Modulation of NK Cell Function with Agonistic Α-CD137 Antibodies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

North Fork of the St. Lucie River Floodplain Vegetation Technical Report
NORTH FORK ST. LUCIE RIVER FLOODPLAIN VEGETATION TECHNICAL REPORT WR-2015-005 Coastal Ecosystem Section Applied Sciences Bureau Water Resources Division South Florida Water Management District Final Report July 2015 i Resources Division North Fork of the St. Lucie River Floodplain Vegetation Technical Report ACKNOWLEDGEMENTS This document is the result of a cooperative effort between the Coastal Ecosystems Section of South Florida Water Management District (SFWMD) and the Florida Department of Environmental Protection (FDEP), Florida Park Service (FPS) at the Savannas Preserve State Park in Jensen Beach, Florida and the Indian River Lagoon Aquatic Preserve Office in Fort Pierce, Florida. The principle author of this document was as follows: Marion Hedgepeth SFWMD The following staff contributed to the completion of this report: Cecilia Conrad SFWMD (retired) Jason Godin SFWMD Detong Sun SFWMD Yongshan Wan SFWMD We would like to acknowledge the contributions of Christine Lockhart of Habitat Specialist Inc. with regards to the pre-vegetation plant survey, reference collection established for this project, and for her assistance with plant identifications. We are especially grateful to Christopher Vandello of the Savannas Preserve State Park and Laura Herren and Brian Sharpe of the FDEP Indian River Lagoon Aquatic Preserves Office for their assistance in establishing the vegetation transects and conducting the field studies. And, we would like to recognize other field assistance from Mayra Ashton, Barbara Welch, and Caroline Hanes of SFWMD. Also, we would like to thank Kin Chuirazzi for performing a technical review of the document. ii North Fork of the St. Lucie River Floodplain Vegetation Technical Report TABLE OF CONTENTS Acknowledgements ..........................................................................................................................ii List of Tables ............................................................................................................................... -

Monoclonal Antibodies Against Cd30 Lacking In
(19) TZZ_97688¥_T (11) EP 1 976 883 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: C07K 16/28 (2006.01) A61P 35/00 (2006.01) 03.10.2012 Bulletin 2012/40 A61P 37/00 (2006.01) (21) Application number: 07718000.8 (86) International application number: PCT/US2007/001451 (22) Date of filing: 17.01.2007 (87) International publication number: WO 2007/084672 (26.07.2007 Gazette 2007/30) (54) MONOCLONAL ANTIBODIES AGAINST CD30 LACKING IN FUCOSYL AND XYLOSYL RESIDUES MONOKLONALE ANTIKÖRPER GEGEN CD30 OHNE FUCOSYL- UND XYLOSYLRESTE ANTICORPS MONOCLONAUX ANTI-CD30 DEPOURVUS DE RESIDUS FUCOSYL ET XYLOSYL (84) Designated Contracting States: • WANG, Ming-Bo AT BE BG CH CY CZ DE DK EE ES FI FR GB GR Canberra Australian Capital Territory 2617 (AU) HU IE IS IT LI LT LU LV MC NL PL PT RO SE SI SK TR (74) Representative: Tuxworth, Pamela M. Designated Extension States: J A Kemp RS 14 South Square Gray’s Inn (30) Priority: 17.01.2006 US 759298 P London WC1R 5JJ (GB) 07.04.2006 US 790373 P 11.04.2006 US 791178 P (56) References cited: 09.06.2006 US 812702 P WO-A-03/059282 US-A1- 2004 261 148 11.08.2006 US 837202 P 11.08.2006 US 836998 P • P. BORCHMANN ET AL.: "The human anti-CD30 antibody 5F11 shows in vitro and in vivo activity (43) Date of publication of application: against malignant lymphoma." BLOOD, vol. 102, 08.10.2008 Bulletin 2008/41 no. -
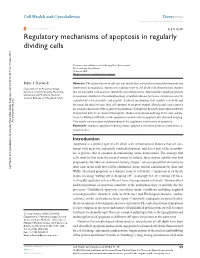
Regulatory Mechanisms of Apoptosis in Regularly Dividing Cells
Cell Health and Cytoskeleton Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Regulatory mechanisms of apoptosis in regularly dividing cells Ribal S Darwish Abstract: The balance between cell survival and death is essential for normal development and Department of Anesthesiology, homeostasis of organisms. Apoptosis is a distinct type of cell death with ultrastructural features Division of Critical Care Medicine, that are consistent with an active, inherently controlled process. Abnormalities and dysregulation University of Maryland Medical of apoptosis contribute to the pathophysiology of multiple disease processes. Apoptosis is strictly Center, Baltimore, Maryland, USA regulated by several positive and negative feedback mechanisms that regulate cell death and determine the final outcome after cell exposure to apoptotic stimuli. Mitochondria and caspases are central components of the regulatory mechanisms of apoptosis. Recently, noncaspase pathways of apoptosis have been explored through the studies of apoptosis-inducing factor and endonu- clease G. Multiple difficulties in the apoptosis research relate to apoptosis detection and imaging. For personal use only. This article reviews current understanding of the regulatory mechanisms of apoptosis. Keywords: caspases, apoptosis-inducing factor, apoptosis inhibitory proteins, cytochrome c, mitochondria Introduction Apoptosis is a distinct type of cell death with ultrastructural features that are con- sistent with an active, inherently controlled process, and it is a part of the necrobio- sis, a process that is essential in maintaining tissue homeostasis. The concept that cells must be lost from the normal tissues to balance their mitotic activity was first proposed by the German anatomist Ludwig Graper,1 who proposed that chromolysis must exist in the cells that will be eliminated. -

US 2017/0020926 A1 Mata-Fink Et Al
US 20170020926A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2017/0020926 A1 Mata-Fink et al. (43) Pub. Date: Jan. 26, 2017 (54) METHODS AND COMPOSITIONS FOR 62/006,825, filed on Jun. 2, 2014, provisional appli MMUNOMODULATION cation No. 62/006,829, filed on Jun. 2, 2014, provi sional application No. 62/006,832, filed on Jun. 2, (71) Applicant: RUBIUS THERAPEUTICS, INC., 2014, provisional application No. 61/991.319, filed Cambridge, MA (US) on May 9, 2014, provisional application No. 61/973, 764, filed on Apr. 1, 2014, provisional application No. (72) Inventors: Jordi Mata-Fink, Somerville, MA 61/973,763, filed on Apr. 1, 2014. (US); John Round, Cambridge, MA (US); Noubar B. Afeyan, Lexington, (30) Foreign Application Priority Data MA (US); Avak Kahvejian, Arlington, MA (US) Nov. 12, 2014 (US) ................. PCT/US2O14/0653O4 (21) Appl. No.: 15/301,046 Publication Classification (22) PCT Fed: Mar. 13, 2015 (51) Int. Cl. A6II 35/28 (2006.01) (86) PCT No.: PCT/US2O15/02O614 CI2N 5/078 (2006.01) (52) U.S. Cl. S 371 (c)(1), CPC ............. A61K 35/28 (2013.01); C12N5/0641 (2) Date: Sep. 30, 2016 (2013.01): CI2N 5/0644 (2013.01); A61 K Related U.S. Application Data 2035/122 (2013.01) (60) Provisional application No. 62/059,100, filed on Oct. (57) ABSTRACT 2, 2014, provisional application No. 62/025,367, filed on Jul. 16, 2014, provisional application No. 62/006, Provided are cells containing exogenous antigen and uses 828, filed on Jun. 2, 2014, provisional application No. -

Modulators of the Function of FAS Receptors and Other Proteins
(19) *EP002042509A1* (11) EP 2 042 509 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 01.04.2009 Bulletin 2009/14 C07H 21/04 (2006.01) C12N 15/63 (2006.01) C12N 15/85 (2006.01) C12N 15/86 (2006.01) (2006.01) (2006.01) (21) Application number: 08018971.5 C07K 14/00 A61K 39/395 (22) Date of filing: 14.06.1996 (84) Designated Contracting States: (72) Inventors: AT BE CH DE DK ES FI FR GB GR IE IT LI LU MC • Wallach, David NL PT SE 76406 Rehovot (IL) Designated Extension States: • Boldin, Mark AL LT LV SI 76000 Rehovot (IL) • Goncharov, Tanya (30) Priority: 16.07.1995 IL 11461595 76000 Rehovot (IL) 17.08.1995 IL 11498695 • Goltsev, Yury 14.09.1995 IL 11531995 76000 Rehovot (IL) 27.12.1995 IL 11658895 16.04.1996 IL 11793296 (74) Representative: Vossius & Partner Siebertstraße 4 (62) Document number(s) of the earlier application(s) in 81675 München (DE) accordance with Art. 76 EPC: 96919472.9 / 0 914 325 Remarks: This application was filed on 30-10-2008 as a (71) Applicant: YEDA RESEARCH AND divisional application to the application mentioned DEVELOPMENT COMPANY, LTD. under INID code 62. 76 100 Rehovot (IL) (54) Modulators of the function of FAS receptors and other proteins (57) The present invention provides proteins capable ceptor. In addition, peptide inhibitors which interfere with of modulating or mediating the FAS receptor ligand or the proteolytic activity of MORT-1-binding proteins hav- TNF effect on cells carrying FAS receptor or p55 receptor ing proteolytic activity are provided as well as a method by binding or interacting with MORT-1 protein, which in of designing them. -

1 Women for Sobriety Combined Bibliographies
Women for Sobriety Combined Bibliographies (June 2016) Compiled by Rita A. Chaney, MS Women for Sobriety Professional Bibliography Abbott, A. A., & Olson, M. (1994). A feminist approach to substance abuse treatment and service delivery. Women’s Health & Social Work, 67-83. Angove, R., & Fothergill, A. (2003, April). Women and alcohol: Misrepresented and misunderstood. Journal of Psychiatric & Mental Health Nursing, 10(2), 213-219. doi: 10.1046/j.1365-2850.2003.00587.x. Atkins, Jr., J. R, & Hawdon, J. E. (2007). Religiosity and participation in mutual-aid support groups for addiction. Journal of Substance Abuse Treatment, 33(3), 321-331. Berenson, D. (1992). Powerlessness—Liberating or enslaving? Responding to the feminist critique of the Twelve Steps. Journal of Feminist Family Therapy, 3(3), 67-84. Bogart, C. J., & Pearce, C. E. (2003). “13th-Stepping:” Why Alcoholics Anonymous is not always a safe place for women. Journal of Addictions Nursing, 14, 43-47. Bond, L. M., & Csordas, T. J. (2014). The paradox of powerlessness. Alcoholism Treatment Quarterly, 32(2-3), 141-156. Chaney, R., & White, W. L. (1992). Metaphors of transformation: Feminine and masculine. Bloomington, IL: Lighthouse Training Institute. Fenner, R.M., & Gifford, M.H. (2012). Women for Sobriety: 35 years of challenges, changes, and continuity. Journal of Groups in Addiction and Recovery, 7(2-4), 142-170. Fenner, R.M., & Gifford, M.H. (2015). Women for Sobriety: An alternative recovery choice. Counselor, 16(4), 18-21. Hafner, S. (1992). Nice girls don’t drink: Stories of recovery. New York, NY: Bergin & Garvey. [An interview of Kirkpatrick]. Hall, M. J., & Tidwell, W. -

C07k - 2021.08
CPC - C07K - 2021.08 C07K PEPTIDES (peptides in foodstuffs A23; obtaining protein compositions for foodstuffs, working-up proteins for foodstuffs A23J; preparations for medicinal purposes A61K; peptides containing beta-lactam rings C07D; cyclic dipeptides not having in their molecule any other peptide link than those which form their ring, e.g. piperazine-2,5-diones, C07D; ergot alkaloids of the cyclic peptide type C07D 519/02; macromolecular compounds having statistically distributed amino acid units in their molecules, i.e. when the preparation does not provide for a specific; but for a random sequence of the amino acid units, homopolyamides and block copolyamides derived from amino acids C08G 69/00; macromolecular products derived from proteins C08H 1/00; preparation of glue or gelatine C09H; single cell proteins, enzymes C12N; genetic engineering processes for obtaining peptides C12N 15/00; compositions for measuring or testing processes involving enzymes C12Q; investigation or analysis of biological material G01N 33/00) Relationships with other classification places An amino acid per se is classified in C07D while peptides (starting from dipeptides) are classified in C07K. Subclass C07K is a function oriented entry for the compounds themselves and does not cover the application or use of the compounds under the subclass definition. For classifying such information other entries exist, for example: preservation of bodies of humans or animals or plants or parts thereof; Biocides, e.g. as disinfectants, as pesticides, as herbicides; pest repellants or attractants; plant growth regulators are classified in A01N. Preparations for medical, dental, or toilet purposes are classified in A61K. Amino acids or derivatives thereof are classified in C07C or C07D. -
2020 Census National Redistricting Data Summary File 2020 Census of Population and Housing
2020 Census National Redistricting Data Summary File 2020 Census of Population and Housing Technical Documentation Issued February 2021 SFNRD/20-02 Additional For additional information concerning the Census Redistricting Data Information Program and the Public Law 94-171 Redistricting Data, contact the Census Redistricting and Voting Rights Data Office, U.S. Census Bureau, Washington, DC, 20233 or phone 1-301-763-4039. For additional information concerning data disc software issues, contact the COTS Integration Branch, Applications Development and Services Division, Census Bureau, Washington, DC, 20233 or phone 1-301-763-8004. For additional information concerning data downloads, contact the Dissemination Outreach Branch of the Census Bureau at <[email protected]> or the Call Center at 1-800-823-8282. 2020 Census National Redistricting Data Summary File Issued February 2021 2020 Census of Population and Housing SFNRD/20-01 U.S. Department of Commerce Wynn Coggins, Acting Agency Head U.S. CENSUS BUREAU Dr. Ron Jarmin, Acting Director Suggested Citation FILE: 2020 Census National Redistricting Data Summary File Prepared by the U.S. Census Bureau, 2021 TECHNICAL DOCUMENTATION: 2020 Census National Redistricting Data (Public Law 94-171) Technical Documentation Prepared by the U.S. Census Bureau, 2021 U.S. CENSUS BUREAU Dr. Ron Jarmin, Acting Director Dr. Ron Jarmin, Deputy Director and Chief Operating Officer Albert E. Fontenot, Jr., Associate Director for Decennial Census Programs Deborah M. Stempowski, Assistant Director for Decennial Census Programs Operations and Schedule Management Michael T. Thieme, Assistant Director for Decennial Census Programs Systems and Contracts Jennifer W. Reichert, Chief, Decennial Census Management Division Chapter 1. -

(12) United States Patent (10) Patent No.: US 7,799,902 B2 Browning Et A1
USOO7799902B2 (12) United States Patent (10) Patent No.: US 7,799,902 B2 Browning et a1. (45) Date of Patent: Sep. 21, 2010 (M)IEEDHORCOUHJMLKENBAND 2mmmww4Ai umm @m?an COMPOSITIONS THEREOF 2004/0198635 A1 10/2004 Browning et al. 2005/0037003 A1 2/2005 Browning et al. (75) Inventors: Jeffrey L. Browning, Cambridge, MA 2005/0281811 A1 12/2005 Browning et al. (US); Veronique Bailly, Boxborough, 2006/0104971 A1 5/2006 Garber et a1. MA (US); Ellen Garber, Cambridge, 2006/0134102 A1 6/2006 LePage et a1. MA (US) 2006/0222644 A1 10/2006 Garber et a1. 2006/0280722 A1 12/2006 Browning et al. (73) Assignee: Biogen Idec MA Inc., Cambridge, MA 2007/0154476 A1 7/2007 Browning et al. (Us) (*) Notice: Subject to any disclaimer, the term of this FOREIGN PATENT DOCUMENTS patent is extended or adjusted under 35 U.S.C. 154(b) by 420 days. EP 0509553 B1 10/1992 EP 0519596 B1 12/1992 (21) App1.No.: 11/524,786 WO WO-91/09967 A1 7/1991 WO WO-92/00329 A1 1/1992 (22) Filed: Sep. 21, 2006 WO WO-94/04679 A1 3/1994 WO WO-94/ 13808 A2 6/ 1994 (65) Prior Publication Data WO WO-94/ 13808 A3 6/ 1994 US 2007/0154476 A1 Jul. 5, 2007 WO WO-94/20625 A1 9/1994 WO WO-96/22788 A1 8/1996 Related US. Application Data WO WO-97/03687 A1 2/1997 (63) Continuation of application No. PCT/US2005/ WO WO-99/38525 A1 8/1999 009967, ?led on Mar. 23, 2005. -

Emerging Roles of Lymphatic Endothelium in Regulating Adaptive Immunity
Emerging roles of lymphatic endothelium in regulating adaptive immunity Catherine M. Card, … , Shann S. Yu, Melody A. Swartz J Clin Invest. 2014;124(3):943-952. https://doi.org/10.1172/JCI73316. Review Series Emerging research on the roles of stromal cells in modulating adaptive immune responses has included a new focus on lymphatic endothelial cells (LECs). LECs are presumably the first cells that come into direct contact with peripheral antigens, cytokines, danger signals, and immune cells travelling from peripheral tissues to lymph nodes. LECs can modulate dendritic cell function, present antigens to T cells on MHC class I and MHC class II molecules, and express immunomodulatory cytokines and receptors, which suggests that their roles in adaptive immunity are far more extensive than previously realized. This Review summarizes the emergent evidence that LECs are important in maintaining peripheral tolerance, limiting and resolving effector T cell responses, and modulating leukocyte function. Find the latest version: https://jci.me/73316/pdf Review series Emerging roles of lymphatic endothelium in regulating adaptive immunity Catherine M. Card, Shann S. Yu, and Melody A. Swartz Institute of Bioengineering and Swiss Institute for Experimental Cancer Research, School of Life Sciences, École Polytechnique Fédérale de Lausanne, Lausanne, Switzerland. Emerging research on the roles of stromal cells in modulating adaptive immune responses has included a new focus on lymphatic endothelial cells (LECs). LECs are presumably the first cells that come into direct contact with peripheral antigens, cytokines, danger signals, and immune cells travelling from peripheral tissues to lymph nodes. LECs can modulate dendritic cell function, present antigens to T cells on MHC class I and MHC class II molecules, and express immunomodulatory cytokines and receptors, which suggests that their roles in adaptive immunity are far more extensive than previously realized. -

Fax: 800-863-7041 E-Mail: Info
Page Part# Description Page Part# Description BUNN CECILWARE 160 B22300.750 FLOW CNTRL W/SCREEN .750 167 CD61A CAP, DISPENSE 163 B23721.0000 SCREEN, STRAINER 167 CD63A CHAMBER, WHIPPER MIXING 159 B23799.1 CORD, POWER 6’ 12/3 50-20P 167 CD64A BLADE, WHIPPER 162 B24331 O-RING 167 CD65A CHAMBER, MOUNT WITH SEAL 162 B24733 O-RING CAPPUCCINO 168 CD66A PILLAR MOUNTING PLATE 162 B24733.1 O-RING 168 CD67A MIXING BOWL, SOCKET 163 B25137 RUBBER FOOT .250, 1/4-20 STUD 168 CD68A HOPPER W/BASE 4 LB 163 B25137.1 RUBBER FOOT .480, 1/4-20 STUD 168 CD75A MOTOR, WHIPPER 163 B25137.2 RUBBER FOOT .480, 8/32 STUD 167 CE76A BULB, FLUORESCENT F8T5CW 164 B25732 STEAM COLLECTOR 167 CE82A BULB, FLUORESCENT 18 WT 158 B25733 CHAMBER, MIXING 168 D017A FAUCET, URN CHROME/BLK HDL 158 B25734 CHAMBER, WHIPPING 168 K355Q PROBE, WATER LEVEL 159 B25736 DISPENSE TIP 168 K402Q PROBE, WATER LEVEL 161 B25902 FROTHER 168 K695Q SENSOR, DUAL LIQUID LEVEL 159 B25903 ELBOW, EJECTOR 167 L042A BULB, FLOURESENT 9 WT 163 B25948 RELAY, 120V 169 L266L THERMOASTAT 165 B26116 VALVE, BUNN DISPENSE 169 L299A SWITCH, TOGGLE 166 B26135.1 VALVE, INLET (120V) 168 L396A STARTER, FLUORESCENT FS5 158 B26239 BULB, FLOURESCENT F8T5CW 167 L398A CNTRL BRD LEVEL 163 B26359 RECEPTACLE, WHIPPER CHAMBER 168 L455A SWITCH, DISPENSE 161 B26504 HINGE, ADJUSTABLE 169 L462A VALVE, INLET CECILWARE 162 B26528 LEG, ADJUSTABLE 4” 3/8 x 16 169 L467A VALVE, DUMP 162 B26528.1 LEG, ADJUSTABLE 1/4 - 20 169 L499A SWITCH, FLOAT 160 B26685 FAUCET, TEA FOR GPR 169 L561A VALVE, DISPENSE 165 B27370 VALVE, DISPENSE 168 L643A -

Extracellular Vesicles As Potential Biomarkers of Acute Graft-Vs.-Host-Disease
AperTO - Archivio Istituzionale Open Access dell'Università di Torino Extracellular vesicles as potential biomarkers of acute graft-vs.-host-disease This is a pre print version of the following article: Original Citation: Availability: This version is available http://hdl.handle.net/2318/1647246 since 2017-10-02T12:01:38Z Published version: DOI:10.1038/leu.2017.277 Terms of use: Open Access Anyone can freely access the full text of works made available as "Open Access". Works made available under a Creative Commons license can be used according to the terms and conditions of said license. Use of all other works requires consent of the right holder (author or publisher) if not exempted from copyright protection by the applicable law. (Article begins on next page) 11 October 2021 Accepted Article Preview: Published ahead of advance online publication Extracellular vesicles as potential biomarkers of acute graft-vs.- host-disease G Lia, L Brunello, S Bruno, A Carpanetto, P Omede` ,M Festuccia, L Tosti, E Maffini, L Giaccone, M Arpinati, G Ciccone, M Boccadoro, A Evangelista, G Camussi, B Bruno Cite this article as: G Lia, L Brunello, S Bruno, A Carpanetto, P Omede` ,M Festuccia, L Tosti, E Maffini, L Giaccone, M Arpinati, G Ciccone, M Boccadoro, A Evangelista, G Camussi, B Bruno, Extracellular vesicles as potential biomarkers of acute graft-vs.-host-disease, Leukemia accepted article preview 30 August 2017; doi: 10.1038/leu.2017.277. This is a PDF file of an unedited peer-reviewed manuscript that has been accepted for publication. NPG are providing this early version of the manuscript as a service to our customers.