User Specific Assistive Technology: Hand Mounted Swtich Control Platform Design
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Luna Moth: Supporting Creativity in the Cloud
Pedro Alfaiate Instituto Superior Técnico / Luna Moth INESC-ID Inês Caetano Instituto Superior Técnico / INESC-ID Supporting Creativity in the Cloud António Leitão Instituto Superior Técnico / INESC-ID 1 ABSTRACT Algorithmic design allows architects to design using a programming-based approach. Current algo- 1 Migration from desktop application rithmic design environments are based on existing computer-aided design applications or building to the cloud. information modeling applications, such as AutoCAD, Rhinoceros 3D, or Revit, which, due to their complexity, fail to give architects the immediate feedback they need to explore algorithmic design. In addition, they do not address the current trend of moving applications to the cloud to improve their availability. To address these problems, we propose a software architecture for an algorithmic design inte- grated development environment (IDE), based on web technologies, that is more interactive than competing algorithmic design IDEs. Besides providing an intuitive editing interface which facilitates programming tasks for architects, its performance can be an order of magnitude faster than current aalgorithmic design IDEs, thus supporting real-time feedback with more complex algorithmic design programs. Moreover, our solution also allows architects to export the generated model to their preferred computer-aided design applications. This results in an algorithmic design environment that is accessible from any computer, while offering an interactive editing environment that inte- grates into the architect’s workflow. 72 INTRODUCTION programming languages that also support traceability between Throughout the years, computers have been gaining more ground the program and the model: when the user selects a component in the field of architecture. In the beginning, they were only used in the program, the corresponding 3D model components are for creating technical drawings using computer-aided design highlighted. -

Work Catalog
Your Partner In Safety -Since 1979- • Illness Prevention Signage BACK TO WORK • Disposable Clothing • Respiratory CATALOG Protection What you need to get back to work safely • Eye Protection • Disinfectants Back To Work Novel Coronavirus (nCoV) Infection Overview The Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) are closely monitoring an outbreak caused by a novel (new) coronavirus first identified in Wuhan, Hubei Province, China. Chinese authorities iden- tified the new coronavirus, which has resulted in hundreds of confirmed cases in China, including cases outside Wuhan, with additional cases being identified in a growing number of countries internationally. These numbers will likely grow given the high amount of travel associated with the Lunar New Year holiday. It has been confirmed that the virus can spread from human to human although specific routes of transmission (i.e. airborne, direct contact, ingestion, etc.) have yet to be definitively determined. Common symptoms include runny nose, headache, cough, sore throat, fever, and a general feeling of being unwell. The CDC is providing the following precautions for health care providers: “Healthcare providers should obtain a detailed travel history for patients with fever and respiratory symptoms. For pa- tients who traveled to Wuhan on or after December 1, 2019 and had onset of illness within 2 weeks of leaving, consider the novel coronavirus outbreak in China when evaluating a patient with these symptoms and notify infection control per- sonnel and your local health department immediately. Although routes of transmission have yet to be definitively determined, CDC recommends a cautious approach to inter- acting with patients under investigation. -

(12) United States Patent (10) Patent No.: US 6,702,110 B1
USOO670211 OB1 (12) UnitedO States Patent (10) Patent No.: US 6,702,110 B1 Flores, Jr. et al. (45) Date of Patent: Mar. 9, 2004 (54) DISC STORAGE CONTAINER 5,573,120 A 11/1996 Kaufman et al. ........... 206/755 5,574,716 A 11/1996 Uchida ....................... 369/291 w 5,584,391 A 12/1996 Weisburn (75) Inventors: Victor' E. SER 5,590,768 A 1/1997 Hilton et al. ............ 206/308.1 erdes, CA (US); Victorio M. Flores, 5,597,068 A 1/1997 Weisburn et al. ........ 206/308.1 III, San Pedro, CA (US); Ernst C. 5,615,779 A 4/1997 Marsilio et al. .............. 211/40 Benjamins, Covina, CA (US) 5,682,991. A 11/1997 Lammerant et al. ..... 206/308.1 5,690,218 A 11/1997 McCamy et al. ........... 206/303 (73) ASSignee: Ace Packaging, Inc., Lake Forest, CA D387,217 S 12/1997 Lakoski et al. .............. D6/407 (US) 5,713,463 A 2/1998 Lakoski et al. .......... 206/308.1 5,762,187 A 6/1998 Belden, Jr. et al. ...... 206/3O8.2 - - - - 5,779,038 A 7/1998 Herr et al. ............... 206/3O8.2 (*) Notice: Subject to any disclaimer, the term of this 5,782,350 A 7/1998 Weisburn et al. ........ 206/3O8.2 patent is extended or adjusted under 35 5,788,068 A 8/1998 Fraser et al. ................ 206/310 U.S.C. 154(b) by 0 days. 5,794,796 A 8/1998 Weisburn ..................... 211/40 5,816,394 A 10/1998 O’Brien et al. .......... 206/308.1 5,829,582 A 11/1998 Ippolito et al. -

Brands Talk Sustainability: Exclusive M&S and Coca-Cola Interviews
VOLUME 13.1 – 2018 BRANDS TALK SUSTAINABILITY: EXCLUSIVE M&S AND COCA-COLA INTERVIEWS WHAT ARE THE DEFINING TRENDS OF 2018? SERIALISATION PERSPECTIVES MINIMALIST DESIGN: THE POWER OF SILENCE INTRODUCING THE DIGITAL NOMAD Cover image © Mehmet Gözetlik Head of Content Senior Account VOLUME 13.1 – 2018 Tim Sykes Managers Kevin Gambrill Editors Jesse Roberts Elisabeth Skoda Libby White Account Manager Dominic Kurkowski Head of Studio Gareth Harrey Executive Assistant Amber Dawson Art Editor Paul Holden-Abbott IT Support Syed Hassan Advertising Coordinator Kayleigh Harvey Data Manager 3 Editorial Tim Sykes Andrew Wood 5 M&S Interview Are we looking at a one-polymer future? 7 2018 Predictions This year’s defining trends in CPG and retail packaging 14 Smart Manufacturing Automation perspectives 17 Innovation Spotlight Pont brings twist to cap design Packaging Europe Ltd 18 Coca-Cola Interview Inside the new sustainability plan Part of the Rapid News Communications Group 20 Pharmapack The future is now Alkmaar House, Alkmaar Way, Norwich, Norfolk, NR6 6BF, UK 23 Bostik What if hotmelt adhesives could bring comfort and safety in your plant? Registered Office: Carlton House, Sandpiper Way, 25 Smurfit Kappa On-shelf differentiation in advance Chester Business Park, Chester, CH4 9QE. 28 Bioplastics EUBP Conference review Company No: 10531302. 31 ADF/PCD Paris Counting down to the next edition Registered in England. VAT Registration No. GB 265 4148 96 33 Prosweets Sweet solution 35 Ipack-Ima Ipack-Ima returns with new vision Telephone: +44 (0)1603 -

Food Packaging Technology
FOOD PACKAGING TECHNOLOGY Edited by RICHARD COLES Consultant in Food Packaging, London DEREK MCDOWELL Head of Supply and Packaging Division Loughry College, Northern Ireland and MARK J. KIRWAN Consultant in Packaging Technology London Blackwell Publishing © 2003 by Blackwell Publishing Ltd Trademark Notice: Product or corporate names may be trademarks or registered Editorial Offices: trademarks, and are used only for identification 9600 Garsington Road, Oxford OX4 2DQ and explanation, without intent to infringe. Tel: +44 (0) 1865 776868 108 Cowley Road, Oxford OX4 1JF, UK First published 2003 Tel: +44 (0) 1865 791100 Blackwell Munksgaard, 1 Rosenørns Allè, Library of Congress Cataloging in P.O. Box 227, DK-1502 Copenhagen V, Publication Data Denmark A catalog record for this title is available Tel: +45 77 33 33 33 from the Library of Congress Blackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton South, British Library Cataloguing in Victoria 3053, Australia Publication Data Tel: +61 (0)3 9347 0300 A catalogue record for this title is available Blackwell Publishing, 10 rue Casimir from the British Library Delavigne, 75006 Paris, France ISBN 1–84127–221–3 Tel: +33 1 53 10 33 10 Originated as Sheffield Academic Press Published in the USA and Canada (only) by Set in 10.5/12pt Times CRC Press LLC by Integra Software Services Pvt Ltd, 2000 Corporate Blvd., N.W. Pondicherry, India Boca Raton, FL 33431, USA Printed and bound in Great Britain, Orders from the USA and Canada (only) to using acid-free paper by CRC Press LLC MPG Books Ltd, Bodmin, Cornwall USA and Canada only: For further information on ISBN 0–8493–9788–X Blackwell Publishing, visit our website: The right of the Author to be identified as the www.blackwellpublishing.com Author of this Work has been asserted in accordance with the Copyright, Designs and Patents Act 1988. -
The Dynisco Extrusion Processors Handbook 2Nd Edition
The Dynisco Extrusion Processors Handbook 2nd edition Written by: John Goff and Tony Whelan Edited by: Don DeLaney Acknowledgements We would like to thank the following people for their contributions to this latest edition of the DYNISCO Extrusion Processors Handbook. First of all, we would like to thank John Goff and Tony Whelan who have contributed new material that has been included in this new addition of their original book. In addition, we would like to thank John Herrmann, Jim Reilly, and Joan DeCoste of the DYNISCO Companies and Christine Ronaghan and Gabor Nagy of Davis-Standard for their assistance in editing and publication. For the fig- ures included in this edition, we would like to acknowledge the contributions of Davis- Standard, Inc., Krupp Werner and Pfleiderer, Inc., The DYNISCO Companies, Dr. Harold Giles and Eileen Reilly. CONTENTS SECTION 1: INTRODUCTION TO EXTRUSION Single-Screw Extrusion . .1 Twin-Screw Extrusion . .3 Extrusion Processes . .6 Safety . .11 SECTION 2: MATERIALS AND THEIR FLOW PROPERTIES Polymers and Plastics . .15 Thermoplastic Materials . .19 Viscosity and Viscosity Terms . .25 Flow Properties Measurement . .28 Elastic Effects in Polymer Melts . .30 Die Swell . .30 Melt Fracture . .32 Sharkskin . .34 Frozen-In Orientation . .35 Draw Down . .36 SECTION 3: TESTING Testing and Standards . .37 Material Inspection . .40 Density and Dimensions . .42 Tensile Strength . .44 Flexural Properties . .46 Impact Strength . .47 Hardness and Softness . .48 Thermal Properties . .49 Flammability Testing . .57 Melt Flow Rate . .59 Melt Viscosity . .62 Measurement of Elastic Effects . .64 Chemical Resistance . .66 Electrical Properties . .66 Optical Properties . .68 Material Identification . .70 SECTION 4: THE SCREW AND BARREL SYSTEM Materials Handling . -
Syringe Assembly
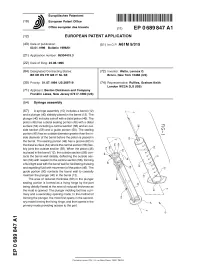
^ ^ ^ ^ I ^ ^ ^ ^ ^ ^ II ^ II ^ ^ ^ ^ ^ ^ ^ ^ ^ ^ ^ ^ ^ I ^ European Patent Office Office europeen des brevets EP 0 689 847 A1 EUROPEAN PATENT APPLICATION (43) Date of publication: (51 ) |nt CIA A61 M 5/31 5 03.01.1996 Bulletin 1996/01 (21) Application number: 95304415.3 (22) Date of filing: 23.06.1995 (84) Designated Contracting States: (72) Inventor: Watts, Lennox O. BE DE ES FR GB IT NL SE Bronx, New York 10466 (US) (30) Priority: 01.07.1994 US 269719 (74) Representative: Ruffles, Graham Keith London WC2A 3LS (GB) (71) Applicant: Becton Dickinson and Company Franklin Lakes, New Jersey 07417-1880 (US) (54) Syringe assembly (57) A syringe assembly (10) includes a barrel (12) and a plunger (40) slidably placed in the barrel (12). The plunger (40) includes a shaft with a distal piston (46). The piston (46) has a distal sealing portion (48) with a distal surface (54) including a central section (56) and an out- side section (58) and a guide portion (50). The sealing portion (48) has an outside diameter greater than the in- side diameter of the barrel before the piston is placed in the barrel. The sealing portion (48) has a groove (62) in the distal surface (54) where the central section (56) flex- ibly joins the outside section (58). When the piston (46) is placed in the barrel (1 2), the outside section ((58) con- tacts the barrel wall distally, deflecting the outside sec- tion (58) with respect to the central sectionpart.� (56), forming a fluid tight seal with the barrel wall for facilitating drawing and expelling fluid with movement of the piston (46). -

Development of a Single Use Device Intended to Wash Blood Clot Debris from a Stent Retriever in the Operating Room
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2020 DEVELOPMENT OF A SINGLE USE DEVICE INTENDED TO WASH BLOOD CLOT DEBRIS FROM A STENT RETRIEVER IN THE OPERATING ROOM Shane Diller Virginia Commonwealth University Follow this and additional works at: https://scholarscompass.vcu.edu/etd Part of the Biomechanical Engineering Commons, Biomedical Devices and Instrumentation Commons, and the Manufacturing Commons © The Author Downloaded from https://scholarscompass.vcu.edu/etd/6450 This Thesis is brought to you for free and open access by the Graduate School at VCU Scholars Compass. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of VCU Scholars Compass. For more information, please contact [email protected]. DEVELOPMENT OF A SINGLE USE DEVICE INTENDED TO WASH BLOOD CLOT DEBRIS FROM A STENT RETRIEVER IN THE OPERATING ROOM A thesis submitted to fulfill the requirements for the degree of Master of Science in Mechanical and Nuclear Engineering at Virginia Commonwealth University by SHANE DILLER B.S. in Biomedical Engineering, Virginia Commonwealth University, May 2014 Department of Mechanical and Nuclear Engineering Virginia Commonwealth University Richmond, Virginia 2019-2020 Advisor: FRANKLIN BOST PROFESSOR, CO-DIRECTOR, VCU INSTITUTE FOR ENGINEERING AND MEDICINE I Acknowledgements I would like to thank Professor Bost and Dr. Mossi for giving me the opportunity to pursue my Master’s in a field that I am deeply passionate about. Through your mentorship, I have become not only a better engineer, but a better communicator and a better person. I look forward to weaving my knowledge of Biomedical Engineering and Mechanical Engineering to help improve the lives of others. -

Design for Additive Manufacturing: Tool Review and a Case Study
applied sciences Article Design for Additive Manufacturing: Tool Review and a Case Study Daniel Moreno Nieto 1,* and Daniel Moreno Sánchez 2 1 Departamento de Ingeniería Mecánica y Diseño Industrial, Escuela Superior de Ingeniería, Universidad de Cádiz, Puerto Real, 11510 Cádiz, Spain 2 Departamento de Ciencia de los Materiales e Ingeniería Metalúrgica y Química Inorgánica, Facultad de Ciencias, IMEYMAT, Campus Río San Pedro, Universidad de Cádiz, PuertoReal, 11510 Cádiz, Spain; [email protected] * Correspondence: [email protected]; Tel.: +34-676923332 Abstract: This paper aims to collect in a structured manner different computer-aided engineering (CAE) tools especially developed for additive manufacturing (AM) that maximize the capabilities of this technology regarding product development. The flexibility of the AM process allows the manu- facture of highly complex shapes that are not possible to produce by any other existing technology. This fact enables the use of some existing design tools like topology optimization that has already existed for decades and is used in limited cases, together with other novel developments like lattice design tools. These two technologies or design approaches demand a highly flexible manufacturing system to be applied and could not be used before, due to the conventional industrial process limita- tions. In this paper, these technologies will be described and combined together with other generic or specific design tools, introducing the study case of an additive manufactured mechanical design of a bicycle stem. Citation: Moreno Nieto, D.; Moreno Keywords: additive manufacturing; industrial design; fused deposition modeling; parametric design; Sánchez, D. Design for Additive industrial design; CAD computer aided design; topology optimization; lattice design Manufacturing: Tool Review and a Case Study. -

DESIGN ESSENTIALS for 3D Printing Design Essentials for 3D Printing
DESIGN ESSENTIALS for 3D Printing Design Essentials for 3D Printing Industrial 3D printing opens up many new design possibilities, but it’s important to keep a few Contents fundamental principles in mind when designing for additive manufacturing processes. Most of these are 03 Rapid Prototyping with Stereolithography fairly obvious like feature resolution, surface finish, and material selection, but there’s more to 3D printing 06 Prototyping with PolyJet 3D Printing success than selecting the right material and process. If you will eventually need increased part quantities 08 3D Printing Fully Functional Parts with through more traditional processes like injection molding, Selective Laser Sintering you should considering the part’s moldability even 11 How to Use Multi Jet Fusion for Functional when designing early prototypes. Understanding the 3D-Printed Parts fundamental principles for 3D printing will help you get the most out the versatile technology—whether you're 14 The Basics of Metal 3D Printing Part Design iterating part design through rapid prototyping or creating end-use production parts. Got a 3D CAD model ready to be quoted? Upload it today for an instant quote. GET INSTANT QUOTE © Proto Labs, Inc. 1999–2018 Protolabs HQ, 5540 Pioneer Creek Dr., Maple Plain, MN 55359 USA | 877-479-3680 2 Design Essentials for 3D Printing Rapid Prototyping with Stereolithography 3 1 Stereolithography, or SLA, emerged in the 2 mid-1980s and established itself as a staple of additive manufacturing (now known as 3D printing) over the next decade. Since that 10 time, SL’s ability to quickly and accurately create 6 complex prototypes has helped transform the design world like never before. -

Computational Terrain Modeling with Distance Functions for Large Scale Landscape Design
222 Full Paper Computational Terrain Modeling with Distance Functions for Large Scale Landscape Design Ilmar Hurkxkens1, Mathias Bernhard2 1ETH Zurich, Chair of Landscape Architecture, Zurich/Switzerland · [email protected] 2ETH Zurich, Digital Building Technologies, Zurich/Switzerland Abstract: The act of reshaping terrain to meet cultural, infrastructural and ecological demands becomes an increasingly important practice with upcoming challenges like sea level rise, landslides, floods and drought. While recent hardware innovation in 3D sensing and autonomous construction machinery has opened up the digital recording and digital fabrication of large-scale topographies (HURKXKENS 2017), 3D modeling of digital terrain is still a complex and time-consuming task. The found geometry of the ground, largely irregular in shape and material constitution, poses serious problems and limitations for an efficient digital workflow today. Based on digital elevation data, this paper demonstrates a powerful computational landform editing tool using 2D distance functions. Keywords: Computational terrain modeling, procedural design, signed distance functions, large scale landscape design, digital fabrication 1 Introduction Most designer-oriented software packages use boundary representations (BReps) in NURBS or mesh surfaces to provide a 3D visual interface to the designer. Using BReps in large scale land- scape design have proven very tedious and difficult to work with. Often a combination of the two is used to create clean-cut topography in NURBS which is embedded in a mesh for the project surroundings (WALLISS & RAHMANN 2016). The digital equivalent of terrain modeling is best described as Boolean operations that tend to be problematic on large NURBS or meshes, quickly reaching the limits of the conventional software packages from Autodesk, Nemetschek or McNeel (MCNEEL 2000). -

Papers for the International Journal of Architectural Computing
Processing Architecture António Leitão, Inês Caetano and Hugo Correia INESC-ID/Instituto Superior Técnico, Universidade de Lisboa, Portugal Av. Rovisco Pais, 1 1049-001 Lisboa, Portugal [email protected] Abstract Programming promotes creative freedom but might require considerable effort to learn. The Processing language was created to simplify this learning process. Due to its graphical capabilities, the language has become very popular among the electronic arts and design communities. Unfortunately, this popularity could not be extended to the architecture community, which relies on traditional heavyweight CAD and BIM applications that cannot be programmed using Processing. As a result, it becomes difficult for architects to take advantage of Processing. To solve this problem, we propose an implementation of Processing that runs in the context of the most used CAD tools in architecture. Our implementation allows Processing to generate 2D or 3D models that are directly usable for architectural work. To this end, we also propose extensions to the language, including three-dimensional modelling primitives that dramatically simplify the effort needed for developing large and complex architectural models with Processing. 1. INTRODUCTION Programming was originally considered a very specialist activity and not part of a design education [1]. Nowadays, many designers are aware of its potential and want to take advantage of it for many different purposes, including automating repetitive tasks, form finding and optimization [2]. Unfortunately, learning a programming language and the associated programming techniques is far from a trivial task and, thus, requires carefully designed languages and programming environments. In this paper, we focus on one of these languages: Processing.