHA 62 F HIGH BUM 1005 A K K I C AMROHA 142 M HIGH BRM 1007 R I C JABDA AMROHA 103 M HIGH BRM 1025 AKG I C JALALPUR DHANA AMROHA 75 M HIGH CUM 1038 S R P I C -

Gajraula Town Is Situated on NH-24, Between Delhi and Moradabad City
AACCTTIIOONN PPLLAANN FFOORR TTHHEE CCOONNTTRROOLL OOFF AAIIRR PPOOLLLLUUTTIIOONN IINN GGAAJJRRAAUULLAA CCIITTYY RREEGGIIOONNAALL OOFFFFIICCEE UUTTTTAARR PPRRAADDEESSHH PPOOLLLLUUTTIIOONN CCOONNTTRROOLL BBOOAARRDD 110088//1111,,, AAVVAASS VVIIKKAASS CCOOLLOONNYY,,, BBIIJJNNOORR 1. INTRODUCTION Gajraula Town is situated on NH-24, between Delhi and Moradabad city. Gajraula is a main Industrial town of District – Amroha (J.P. Nagar). Gajraula is a Small city/ Town but known as a Developed Town due to its, Location, Rail and Road connectivity and Industrial activity. Most of The Nearby area is well developed forming area and dairy Milk producing area as well as good forming of sugarcane also. Local drain/River Bagad is the main Rainy drain which carry the storm water and industrial treated waste water and ultimately meet to River Ganga. Gajraula has a humid subtropical climate with cool, dry winter form mid November to February and dry hot summer from late March to June. Due to local sugar crop growing and Ganga River bed December January is mostly full of Fog weather. Gajraula Town is under limit of Nagar Palika Parishad Gajraula. It is an important industrial area of Uttar Pradesh. Ambient air quality monitoring in Gajraula Town is carried out by UPPCB on out sourcing basis at two location (i) Raunak Automotive Ltd, U.P.S.I.D.C. industrial area and (ii) Indira Chowk, Gajraula. Ambient air quality monitoring is carried out at above two main location of this town. The ambient air quality (PM 10 ) is increasing periodically due to development of industrial, commercial and residential activities in this area. Besides this NHAI work for 06 lining of NH-24 is also in progress and dust emission is prominent due to this activity. -

District Name: Amroha
District Name: Amroha District Name: Amroha DISTRICT Amroha NAME STATE Uttar Pradesh YEAR 2020-21 As – Is Scenario Aggregate Demand • Map the District Map the Primary Demand • Topography Agriculture – Major Crops • Climate Animal Husbandry • Economic Profile Horticulture • Literacy Poultry • Population Others • Identify the Target Population Producer Groups/ SHG Base Map the Secondary Demand • Population of District Major manufacturing clusters • Rural Urban Products/ Trade • Gender • Large Towns/ Villages Map the Service/ Tertiary • Map the Infra Sector • Skill Training Centers Retail across schemes and Tourism departments long and Others short term Map the Traditional Arts and • Current Courses and Crafts performance (E/T/P) SHG Map emerging sectors IT … Self-Employment opportunity Analyse the Gap Action Plan What’s the SWOT for the • Develop Execution plan district (skill and livelihood • Baseline data ecosystem perspective) ? • What are we trying to achieve What are the Demand Supply through this activity(physical and Gaps – aggregate and block other targets) level? • Target audience/beneficiary Migration – Inward and Identify Sectors roles and Outward? courses Knowledge Partners TPs Budget and other resources Develop monitoring and evaluation plan& templates Perceived risks and mitigation strategies 2 District Name: Amroha District Information:- District Name: Amroha District Amroha lies in the west of Moradabad District adjoining district Hapur, Sambhal & Buland Shahar,Bijnor. The district came into being on 15th April 1997 in the memory of famous social reformer Sant Mahatama Jyotiba Phule by combining Amroha, Dhanora & Hasanpur Tehsils of Moradabad district vide UP Gazette no. 1071/1-5-97/224/sa-5 dated 15th April 1997 whose headoffice is situated in the ancient city Amroha. -
Bareilly Zone CSC List
S Grampanchayat N District Block Name Village/CSC name Pincode Location VLE Name Contact No Village Name o Badaun Budaun2 Kisrua 243601 Village KISRUA Shailendra Singh 5835005612 Badaun Gunnor Babrala 243751 Babrala Ajit Singh Yadav Babrala 5836237097 Badaun Budaun1 shahavajpur 243638 shahavajpur Jay Kishan shahavajpur 7037970292 Badaun Ujhani Nausera 243601 Rural Mukul Maurya 7351054741 Badaun Budaun Dataganj 243631 VILLEGE MARORI Ajeet Kumar Marauri 7351070370 Badaun Budaun2 qadarchowk(R) 243637 qadarchowk sifate ali qadarchowk 7351147786 Badaun Budaun1 Bisauli 243632 dhanupura Amir Khan Dhanupura 7409212060 Badaun Budaun shri narayanganj 243639 mohalla shri narayanganj Ashok Kumar Gupta shri narayanganj 7417290516 Badaun BUDAUN1 Ujhani(U) 243639 NARAYANGANJ SHOBHIT AGRAWAL NARAYANGANJ 7417721016 Badaun BUDAUN1 Ujhani(U) 243639 NARAYANGANJ SHOBHIT AGRAWAL NARAYANGANJ 7417721016 Badaun BUDAUN1 Ujhani(U) 243639 BILSI ROAD PRADEEP MISHRA AHIRTOLA 7417782205 Badaun Vazeerganj Wazirganj (NP) 202526 Wazirganj YASH PAL 7499478130 Badaun Dahgawan Nadha 202523 Nadha Mayank Kumar 7500006864 Badaun Budaun2 Bichpuri 243631 VILL AND POST MIAUN Atul Kumar 7500379752 Badaun Budaun Ushait 243641 NEAR IDEA TOWER DHRUV Ushait 7500401211 Badaun BUDAUN1 Ujhani(R) 243601 Chandau AMBRISH KUMAR Chandau 7500766387 Badaun Dahgawan DANDARA 243638 DANDARA KULDEEP SINGH DANDARA 7534890000 Badaun Budaun Ujhani(R) 243601 KURAU YOGESH KUMAR SINGH Kurau 7535079775 Badaun Budaun2 Udhaiti Patti Sharki 202524 Bilsi Sandeep Kumar ShankhdharUGHAITI PATTI SHARKI 7535868001 -

Udyog Aadhaar Registration Certificate
Type of Enterprise Micro Small Medium Manufacturing A B C C Services D E F UAN UP40B0000032 Udyog Aadhaar Registration Certificate Udyog Aadhaar Number UP40B0000032 Name of Enterprise NOREX FLAVOURS PRIVATE LIMITED Location of Plant Details Name of Premises/Building SN Flat/Door/Block No. Road/Street/ Lane Area/Locality City Pin State District Village OPP. ROADWAYS NOREX FLAVOURS PRIVATE GAJRAULA CHANDPUR MANDI UTTAR AMROHA(JYOTIBA PHULE 1 DHANAURA 244231 BUS ST LIMITED ROAD DHANAURA PRADESH NAGAR) NOREX FLAVOURS PRIVATE MANDI UTTAR AMROHA(JYOTIBA PHULE 2 AMROHA ROAD MANDI DHANAURA DHANAURA 244231 LIMITED DHANAURA PRADESH NAGAR) Official Address of Enterprise OPP. ROADWAYS BUS STAND, GAJRAULA CHANDPUR ROAD, MANDI DHANAURA 244231 DISTT AMROHA District AMROHA(JYOTIBA PHULE NAGAR) State UTTAR PRADESH PIN 244231 Mobile No: 9897036570 Email: [email protected] Date of commencement 07/03/2009 Major Activity MANUFACTURING Enterprise Type Medium Previous Registration details-if any EM-2 :: 090061100472 National Industry Classification Code SN NIC 2 Digit NIC 4 Digit NIC 5 Digit Code Activity Type 21 - Manufacture of pharmaceuticals, 2100 - Manufacture of pharmaceuticals, 21009 - Manufacture of other pharmaceutical and botanical 1 medicinal chemical and botanical Manufacturing medicinal chemical and botanical products products n.e.c. like hina powder etc. products 2 32 - Other manufacturing 3290 - Other manufacturing n.e.c. 32909 - Manufacture of other articles n.e.c. Manufacturing 20 - Manufacture of chemicals and 2029 - Manufacture of other chemical 20293 - Manufacture of essential oils; modification by chemical 3 Manufacturing chemical products products n.e.c. processes of oils and fats (e.g. by oxidation, polymerization etc.) Acknowledgement Date of Filing 19/12/2015 Date of Printing 20/04/2018 Disclaimer: This is computer generated statement, no signature required. -

CP Vol IX RAP
Uttar Pradesh Core Road Network Development Program DETAILED PROJECT REPORT Volume – IX: Resettlement Action Plan Badaun – Bilsi – Bijnaour Road (SH-51) 0 EXECUTIVE SUMMARY 0.1 Introduction The state has a road network of 299,604 km, out of which 174,451 km is under Uttar Pradesh Public Works Department (PWD). The roads under PWD comprise 7,550 km of National Highways (NHs), 7,530 km of State Highways (SHs), 5,761 km of Major District Roads (MDRs), 3,254 km of Other District Roads (ODRs) and 138,702 km of Village Roads (VRs). Only about 60% of SHs are two-lane (7 m). In the entire state 62% of MDRs and 83% of ODRs have widths less than 7 m. With a view to improve the transport network system, UP PWD has identified 24,095 km of Core Road Network (CRN) for the development. The Core road development works will consist of raising the formation level, widening to a full two lanes from the existing single and intermediate lane widths, and/or pavement rehabilitation/strengthening. Road sections with high volumes of non-motorized traffic will be widened to 10m with 1.5m full paved shoulders. Road stretches crossing urban areas may also require upgrading to a four lane cross section, and/or provision for drains, sidewalks and parking where required. In some cases, new alignments (by-passes and/or re-alignments may also be required. In view of the above, UP core road network development project (UPCRNDP) has been designed. The UPCRNDP will have three Components: Upgrading/reconstruction/widening as well as rehabilitation of selected roads from the Core Road Network (CRN) including construction of a new Sharda Bridge at Pachpheri Ghat in Lakhimpur district. -
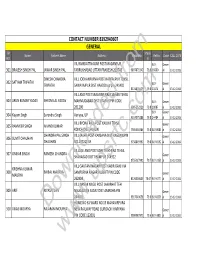
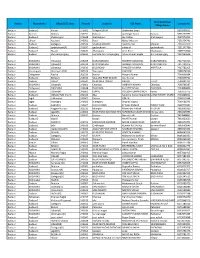
CONTACT NUMBER 8392940607 GENERAL SR Marks Name Father's Name Address Mobileno Refno
CONTACT NUMBER 8392940607 GENERAL SR Marks Name Father's Name Address MobileNo RefNo. Caste CALL DATE NO. % VIL RAMDATTNAGAR POST MADANPUR BLY- Gener 301 BRAJESH SINGH PAL JAWAR SINGH PAL FARRUKHABAD UTTAR PRADESH 209743 9897871342 79.8 16600 al 13-12-2018 DINESH CHANDRA VILL JODHANPURVA POST HARPALPUR TEHSIL 302 SATYAM TRIPATHI TRIPATHI SAWAYAJPUR DIST HARDOI up pin 241402 BLY- Gener from8174876425 79.8 11674 al 13-12-2018 VILL AND POST SARAIYAN RAJA SAHAB TEHSIL 303 ARUN KUMAR YADAV SHYAM LAL YADAV MAHMUDABAD DIST SITAPUR PIN CODE BLY- Gener 261206 9005252321 79.8 10087 al 13-12-2018 BLY- Gener 304 Kayam Singh Surendra Singh Auriyya, UP 9557075288 79.8 14484 al 13-12-2018 VILL BYONA RAJA POST KAILIYA TEHSIL 305 RAMVEER SINGH ANAND KUMAR Gener KONCH DIST JALAUN 7905366386 79.8 BLY-8086 al 13-12-2018 CHANDRA PAL SINGH VILL-JAKHA POST-KARSANA DIST-KASGANJPIN 306 SUMIT CHAUHAN Gener CHAUHAN NO.207241 UP 9758849397 79.8 BLY-6592 al 13-12-2018 VILLAGE AND POST KARETHI KHERA TEHSIL 307 OMKAR SINGH RAMESH CHANDRA SHAHABAD DISTT RAMPUR 244922 Gener 8755327990 79.7 BLY-2351 al 13-12-2018 VILL GAUTAM NAGAR POST KABIR GANJ VIA KRISHNA KUMAR 308 BIRBAL MAURYA SAMPURNA NAGAR PILIBHIT PIN CODE MAURYA Gener 262904 8126903654 79.67 BLY-6777 al 13-12-2018 VILL NANAK NAGLI POST LAKARHAT TEH 309 ARIF RIYASAT JAN NAUGAWAN SADAT DIST AMROHA PIN Gener 244501 9917949658 79.6 BLY-8256 al 13-12-2018 HOME NO 61 WARD NO 15 MAHAVIRPURA 310 VIKAS MOURYA RAJARAMDownloaded MOURYA NEW RAILWAY ROAD GURGAON HARYANA Gener PIN CODE 122001 9990087870 79.6 BLY-3815 al 13-12-2018 -

Comparison of Categorization of Assessment Units (2020 and 2017) State: Uttar Pradesh
COMPARISON OF CATEGORIZATION OF ASSESSMENT UNITS (2020 AND 2017) STATE: UTTAR PRADESH Stage of Stage of Ground Ground Name of Assessment Categorization Name of Assessment Categorization in S. No Name of District Water Name of District Water Remark Unit (Block) in 2017 Unit (Block) 2020 Extraction Extraction (%) (%) in 2017 in 2020 1 2 3 4 5 6 7 8 9 10 LIST OF DISTRICTS AND BLOCKS WHOES CATEGORY IMPROVED FROM 2017 TO 2020 1 AMBEDKAR NAGAR BASKHARI 74.00 Semi-Critical AMBEDKAR NAGAR BASKHARI 67.83 Safe Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 2 AMBEDKAR NAGAR BHITI 89.09 Semi-Critical AMBEDKAR NAGAR BHITI 68.48 Safe Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 3 AMBEDKAR NAGAR JAHANGIRGANI 89.81 Semi-Critical AMBEDKAR NAGAR JAHANGIRGANI 57.61 Safe Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 4 AMBEDKAR NAGAR KATEHARI 74.03 Semi-Critical AMBEDKAR NAGAR KATEHARI 61.50 Safe Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 5 AMROHA DHANAURA 104.43 Over Exploited AMROHA DHANAURA 97.09 Critical Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 6 AMROHA GAJRAULA 110.42 Over Exploited AMROHA GAJRAULA 98.04 Critical Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 7 AMROHA HASANPUR 111.60 Over Exploited AMROHA HASANPUR 92.35 Critical Extraction for irrigation reduced asper MI Cencus, WL raised subsequently 8 BARABANKI BANI KODAR 80.40 Semi-Critical BARABANKI BANI KODAR 65.64 Safe Extraction -

World Bank Document
GOVERNMENT OF UTTAR PRADESH Public Works Department Public Disclosure Authorized Uttar Pradesh Core Road Network Development Program Part – A: Project Preparation DETAILED PROJECT REPORT Volume - VIII: Draft Environmental Impact Assessment Report and Environmental Management Plan Public Disclosure Authorized Badaun – Bilsi – Bijnaour Road (SH-51) Public Disclosure Authorized Public Disclosure Authorized December 2014 India Consulting engineers pvt. ltd. Uttar Pradesh Core Road Network Development Program DETAILED PROJECT REPORT Volume-VIII: Draft EIA and EMP Report Badaun – Bilsi – Bijnaour Road (SH-51) Volume-VIII : Draft Environmental Impact Assessment Report and Document Name Environmental Management Plan (Detailed Project Report) Document Number EIRH1UP020/DPR/SH-51/BBB/003/VIII Uttar Pradesh Core Road Network Development Program Project Name Part – A: Project Preparation including Detailed Engineering Design and Contract Documentation Project Number EIRH1UP020 Document Authentication Name Designation Prepared by Dr. S.S. Deepak Environmental Specialist Reviewed by Sudhendra Kumar Karanam Sr. General Manager (Roads & Highways) Rajeev Kumar Gupta Deputy Team Leader Avadesh Singh Technical Head Approved by Francisco Eucario Perez Team Leader History of Revisions Version Date Description of Change(s) Rev. 0 23/12/2014 First Submission Page i| Rev: R0 , Uttar Pradesh Core Road Network Development Program DETAILED PROJECT REPORT Volume-VIII: Draft EIA and EMP Report Badaun – Bilsi – Bijnaour Road (SH-51) TABLE OF CONTENTS Chapter Description