Top Six Reasons Why Your Shoulder Pain Isn't Going Away by Pat Schuh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Complex Regional Pain Syndrome Type I (Shoulder-Hand Syndrome) in an Elderly Patient After Open Cardiac Surgical Intervention; a Case Report
Eastern Journal of Medicine 16 (2011) 56-58 L. Ediz et al / CRPS type I after open cardiac Surgery Case Report Complex regional pain syndrome type I (shoulder-hand syndrome) in an elderly patient after open cardiac surgical intervention; a case report Levent Ediza*, Mehmet Fethi Ceylanb , Özcan Hıza, İbrahim Tekeoğlu c a Department of Physical Medicine and Rehabilitation, Yüzüncü Yıl University Medical Faculty, Van, Turkey b Department of Orthopaedics and Traumatology,Yüzüncü Yıl University Medical Faculty, Van, Turkey c Department of Rheumatology, Yüzüncü Yıl University Medical Faculty, Van, Turkey Abstract. We described the first case report in the literature who developed Complex Regional Pain Syndrome (CRPS type I) symptoms in his right shoulder and right hand within 15 days after open cardiac surgery and discussed shoulder-hand syndrome (CRPS type I) and frozen shoulder diagnosis along with the reasons of no report of CRPS type I in these patients. We also speculated whether frozen shoulder seen in postthoracotomy and postcardiac surgery patients might be CRPS type I in fact. Key words: Complex regional pain syndrome, cardiac surgery, frozen shoulder 1. Introduction Improper patient positioning, muscle division, perioperative nerve injury, rib spreading, and Complex Regional Pain Syndrome (CRPS) is consequent postoperative pain influence the complication of injuries which is seen at the patient's postoperative shoulder function and distal end of the affected area characterized by quality of life (5). In a study Tuten HR et al pain, allodyni, hyperalgesia, edema, abnormal retrospectively evaluated for the incidence of vasomotor and sudomotor activity, movement adhesive capsulitis of the shoulder of two disorders, joint stiffness, regional osteopenia, and hundred fourteen consecutive male cardiac dystrophic changes in soft tissue (1,2). -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Early Passive Motion After Surgery
www.western -ortho.com www.denvershoulder.com Early Passive Motion after Shoulder Surgery Passive motion involves someone else moving the affected arm through the motion described. Or, in the case of elbow flexion/extension, you can use your opposite (non-affected arm) to move through the motion. Do 5 repetitions of each stretch 3 times per day. When you feel a slight ‘tightness’ with your arm in the position diagrammed, hold that position for 30 seconds. If lying down is difficult, the stretches can be done while seated. Shoulder Flexion Support arm at the wrist and elbow. With the thumb pointed forward, gently bring the arm up and forward then back to the side. Shoulder Abduction Support arm at wrist and elbow. With the thumb pointed away from the body and palm up, gently bring the arm out to the side. www.western -ortho.com www.denvershoulder.com Shoulder Internal/External Rotation Support arm at wrist and elbow. With the elbow at the side and bent to a 90 degree angle, gently rotate the hand away from the body down toward the table the individual is lying on. Elbow Flexion/Extension Forearm Pronation/Supination Grasp the wrist of your affected arm with your unaffected With your elbow and forearm supported on a table, hand. With your affected elbow against your side and your gently turn forearm so your palm is down, then turn palm up, gently bend and straighten your elbow. forearm so your palm is up. This can be done actively (without assistance from your other hand). . -

Nerve Blocks for Surgery on the Shoulder, Arm Or Hand
The Association of Regional The Royal College of Anaesthetists of Great Anaesthesia – Anaesthetists Britain and Ireland United Kingdom Nerve blocks for surgery on the shoulder, arm or hand Information for patients and families www.rcoa.ac.uk/patientinfo First edition 2015 This leaflet is for anyone who is thinking about having a nerve block for an operation on the shoulder, arm or hand. It will be of particular interest to people who would prefer not to have a general anaesthetic. The leaflet has been written with the help of patients who have had a nerve block for their operation. You can find more information leaflets on the website www.rcoa.ac.uk/patientinfo. The leaflets may also be available from the anaesthetic department or pre-assessment clinic in your hospital. The website includes the following: ■ Anaesthesia explained (a more detailed booklet). ■ You and your anaesthetic (a shorter summary). ■ Your spinal anaesthetic. ■ Anaesthetic choices for hip or knee replacement. ■ Epidural pain relief after surgery. ■ Local anaesthesia for your eye operation. ■ Your child’s general anaesthetic. ■ Your anaesthetic for major surgery with planned high dependency care afterwards. ■ Your anaesthetic for a broken hip. Risks associated with your anaesthetic This is a collection of 14 articles about specific risks associated with having an anaesthetic or an anaesthetic procedure. It supplements the patient information leaflets listed above and is available on the website: www.rcoa.ac.uk/patients-and-relatives/risks. Throughout this leaflet and others in the series, we have used this symbol to highlight key facts. 2 NERVE BLOCKS FOR SURGERY ON THE SHOULDER, ARM OR HAND Brachial plexus block? The brachial plexus is the group of nerves that lies between your neck and your armpit. -

GLOSSARY of MEDICAL and ANATOMICAL TERMS
GLOSSARY of MEDICAL and ANATOMICAL TERMS Abbreviations: • A. Arabic • abb. = abbreviation • c. circa = about • F. French • adj. adjective • G. Greek • Ge. German • cf. compare • L. Latin • dim. = diminutive • OF. Old French • ( ) plural form in brackets A-band abb. of anisotropic band G. anisos = unequal + tropos = turning; meaning having not equal properties in every direction; transverse bands in living skeletal muscle which rotate the plane of polarised light, cf. I-band. Abbé, Ernst. 1840-1905. German physicist; mathematical analysis of optics as a basis for constructing better microscopes; devised oil immersion lens; Abbé condenser. absorption L. absorbere = to suck up. acervulus L. = sand, gritty; brain sand (cf. psammoma body). acetylcholine an ester of choline found in many tissue, synapses & neuromuscular junctions, where it is a neural transmitter. acetylcholinesterase enzyme at motor end-plate responsible for rapid destruction of acetylcholine, a neurotransmitter. acidophilic adj. L. acidus = sour + G. philein = to love; affinity for an acidic dye, such as eosin staining cytoplasmic proteins. acinus (-i) L. = a juicy berry, a grape; applied to small, rounded terminal secretory units of compound exocrine glands that have a small lumen (adj. acinar). acrosome G. akron = extremity + soma = body; head of spermatozoon. actin polymer protein filament found in the intracellular cytoskeleton, particularly in the thin (I-) bands of striated muscle. adenohypophysis G. ade = an acorn + hypophyses = an undergrowth; anterior lobe of hypophysis (cf. pituitary). adenoid G. " + -oeides = in form of; in the form of a gland, glandular; the pharyngeal tonsil. adipocyte L. adeps = fat (of an animal) + G. kytos = a container; cells responsible for storage and metabolism of lipids, found in white fat and brown fat. -

5 Common Causes of Shoulder Pain
5 Common Causes of Shoulder Pain Leslie B. Vidal, M.D. Orthopedic Associates, LLC 303-321-6600 Rotator Cuff Syndrome: Inflammation of rotator cuff tendons and subacromial bursitis, can proceed rotator cuff tear. History: Insidious onset of anterior and lateral shoulder pain, worse with reaching overhead and behind (putting dishes away in upper cabinet, reaching into the back seat of car). Patients often report positional night pain. Symptoms may be partially alleviated with NSAIDs and ice. Exam: Pain at the extremes of shoulder range of motion, no significant loss of motion. Strength is intact although may be slightly guarded due to pain. Impingement tests positive. Treatment: NSAIDs, Physical Therapy for scapular stabilizing exercises and rotator cuff strengthening. When to refer: If no improvement with 6 weeks of NSAIDs and PT, consider MRI to rule out rotator cuff tear. Consider referral to shoulder surgeon for ultrasound guided subacromial cortisone injection. Surgery can be considered for refractory cases. If there is significant loss of motion (see adhesive capsulitis) or weakness (may have rotator cuff tear), consider immediate referral as NSAIDs and PT may not be as effective in these cases. A history of trauma resulting in shoulder weakness should lead to a prompt referral to a shoulder surgeon, as this may represent an acute RCT. Instability: Subluxation or dislocation of the glenohumeral joint. Can be acute and traumatic and unidirectional; or recurrent, atraumatic and multidirectional. History: Patient may report a traumatic injury to the shoulder resulting in a dislocation requiring a reduction maneuver; or a more nonspecific history of shoulder pain and sense of instability that the patient is able to self-reduce. -

ANTERIOR SHOULDER TIGHTNESS Home Exercises
ANTERIOR SHOULDER TIGHTNESS Home Exercises Shoulder Dysfunction Anterior tightness and periscapular weakness can be contributing factors to shoulder pain and dysfunction. Periscapular weakness occurs when the muscles that attach to the shoulder blade fail to provide adequate support for the shoulder complex as a whole. Loss of balance between flexibility and strength can lead to scapular dyskinesia. Scapular dyskinesia is recognized as an alteration of normal shoulder movement. How does shoulder dysfunction occur? Anterior tightness, periscapular weakness, and scapular dyskinesia can be the result of trauma, repetitive use, and/ or poor posture. Much of life happens in front of us. Computers, phones, cooking, and sitting subject us to more of a forward flexed posture. If trauma occurs, our immediate response is to protect our shoulders by posturing in a forward flexed position. Over time, this position contributes to shortening of the chest muscles and lengthening and weakening of the back muscles. Ultimately, this also leads to decreased spacing at the anterior shoulder joint where the rotator cuff muscles can then be irritated, frayed, or even torn. The goal of therapy is to restore normal movement of the shoulder through strengthening, stretching, and postural correction. Poor Posture Good Posture • Shoulders rounded forward • Shoulders pulled back and down • Ears lined up in front of shoulders • Ears lined up with tip of shoulder • Chin forward and down • Chin pulled back and in • Spine is unsupported and compressed • Spine is supported and lengthened • Belly pushed out • Belly is pulled in 1 oahct.com Poor Posture Good Posture • Head tipped forward and down • Head level and chin pulled back and in • Upper back rounded forward • Upright posture • Shoulders rounded forward • Shoulders pulled back and down • Body leans toward the device • Device is brought toward eye level PECTORALIS DOORWAY STRETCH - LOW While standing in a doorway, place your arm downward on the door frame and lean in until a stretch is felt along the front of your chest and/or shoulder. -

Rotator Cuff Tears
OrthoInfo Basics Rotator Cuff Tears What is a rotator cuff? One of the Your rotator cuff helps you lift your arm, rotate it, and reach up over your head. most common middle-age It is made up of muscles and tendons in your shoulder. These struc- tures cover the head of your upper arm bone (humerus). This “cuff” complaints is holds the upper arm bone in the shoulder socket. shoulder pain. Rotator cuff tears come in all shapes and sizes. They typically occur A frequent in the tendon. source of that Partial tears. Many tears do not completely sever the soft tissue. Full thickness tears. A full or "complete" tear will split the soft pain is a torn tissue into two, sometimes detaching the tendon from the bone. rotator cuff. Rotator Cuff Bursa A torn rotator cuff will Tendon Clavicle (Collarbone) Humerus weaken your shoulder. (Upper Arm) This means that many Normal shoulder anatomy. daily activities, like combing your hair or Scapula getting dressed, may (Shoulder Blade) become painful and difficult to do. Rotator Cuff Tendon A complete tear of the rotator cuff tendon. 1 OrthoInfo Basics — Rotator Cuff Tears What causes rotator cuff tears? There are two main causes of rotator cuff repeating the same shoulder motions again and tears: injury and wear. again. Injury. If you fall down on your outstretched This explains why rotator cuff tears are most arm or lift something too heavy with a jerking common in people over 40 who participate in motion, you could tear your rotator cuff. This activities that have repetitive overhead type of tear can occur with other shoulder motions. -

Chapter 5 the Shoulder Joint
The Shoulder Joint • Shoulder joint is attached to axial skeleton via the clavicle at SC joint • Scapula movement usually occurs with movement of humerus Chapter 5 – Humeral flexion & abduction require scapula The Shoulder Joint elevation, rotation upward, & abduction – Humeral adduction & extension results in scapula depression, rotation downward, & adduction Manual of Structural Kinesiology – Scapula abduction occurs with humeral internal R.T. Floyd, EdD, ATC, CSCS rotation & horizontal adduction – Scapula adduction occurs with humeral external rotation & horizontal abduction © McGraw-Hill Higher Education. All rights reserved. 5-1 © McGraw-Hill Higher Education. All rights reserved. 5-2 The Shoulder Joint Bones • Wide range of motion of the shoulder joint in • Scapula, clavicle, & humerus serve as many different planes requires a significant attachments for shoulder joint muscles amount of laxity – Scapular landmarks • Common to have instability problems • supraspinatus fossa – Rotator cuff impingement • infraspinatus fossa – Subluxations & dislocations • subscapular fossa • spine of the scapula • The price of mobility is reduced stability • glenoid cavity • The more mobile a joint is, the less stable it • coracoid process is & the more stable it is, the less mobile • acromion process • inferior angle © McGraw-Hill Higher Education. All rights reserved. 5-3 © McGraw-Hill Higher Education. All rights reserved. From Seeley RR, Stephens TD, Tate P: Anatomy and physiology , ed 7, 5-4 New York, 2006, McGraw-Hill Bones Bones • Scapula, clavicle, & humerus serve as • Key bony landmarks attachments for shoulder joint muscles – Acromion process – Humeral landmarks – Glenoid fossa • Head – Lateral border • Greater tubercle – Inferior angle • Lesser tubercle – Medial border • Intertubercular groove • Deltoid tuberosity – Superior angle – Spine of the scapula © McGraw-Hill Higher Education. -

Shoulder Joint - Upper Limb
Shoulder Joint - Upper Limb Dr. Brijendra Singh Prof & Head Department of Anatomy AIIMS Rishikesh Learning objectives •Anatomy of shoulder joint •Formation , type & components •Rotator cuff •Relations /nerve & blood supply •Movements & muscles producing them •Dislocations /nerve injuries Articulation - Rounded head of humerus & Shallow , glenoid cavity of scapula. Glenoid cavity • Articular surfaces are covered by articular - hyaline cartilage. • Glenoid cavity is deepened by fibro cartilaginous rim called glenoid labrum. Synovial membrane •lines fibrous capsule & attached to margins of the cartilage covering the articular surfaces. •forms a tubular sheath around the tendon of the long head of biceps brachii. •It extends through anterior wall of capsule to form subscapularis bursa beneath subscapularis muscle. Synovial membrane Musculotendinious/Rotator cuff •Supraspinatus – superiorly •Infraspinatus & Teres minor- posteriorly •Subscapularis – anteriorly •Long head of triceps – inferiorly ( axillary n & post circumflex humeral artery – lax and least supported) – •most common dislocations – Inferiorly axillary n palsy –loss of abduction NERVE SUPPLY of Shoulder joint NERVE SUPPLY of Shoulder joint 1. axillary n 2. suprascapular n & 3. lateral pectoral nerve. Shoulder joint - spaces Quadrangular space Triangular space •Sup - teres minor •Sup – teres major •Inf - teres major •Medially- long head •Medially - long head of of triceps triceps •Laterally – •Laterally – lateral head triceps(humerus) of triceps (humerus) •Contents – in spiral •Contents -
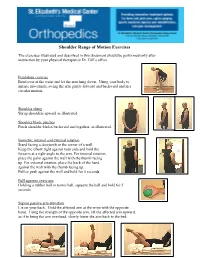
Shoulder Range of Motion Exercises
Shoulder Range of Motion Exercises The exercises illustrated and described in this document should be performed only after instruction by your physical therapist or Dr. Gill’s office. Pendulum exercise Bend over at the waist and let the arm hang down. Using your body to initiate movement, swing the arm gently forward and backward and in a circular motion. Shoulder shrug Shrug shoulders upward as illustrated. Shoulder blade pinches Pinch shoulder blades backward and together, as illustrated. Isometric internal and external rotation Stand facing a doorjamb or the corner of a wall. Keep the elbow tight against your side and hold the forearm at a right angle to the arm. For internal rotation, place the palm against the wall with the thumb facing up. For external rotation, place the back of the hand against the wall with the thumb facing up. Pull or push against the wall and hold for 5 seconds Ball squeeze exercises Holding a rubber ball or tennis ball, squeeze the ball and hold for 5 seconds Supine passive arm elevation Lie on your back. Hold the affected arm at the wrist with the opposite hand. Using the strength of the opposite arm, lift the affected arm upward, as if to bring the arm overhead, slowly lower the arm back to the bed. St. Elizabeth's Medical Center Orthopedics Department 736 Cambridge Street Brighton, MA 02135 www.semc.org/ortho Supine Passive Forward Flexion Lie on your back. Holding a stick in both hands about shoulder width apart, raise the involved arm with the help of the uninvolved arm up and then backward as if to reach overhead. -

Anatomy, Biomechanics, Physiology, Diagnosis and Treatment of Teres
ANATOMY, BIOMECHANICS, PHYSIOLOGY, DIAGNOSIS AND TREATMENT OF TERES MAJOR STRAINS IN THE CANINE Laurie Edge-Hughes, BScPT, CAFCI, CCRT Four Leg Rehabilitation Therapy & The Canine Fitness Centre Ltd, Calgary, AB, Canada The Canadian Horse and Animal Physical Rehabilitation Assn. The Animal Rehab Institute, Loxahatchee, Florida, USA BACKGROUND The canine shoulder apparatus is unique as compared to other canine joints and also when compared to the human shoulder. When compared to the hind limb it is interesting to note that the front limb has no boney attachment to the axial skeleton in that there is no clavicle in the canine. This factor alone means that muscular strength and co-ordination is of utmost importance to full functioning of the front limb. When compared to the human shoulder, one obvious difference is that the shoulder joint is a weight bearing joint. The orientation of the canine scapula and humerus is vertical and the weight distribution is 60 to 65 % on the front legs and 40 – 35% on the hind legs. Essentially dogs are like ‘front wheel drive vehicles’, designed to propel themselves forward by primarily ‘pulling’ from the front end. This is why identification and treatment of front limb muscle injuries is critically important for athletic or just high energy dogs who are most prone to injuring shoulder muscles. The teres major muscle is one that is commonly strained, often unidentified and hence not as effectively treated as it could be in the active canine patient. ANATOMY The teres major muscle originates from the caudal angle and caudal edge of the scapula and inserts into the eminence on the proximal 1/3 of the medial surface of the humerus.