SRH) Into Disaster Risk Reduction (DRR) in Crisis-Affected Pakistan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PAKISTAN: FLOODS/RAINS 2012 Series No. 4 RAPID
Pakistan Floods / Rains 2012: Rapid Crop Damage Assessment: Series No. 4 PAKISTAN: FLOODS/RAINS 2012 Series No. 4 RAPID CROP DAMAGE ASSESSMENT October 30, 2012 Pakistan Space & Food and Agriculture Upper Atmosphere Organization of the Research Commission United Nations Pakistan Floods / Rains 2012: Rapid Crop Damage Assessment: Series No. 4 ISBN : 978-969-9102-11-0 Pakistan Space & Upper Atmosphere Research Commission SPARC, Islamabad Phone: 051-9273312, 051-4611792 e-mail:[email protected], Website: www.suparco.gov.pk Pakistan Floods / Rains 2012: Rapid Crop Damage Assessment: Series No. 4 Foreword Pakistan faced floods and tormenting rains during the last three consecutive monsoons from 2010 to 2012. During these floods, the ground communication systems were generally disrupted and information on flood extent and damage through ground reporting services was not available for taking timely decisions. To address the situation and to ensure continuous provision of current and timely information to the concerned stakeholder’s and decision makers satellite remote sensing and GIS technologies were extensively utilized. SUPARCO in collaboration with FAO started generating data on daily basis on flood extent, damage to households, infrastructure and crops besides undertaking detailed Damage Need Assessment (DNA). This fast track supply of information made it possible to reach out to affected and displaced masses for supply of food, medical care, relief, rehabilitation and follow up programs. In the aftermath of floods, monitoring of flood recession and ponding of water in the affected areas on decadal basis was also carried out for several months. All of this work was published by SUPARCO-FAO jointly in three reports (Reports 1 to 3). -

Population According to Religion, Tables-6, Pakistan
-No. 32A 11 I I ! I , 1 --.. ".._" I l <t I If _:ENSUS OF RAKISTAN, 1951 ( 1 - - I O .PUlA'TION ACC<!>R'DING TO RELIGIO ~ (TA~LE; 6)/ \ 1 \ \ ,I tin N~.2 1 • t ~ ~ I, . : - f I ~ (bFICE OF THE ~ENSU) ' COMMISSIO ~ ER; .1 :VERNMENT OF PAKISTAN, l .. October 1951 - ~........-.~ .1',l 1 RY OF THE INTERIOR, PI'ice Rs. 2 ~f 5. it '7 J . CH I. ~ CE.N TABLE 6.-RELIGION SECTION 6·1.-PAKISTAN Thousand personc:. ,Prorinces and States Total Muslim Caste Sch~duled Christian Others (Note 1) Hindu Caste Hindu ~ --- (l b c d e f g _-'--- --- ---- KISTAN 7,56,36 6,49,59 43,49 54,21 5,41 3,66 ;:histan and States 11,54 11,37 12 ] 4 listricts 6,02 5,94 3 1 4 States 5,52 5,43 9 ,: Bengal 4,19,32 3,22,27 41,87 50,52 1,07 3,59 aeral Capital Area, 11,23 10,78 5 13 21 6 Karachi. ·W. F. P. and Tribal 58,65 58,58 1 2 4 Areas. Districts 32,23 32,17 " 4 Agencies (Tribal Areas) 26,42 26,41 aIIjab and BahawaJpur 2,06,37 2,02,01 3 30 4,03 State. Districts 1,88,15 1,83,93 2 19 4,01 Bahawa1pur State 18,22 18,08 11 2 ';ind and Kbairpur State 49,25 44,58 1,41 3,23 2 1 Districts 46,06 41,49 1,34 3,20 2 Khairpur State 3,19 3,09 7 3 I.-Excluding 207 thousand persons claiming Nationalities other than Pakistani. -

World Bank Document
ENVIRONMENTAL ASSESSMENT (EA) AND THE ENVIRONMENTAL AND SOCIAL MANAGEMENT FRAMEWORK Public Disclosure Authorized PUNJAB EDUCATION SECTOR REFORMS PROGRAM-II (PESRP-II) Public Disclosure Authorized PROGRAM DIRECTOR PUNJAB EDUCATION SECTOR REFORMS PROGRAM (PESRP) SCHOOL EDUCATION DEPARTMENT GOVERNMENT OF THE PUNJAB Tel: +92 42 923 2289~95 Fax: +92 42 923 2290 url: http://pesrp.punjab.gov.pk email: [email protected] Public Disclosure Authorized Revised and Updated for PERSP-II February 2012 Public Disclosure Authorized DISCLAIMER This environmental and social assessment report of the activities of the Punjab Education Sector Reforms Program of the Government of the Punjab, which were considered to impact the environment, has been prepared in compliance to the Environmental laws of Pakistan and in conformity to the Operational Policy Guidelines of the World Bank. The report is Program specific and of limited liability and applicability only to the extent of the physical activities under the PESRP. All rights are reserved with the study proponent (the Program Director, PMIU, PESRP) and the environmental consultant (Environs, Lahore). No part of this report can be reproduced, copied, published, transcribed in any manner, or cited in a context different from the purpose for which it has been prepared, except with prior permission of the Program Director, PESRP. EXECUTIVE SUMMARY This document presents the environmental and social assessment report of the various activities under the Second Punjab Education Sector Reforms Program (PESRP-II) – an initiative of Government of the Punjab for continuing holistic reforms in the education sector aimed at improving the overall condition of education and the sector’s service delivery. -
Initial Needs Assesment Report by SANJH Pakistan.Pdf
INITIAL NEEDS ASSESMENT REPORT FLOOD 2014 BY Society for the Advancement of Nature, Justice & Health SANJH Pakistan Muzaffargarh Tehsil Jatoi SANJH (Society for the Advancement of Nature, Name of Organization Justice & Health) Phone Number 066-2424872 , E-mail [email protected] [email protected] Cell Number Contact Person 0341 – 7022965, Website : www.sanjh.org.pk http://twitter.com/SANJH9 www.facebook.com/SANJH.P Links : www.facebook.com/SANJH.Pak skype: sanjh.pk Introduction Executive Summary SANJH Pakistan conducted a post flood needs assessment in the Food, Health sector, Shelter with an estimated Population of 32300 people. The objective of this assessment is to develop an understanding of the impact of flood on lives of affected communities and measures necessary Rehabilitation of Households related urgent needs. This study is composed of two main components. The first is a background study, focused group discussions, stakeholders’ consultation, secondary data analysis, oral testimonials and usage of PLA/PRA techniques, providing a picture of the pre--‐flood socio--‐economic situation, in addition to emergency and early recovery responses in the area. Stakeholder level (focusing on prioritized needs shelter, food, WASH, education and health) and at vulnerable group level (assessing their households conditions during and after the flood). The major findings of this assessment are as follow: o In Tehsil Jatoi Disst.Muzaffargarh district around 216 houses have been partially or completely damaged because of flood waters. o The total loss due to flood in Tehsil Jatoi district Muzaffargarh has been estimated as PKR. 220 Million. District Muzaffargarh Muzaffargarh District is a district of the Punjab province of Pakistan. -

Rapid Assessment Report of Flood-Affected Communities in Muzaffargarh District, Punjab, Pakistan
Rapid Assessment Report of Flood-Affected Communities in Muzaffargarh District, Punjab, Pakistan Residents fleeing rising floodwater near the village of Baseera, Muzaffargarh District Photo by Jason Tanner Monitoring, Evaluation and Accountability Unit August 21, 2010 Acknowledgements We would like to acknowledge the valuable support of the team at SYCOP Muzaffargarh who diligently worked with us to make this study possible. We appreciate the hard work of our data enumerators who traveled extensively to high risk areas to collect the required information. Finally we want to extend our sincere regards to the flood affected communities of Muzaffargarh who cooperated with us in collecting this valuable information. Report by: Sajjad Akram Monitoring, Evaluation & Accountability Manager Omer Aijazi Monitoring, Evaluation & Accountability Coordinator Save the Children, Malakand Response Program, Pakistan © Photo by M. Ismail Tahir Seyal, A submerged Union Council Office in Muzaffargarh District, Punjab Save the Children Federation Inc. 2010 1 List of Abbreviations and Acronyms BHU Basic Health Unit CD Civil Dispensary CH Civil Hospital DHQ District Headquarter Hospital HHs Households IDPs Internally Displaced Persons Km Kilometres MNCH Maternal, Neonatal, and Child Health NFIs Non Food Items SPSS Statistical Package for Social Sciences SYCOP Social Youth Council of Pakistan THQ Tehsil Headquarter Hospital UCs Union Councils 2 Table of Contents Executive Summary ........................................................................................................................ -

MUZAFFARGARH Multiple Indicator Cluster Survey (MICS) Punjab 2007-08
Volume 7 MUZAFFARGARH Multiple Indicator Cluster Survey (MICS) Punjab 2007-08 VOLUME -7 MUZAFFARGARH GOVERNMENT OF THE PUNJAB PLANNING & DEVELOPMENT DEPARTMENT BUREAU OF STATISTICS MARCH 2009 Contributors to the Report: Bureau of Statistics, Government of Punjab, Planning and Development Department, Lahore UNICEF Pakistan Consultant: Manar E. Abdel-Rahman, PhD M/s Eycon Pvt. Limited: data management consultants The Multiple Indicator Cluster Survey was carried out by the Bureau of Statistics, Government of Punjab, Planning and Development Department. Financial support was provided by the Government of Punjab through the Annual Development Programme and technical support by the United Nations Children's Fund (UNICEF). The final reportreport consists consists of of 36 36 volumes volumes. of whichReaders this may document refer to is the the enclosed first. Readers table may of contents refer to thefor reference.enclosed table of contents for reference. This is a household survey planned by the Planning and Development Department, Government of the Punjab, Pakistan (http://www.pndpunjab.gov.pk/page.asp?id=712). Survey tools were based on models and standards developed by the global MICS project, designed to collect information on the situation of children and women in countries around the world. Additional information on the global MICS project may be obtained from www.childinfo.org. Suggested Citation: Bureau of Statistics, Planning and Development Department, Government of the Punjab - Multiple Indicator Cluster Survey, Punjab 2007–08, Lahore, Pakistan. ii MICS PUNJAB 2007-08 FOREWORD Government of the Punjab is committed to reduce poverty through sustaining high growth in all aspects of provincial economy. An abiding challenge in maintaining such growth pattern is concurrent development of capacities in planning, implementation and monitoring which requires reliable and real time data on development needs, quality and efficacy of interventions and impacts. -
Muzaffarghar Blockwise
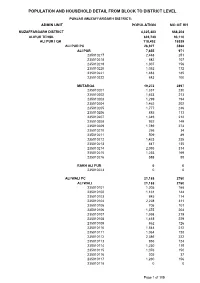
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL PUNJAB (MUZAFFARGARH DISTRICT) ADMIN UNIT POPULATION NO OF HH MUZAFFARGARH DISTRICT 4,325,483 668,204 ALIPUR TEHSIL 639,748 93,110 ALI PUR I QH 118,492 16339 ALI PUR PC 26,927 3868 ALI PUR 7,655 971 235010217 2,448 251 235010218 682 107 235010219 1,307 156 235010220 1,052 172 235010221 1,483 185 235010222 683 100 MUTARQA 19,272 2897 235010201 1,337 230 235010202 1,453 213 235010203 1,299 194 235010204 1,462 202 235010205 1,777 246 235010206 885 113 235010207 1,349 212 235010208 952 149 235010209 1,789 274 235010210 256 34 235010211 509 89 235010212 1,423 235 235010213 847 135 235010214 2,093 314 235010215 1,253 169 235010216 588 88 RAKH ALI PUR 0 0 235010223 0 0 ALI WALI PC 21,188 2760 ALI WALI 21,188 2760 235010101 1,205 168 235010102 1,161 144 235010103 845 114 235010104 2,228 311 235010105 705 101 235010106 1,375 204 235010107 1,598 219 235010108 1,418 229 235010109 862 126 235010110 1,544 212 235010111 1,064 128 235010112 2,386 222 235010113 956 124 235010114 1,230 115 235010115 1,076 150 235010116 305 37 235010117 1,230 156 235010118 0 0 Page 1 of 105 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL PUNJAB (MUZAFFARGARH DISTRICT) ADMIN UNIT POPULATION NO OF HH BAQAR SHAH SHUMALI PC 10,540 1598 BAQAR SHAH SHUMALI 9,273 1411 235010501 1,805 303 235010502 1,087 174 235010503 1,768 229 235010504 1,445 278 235010505 2,373 296 235010506 795 131 NAHAL WALA 1,267 187 235010507 1,267 187 BET NABI SHAH PC 14,034 2363 BET NABI SHAH 14,034 2363 235010301 1,988 314 235010302 -

To View NSP QAT Schedule
EMIS CODE New QAT Program Sr. No Shift Time SCHOOL NAME Address TEHSIL DISTRICT REGION QAT Day /SCHOOL CODE Date Name 12.30 pm NEW AGE PUBLIC UC Name Dhurnal, UC # 39, Moza FATEH 1 B ATK-FJG-NSP-VIII-3061 ATTOCK North 14 18.12.18 NSP to 2.30 pm SCHOOL Dhurnal, Chak / Basti Dhurnal Ada, JANG Tehsil Fateh Jung District Attock 12.30 pm Village Bai, PO Munnoo Nagar, Tehsil HASSANAB 2 B ATK-HDL-NSP-IV-210 Sun Rise High School ATTOCK North 11 14.12.18 NSP to 2.30 pm Hassan Abdal, District Attock DAL 12.30 pm Science Secondary Thatti Sado Shah, Po Akhlas, Tehsil PINDI 3 B ATK-PGB-NSP-IV-214 ATTOCK North 16 20.12.18 NSP to 2.30 pm School Pindi Gheb, District Attock GHEB 12.30 pm Al Aziz Educational Village Gangawali, Teshil Pindi Gheb, PINDI 4 B ATK-PGB-NSP-IV-216 ATTOCK North 17 09.01.19 NSP to 2.30 pm School System District Attock GHEB Basti Haider town(Pindi Gheb), Mouza 12.30 pm PINDI 5 B ATK-PGB-NSP-VII-2477 Hamza Public School Pindi Gheb, UC Name Chakki, UC # 53, ATTOCK North 17 09.01.19 NSP to 2.30 pm GHEB Tehsil Pindi Gheb, District Attock. Mohallah Jibby. Village Qiblabandi, PO 12.30 pm Tameer-e-Seerat Public 6 B ATK-HZO-NSP-IV-211 Kotkay, Via BaraZai, Tehsil Hazro, HAZRO ATTOCK North 12 15.12.18 NSP to 2.30 pm School District Attock 9.00 am to Stars Public Elementary 7 A ATK-ATK-NSP-IV-207 Dhoke Jawanda, Tehsil & District Attock ATTOCK ATTOCK North 12 15.12.18 NSP 11.00 School 12.30 pm Muslim Scholar Public Dhoke Qureshian, P/O Rangwad, tehsil 8 B ATK-JND-NSP-VI-656 JAND ATTOCK North 15 19.12.18 NSP to 2.30 pm School Jand 12.30 pm Farooqabad -

Flood Situation Update 2014
Flood Situation Update 2014 District Muzaffargarh Muzaffargarh District is located in South Punjab. It is spread over an area of 8,435 km. It is located between the river Chenab on its east and Indus river on its West. According to the 1998 census of Pakistan, the population of the district was 2,635,903. It is predominantly rural with only 12.75% population living in urban areas. There are 93 union councils in the district. Administrative setup: Sr. Name of No of Union Total # Tehsil Councils Population 1 Muzaffargarh 35 982866 2 Kot Addu 28 808438 3 Jatoi 16 446546 4 Alipur 14 358098 93 2595948 Population and areas to be affected during flood 2014: The estimation is given by the District Government. The coordination meeting was called by the district government Muzaffargarh and the following data was shared with all stakeholders. Total Total Total Total Sr. # Name of Tehsil Qanoungoi Mouzas Area Population 1 Muzaffargarh 6 110 1,24,035 79,625 2 Jatoi 2 15 16,670 14,563 3 Alipur 4 30 94,447 75,835 12 155 111117 170023 Vulnerable points on Chenab River: These locations/points were declared vulnerable by the district government before flood forecasting in district Muzaffargarh; Rangpur Flood Bund Head Muhammad Wala Bund Thatha Silianwala (Doaba, Buttapur, Jesilwain) Tailari (Sunaki, Lalpur) Khangarh Flood Bund Sher Shah Flood Bund Mochi Wala Flood Bund Mud Wala Flood Bund Shehar Sultan Flood Bund Punjnad, Chandar Bund, Bait Mulla Wali Flood Bund Bait Burra Bund Relief camps detail Tehsil wise: Tehsil Muzaffargarh Sr. # Name of Relief Camps 1 Canal Rest House Jawana Bangla 2 Govt. -

ASA 33/006/2002 Pakistan: Insufficient Protection of Women
PAKISTAN INSUFFICIENT PROTECTION OF WOMEN “The government of Pakistan vigorously condemns the practice of so-called honour killings. Such acts do not find a place in our religion or law. Killing in the name of honour is murder and will be treated as such”, General Musharraf, April 2000 1. INTRODUCTION For years, women in Pakistan have been severely disadvantaged and discriminated against. They have been denied the enjoyment of a whole range of rights - economic, social, civil and political rights and often deprivation in one of these areas has entailed discrimination in another. Women who have been denied social rights including the right to education are also often denied the right to decide in matters relating to their marriage and divorce, are more easily abused in the family and community and are more likely to be deprived of the right to legal redress. Often abuses are compounded; poor girls and women are trafficked and subject to forced marriage, forced prostitution or exploitative work situations such as bonded labour. In all of these situations they are likely to be mentally, physically and sexually abused, again without having the wherewithal to obtain justice.1 Since publishing its 1999 report, Pakistan: Violence against women in the name of honour2, Amnesty International has found that while few positive changes have taken place in the area of women’s rights, the state in Pakistan still by and large fails to provide adequate protection for women against abuses in the custody of the state and in the family and the community. In fact, the number of victims of violence appears to rise. -

S.R.O. No.---/2011.In Exercise Of
PART II] THE GAZETTE OF PAKISTAN, EXTRA., JANUARY 9, 2021 39 S.R.O. No.-----------/2011.In exercise of powers conferred under sub-section (3) of Section 4 of the PEMRA Ordinance 2002 (Xlll of 2002), the Pakistan Electronic Media Regulatory Authority is pleased to make and promulgate the following service regulations for appointment, promotion, termination and other terms and conditions of employment of its staff, experts, consultants, advisors etc. ISLAMABAD SATURDAY, JANUARY 9, 2021 PART II Statutory Notifications (S. R. O.) GOVERNMENT OF PAKISTAN MINISTRY OF NATIONAL FOOD SECURITY AND RESEARCH NOTIFICATION Islamabad, the 6th January, 2021 S. R. O. (17) (I)/2021.—In exercise of the powers conferred by section 15 of the Agricultural Pesticides Ordinance, 1971 (II of 1971), and in supersession of its Notifications No. S.R.O. 947(I)/2002, dated the 23rd December, 2002, S.R.O. 1251 (I)2005, dated the 15th December, 2005, S.R.O. 697(I)/2005, dated the 28th June, 2006, S.R.O. 604(I)/2007, dated the 12th June, 2007, S.R.O. 84(I)/2008, dated the 21st January, 2008, S.R.O. 02(I)/2009, dated the 1st January, 2009, S.R.O. 125(I)/2010, dated the 1st March, 2010 and S.R.O. 1096(I), dated the 2nd November, 2010. The Federal Government is pleased to appoint the following officers specified in column (2) of the Table below of Agriculture Department, Government of the Punjab, to be inspectors within the local limits specified against each in column (3) of the said Table, namely:— (39) Price: Rs. -

Community Based Flood Risk Reduction in District Muzaffargarh, Punjab Province of Pakistan Muhammad Shahjahan Raza
International Journal of Scientific & Engineering Research Volume 9, Issue 12, December-2018 697 ISSN 2229-5518 Community Based Flood Risk Reduction in District Muzaffargarh, Punjab Province of Pakistan Muhammad Shahjahan Raza Abstract—Pakistan shares geographical region which is prone to different kinds of natural disasters. Inception of technology and advancement has bought drastic change in living standards, this shift resulted in occurrence of natural and manmade disasters such as floods, global warming, greenhouse gasses and landslides etc. Floods are most catastrophic in terms of losses. Floods are one of the major type of natural disaster which cannot be stopped but its impact can be controlled and minimized. With the help of community-based risk reduction measure, we can mitigate the adverse effect of floods. The aim of this research paper is to highlight community approach and attitude towards disaster risk reduction and highlight the problems which local community of district Muzaffargarh is facing because of floods. This paper will inspect various factors contributing towards occurrence of floods. Further paper will come up with recommendation solely based on indigenous knowledge and local community suggestions, approaches and perceptions. Index Terms— vulnerability, hazard, mitigation, local community, Disaster Risk Reduction, Natural Disasters, Catastrophic. —————————— —————————— 1 INTRODUCTION Economically it is agriculture-based district along with District Muzaffargarh is in southern belt of Punjab some industrial zones. Agriculture serve as base lined for community employment or source of income. province at the distance of 34 kilometers across river Chenab on its East. On its North it shares boundary with District Muzaffargarh is prone to seasonal flood due to its subdivision of district Lyaah.