Expression, Regulation and Targeting of Receptor Tyrosine Kinases in Esophageal Squamous Cell Carcinoma Manoj Kumar Kashyap1,2* and Omar Abdel-Rahman3
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Novel Mouse Mutant, Chuzhoi, Has Disruption of Ptk7 Protein and Exhibits Defects in Neural Tube, Heart and Lung Development
Paudyal et al. BMC Developmental Biology 2010, 10:87 http://www.biomedcentral.com/1471-213X/10/87 RESEARCH ARTICLE Open Access The novel mouse mutant, chuzhoi, has disruption of Ptk7 protein and exhibits defects in neural tube, heart and lung development and abnormal planar cell polarity in the ear Anju Paudyal1, Christine Damrau1, Victoria L Patterson1, Alexander Ermakov1,2, Caroline Formstone3, Zuzanna Lalanne1,4, Sara Wells5, Xiaowei Lu6, Dominic P Norris1, Charlotte H Dean1, Deborah J Henderson7, Jennifer N Murdoch1,8* Abstract Background: The planar cell polarity (PCP) signalling pathway is fundamental to a number of key developmental events, including initiation of neural tube closure. Disruption of the PCP pathway causes the severe neural tube defect of craniorachischisis, in which almost the entire brain and spinal cord fails to close. Identification of mouse mutants with craniorachischisis has proven a powerful way of identifying molecules that are components or regulators of the PCP pathway. In addition, identification of an allelic series of mutants, including hypomorphs and neomorphs in addition to complete nulls, can provide novel genetic tools to help elucidate the function of the PCP proteins. Results: We report the identification of a new N-ethyl-N-nitrosourea (ENU)-induced mutant with craniorachischisis, which we have named chuzhoi (chz). We demonstrate that chuzhoi mutant embryos fail to undergo initiation of neural tube closure, and have characteristics consistent with defective convergent extension. These characteristics include a broadened midline and reduced rate of increase of their length-to-width ratio. In addition, we demonstrate disruption in the orientation of outer hair cells in the inner ear, and defects in heart and lung development in chuzhoi mutants. -

PTK7 Expression in Triple-Negative Breast Cancer
ANTICANCER RESEARCH 33: 3759-3764 (2013) PTK7 Expression in Triple-negative Breast Cancer BEYHAN ATASEVEN1,2, REGINA ANGERER1, RONALD KATES3, ANGELA GUNESCH1, PJOTR KNYAZEV4, BERNHARD HÖGEL5, CLEMENS BECKER5, WOLFGANG EIERMANN6 and NADIA HARBECK7 1Department of Gynecology and Obstetrics, Red Cross Women’s Hospital, Munich, Germany; 2Department of Gynecology and Gynecologic Oncology, Kliniken Essen-Mitte, Evangelische Huyssens-Stiftung, Essen, Germany; 3Breast Center, Department of Gynecology and Obstetrics Maistrasse Campus, Ludwig Maximilian University Munich, Munich, Germany; 4Department of Molecular Biology, Max Planck Institute of Biochemistry, Martinsried, Germany; 5Department of Pathology, Red Cross Women’s Hospital Munich, Munich, Germany; 6Department of Gynecology and Oncology, Interdiscipilnary Oncology Center Munich, Germany; 7Breast Center, Department of Gynecology and Obstetrics, Großhadern Campus, Ludwig Maximilian University Munich, Munich, Germany Abstract. Background: Protein tyrosine kinase-7 (PTK7) immunoglobulin-like loops, a transmenbrane domain and an plays an important role in cancer. Our aim was to evaluate inactive catalytic tyrosine kinase domain (2, 3). PTK7 seems PTK7 in triple-negative breast cancer (TNBC). Materials to be highly involved in the WNT (named after the Drosophilia and Methods: PTK7 Expression was assessed by Wingless (Wg) and the mouse Int-1 genes)-pathways (4), which immunohistochemistry (IHC) in 133 patients with TNBC. again represent key pathways for epithelial mesenchymal Expression levels were correlated with clinicopathological transition (EMT) and play important roles in cancer (5-8). A features and survival, taking chemotherapy into account. potential impact of PTK7 expression has been studied in Results: Positive PTK7 expression was detected in 28.6% of several malignancies, including colon, lung, gastric and breast tumors. In the total population, no significant difference was cancer, acute myeloid leukemia and liposarcoma (9-15). -

Ptk7-Deficient Mice Have Decreased Hematopoietic Stem Cell Pools As a Result of Deregulated Proliferation and Migration
Ptk7-Deficient Mice Have Decreased Hematopoietic Stem Cell Pools as a Result of Deregulated Proliferation and Migration This information is current as Anne-Catherine Lhoumeau, Marie-Laure Arcangeli, Maria of September 24, 2021. De Grandis, Marilyn Giordano, Jean-Christophe Orsoni, Frédérique Lembo, Florence Bardin, Sylvie Marchetto, Michel Aurrand-Lions and Jean-Paul Borg J Immunol 2016; 196:4367-4377; Prepublished online 18 April 2016; Downloaded from doi: 10.4049/jimmunol.1500680 http://www.jimmunol.org/content/196/10/4367 Supplementary http://www.jimmunol.org/content/suppl/2016/04/16/jimmunol.150068 http://www.jimmunol.org/ Material 0.DCSupplemental References This article cites 55 articles, 24 of which you can access for free at: http://www.jimmunol.org/content/196/10/4367.full#ref-list-1 Why The JI? Submit online. by guest on September 24, 2021 • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright -
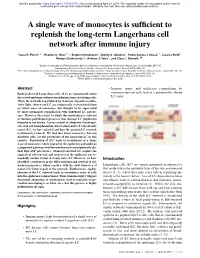
A Single Wave of Monocytes Is Sufficient to Replenish the Long-Term
bioRxiv preprint doi: https://doi.org/10.1101/617514; this version posted April 24, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. A single wave of monocytes is sufficient to replenish the long-term Langerhans cell network after immune injury Ivana R. Ferrer1,2,a, Heather C. West1,2,a, Stephen Henderson2, Dmitry S. Ushakov3, Pedro Santos e Sousa1,2, Jessica Strid4, Ronjon Chakraverty1,2, Andrew J. Yates5, and Clare L. Bennett1,2 1Institute of Immunity and Transplantation, Division of Infection and Immunity, University College London, London NW3 2PF, UK 2Haematology, Division of Cancer Studies, University College London, London WC1E 6DD, UK. 3Peter Gorer Department of Immunobiology, School of Immunology and Microbial Sciences, King’s College London, New Hunt’s House, Newcomen St, London SE1 1UL, UK 4Division of Immunology and Inflammation, Imperial College London, Hammersmith campus, London W12 0NN, UK. 5Department of Pathology and Cell Biology, Columbia University Medical Center, New York, NY10032, USA. aThese authors contributed equally to this work Abstract • Immune injury and inefficient repopulation by Embryo-derived Langerhans cells (eLC) are maintained within monocyte-derived cells lead to a permanently altered the sealed epidermis without contribution from circulating cells. LC niche. When the network is perturbed by transient exposure to ultra- violet light, short-term LC are temporarily reconstituted from an initial wave of monocytes, but thought to be superseded by more permanent repopulation with undefined LC precur- sors. However, the extent to which this mechanism is relevant to immune-pathological processes that damage LC population integrity is not known. -

Ponatinib Shows Potent Antitumor Activity in Small Cell Carcinoma of the Ovary Hypercalcemic Type (SCCOHT) Through Multikinase Inhibition Jessica D
Published OnlineFirst February 9, 2018; DOI: 10.1158/1078-0432.CCR-17-1928 Cancer Therapy: Preclinical Clinical Cancer Research Ponatinib Shows Potent Antitumor Activity in Small Cell Carcinoma of the Ovary Hypercalcemic Type (SCCOHT) through Multikinase Inhibition Jessica D. Lang1,William P.D. Hendricks1, Krystal A. Orlando2, Hongwei Yin1, Jeffrey Kiefer1, Pilar Ramos1, Ritin Sharma3, Patrick Pirrotte3, Elizabeth A. Raupach1,3, Chris Sereduk1, Nanyun Tang1, Winnie S. Liang1, Megan Washington1, Salvatore J. Facista1, Victoria L. Zismann1, Emily M. Cousins4, Michael B. Major4, Yemin Wang5, Anthony N. Karnezis5, Aleksandar Sekulic1,6, Ralf Hass7, Barbara C. Vanderhyden8, Praveen Nair9, Bernard E. Weissman2, David G. Huntsman5,10, and Jeffrey M. Trent1 Abstract Purpose: Small cell carcinoma of the ovary, hypercalcemic type three SWI/SNF wild-type ovarian cancer cell lines. We further (SCCOHT) is a rare, aggressive ovarian cancer in young women identified ponatinib as the most effective clinically approved that is universally driven by loss of the SWI/SNF ATPase subunits RTK inhibitor. Reexpression of SMARCA4 was shown to confer SMARCA4 and SMARCA2. A great need exists for effective targeted a 1.7-fold increase in resistance to ponatinib. Subsequent therapies for SCCOHT. proteomic assessment of ponatinib target modulation in Experimental Design: To identify underlying therapeutic vul- SCCOHT cell models confirmed inhibition of nine known nerabilities in SCCOHT, we conducted high-throughput siRNA ponatinib target kinases alongside 77 noncanonical ponatinib and drug screens. Complementary proteomics approaches pro- targets in SCCOHT. Finally, ponatinib delayed tumor dou- filed kinases inhibited by ponatinib. Ponatinib was tested for bling time 4-fold in SCCOHT-1 xenografts while reducing efficacy in two patient-derived xenograft (PDX) models and one final tumor volumes in SCCOHT PDX models by 58.6% and cell-line xenograft model of SCCOHT. -
Molecular Regulation of Janus Kinases (Jaks) Focus on the Pseudokinase Domain
JUULI RAIVOLA Molecular Regulation of Janus Kinases (JAKs) Focus on the Pseudokinase Domain Tampere University Dissertations 366 7DPSHUH8QLYHUVLW\'LVVHUWDWLRQV -88/,5$,92/$ 0ROHFXODU5HJXODWLRQRI-DQXV.LQDVHV -$.V )RFXVRQWKH3VHXGRNLQDVH'RPDLQ $&$'(0,&',66(57$7,21 7REHSUHVHQWHGZLWKWKHSHUPLVVLRQRI WKH)DFXOW\RI0HGLFLQHDQG+HDOWK7HFKQRORJ\ RI7DPSHUH8QLYHUVLW\ IRUSXEOLFGLVFXVVLRQLQ$UYRYlpön NDWX7DPSHUH RQ-DQXDU\DWR¶FORFN $&$'(0,&',66(57$7,21 7DPSHUH8QLYHUVLW\)DFXOW\RI0HGLFLQHDQG+HDOWK7HFKQRORJ\ )LQODQG Responsible 3URIHVVRU2OOL6LOYHQQRLQHQ supervisor 7DPSHUH8QLYHUVLW\ and Custos )LQODQG Pre-examiners 3URIHVVRU-DUL<OlQQH 'RFHQW9LYHN6KDUPD 8QLYHUVLW\RI-\YlVN\Ol 8QLYHUVLW\RI+HOVLQNL )LQODQG )LQODQG Opponent 3URIHVVRU6WHIDQ1&RQVWDQWLQHVFX 8QLYHUVLWpFDWKROLTXHGH/RXYDLQ %HOJLXP 7KHRULJLQDOLW\RIWKLVWKHVLVKDVEHHQFKHFNHGXVLQJWKH7XUQLWLQ2ULJLQDOLW\&KHFN VHUYLFH &RS\ULJKWDXWKRU &RYHUGHVLJQ5RLKX,QF ,6%1 SULQW ,6%1 SGI ,661 SULQW ,661 SGI KWWSXUQIL851,6%1 3XQD0XVWD2\±<OLRSLVWRSDLQR -RHQVXX To my Family i ii TIIVISTELMÄ JAK-STAT-(vapaasti suomennettuna Janus-kinaasi - signaalinvälittäjä ja transkriptioaktivaattori) reitti välittää yli 50 sytokiinin signaaleja, jotka säätelevät solun selviytymistä, jakaantumista, migraatiota, geeniekspressiota, sekä muita elintärkeitä prosesseja kuten immuunivastetta. Siksi myös virheellisesti toimiva JAK- STAT signalointi aikaansaa vakavia seurauksia. Aktivoivat JAK-mutaatiot aiheuttavat hematologisia syöpiä sekä myeloproliferatiivisia tauteja, kun taas vajaatoimintainen JAK-signalointi voi johtaa muun muassa vakavaan -

Targeting Cancer Stem Cells in Triple-Negative Breast Cancer
Review Targeting Cancer Stem Cells in Triple‐Negative Breast Cancer So‐Yeon Park 1,2, Jang‐Hyun Choi 1 and Jeong‐Seok Nam 1,2,* 1 School of Life Sciences, Gwangju Institute of Science and Technology, Gwangju 61005, Korea 2 Cell Logistics Research Center, Gwangju Institute of Science and Technology, Gwangju 61005, Korea * Correspondence: [email protected]; Tel.: +82‐62‐715‐2893; Fax: +82‐62‐715‐2484 Received: 11 June 2019; Accepted: 04 July 2019; Published: 9 July 2019 Abstract: Triple‐negative breast cancer (TNBC) is a highly aggressive form of breast cancer that lacks targeted therapy options, and patients diagnosed with TNBC have poorer outcomes than patients with other breast cancer subtypes. Emerging evidence suggests that breast cancer stem cells (BCSCs), which have tumor‐initiating potential and possess self‐renewal capacity, may be responsible for this poor outcome by promoting therapy resistance, metastasis, and recurrence. TNBC cells have been consistently reported to display cancer stem cell (CSC) signatures at functional, molecular, and transcriptional levels. In recent decades, CSC‐targeting strategies have shown therapeutic effects on TNBC in multiple preclinical studies, and some of these strategies are currently being evaluated in clinical trials. Therefore, understanding CSC biology in TNBC has the potential to guide the discovery of novel therapeutic agents in the future. In this review, we focus on the self‐renewal signaling pathways (SRSPs) that are aberrantly activated in TNBC cells and discuss the specific signaling components that are involved in the tumor‐initiating potential of TNBC cells. Additionally, we describe the molecular mechanisms shared by both TNBC cells and CSCs, including metabolic plasticity, which enables TNBC cells to switch between metabolic pathways according to substrate availability to meet the energetic and biosynthetic demands for rapid growth and survival under harsh conditions. -

Protein Tyrosine Kinases: Their Roles and Their Targeting in Leukemia
cancers Review Protein Tyrosine Kinases: Their Roles and Their Targeting in Leukemia Kalpana K. Bhanumathy 1,*, Amrutha Balagopal 1, Frederick S. Vizeacoumar 2 , Franco J. Vizeacoumar 1,3, Andrew Freywald 2 and Vincenzo Giambra 4,* 1 Division of Oncology, College of Medicine, University of Saskatchewan, Saskatoon, SK S7N 5E5, Canada; [email protected] (A.B.); [email protected] (F.J.V.) 2 Department of Pathology and Laboratory Medicine, College of Medicine, University of Saskatchewan, Saskatoon, SK S7N 5E5, Canada; [email protected] (F.S.V.); [email protected] (A.F.) 3 Cancer Research Department, Saskatchewan Cancer Agency, 107 Wiggins Road, Saskatoon, SK S7N 5E5, Canada 4 Institute for Stem Cell Biology, Regenerative Medicine and Innovative Therapies (ISBReMIT), Fondazione IRCCS Casa Sollievo della Sofferenza, 71013 San Giovanni Rotondo, FG, Italy * Correspondence: [email protected] (K.K.B.); [email protected] (V.G.); Tel.: +1-(306)-716-7456 (K.K.B.); +39-0882-416574 (V.G.) Simple Summary: Protein phosphorylation is a key regulatory mechanism that controls a wide variety of cellular responses. This process is catalysed by the members of the protein kinase su- perfamily that are classified into two main families based on their ability to phosphorylate either tyrosine or serine and threonine residues in their substrates. Massive research efforts have been invested in dissecting the functions of tyrosine kinases, revealing their importance in the initiation and progression of human malignancies. Based on these investigations, numerous tyrosine kinase inhibitors have been included in clinical protocols and proved to be effective in targeted therapies for various haematological malignancies. -

Effects of Fyn-Related-Kinase Activity on Breast
EFFECTS OF FYN-RELATED-KINASE ACTIVITY ON BREAST CANCER CELL PROLIFERATION, MIGRATION, INVASION AND COLONY FORMATION A Thesis Submitted to the College of Graduate Studies and Research In Partial Fulfillment of the Requirements For the Degree of Master of Science In the Department of Biochemistry University of Saskatchewan Saskatoon By Chenlu Dai Copyright Chenlu Dai, January, 2015. All rights reserved. Permission to Use In presenting this thesis in partial fulfilment of the requirements for a Postgraduate degree from the University of Saskatchewan, I agree that the Libraries of this University may make it freely available for inspection. I further agree that permission for copying of this thesis in any manner, in whole or in part, for scholarly purposes may be granted by the professor or professors who supervised my thesis work or, in their absence, by the Head of the Department or the Dean of the College in which my thesis work was completed. It is understood that any copying or publication or use of this thesis or parts thereof financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and to the University of Saskatchewan in any scholarly use which may be made of any material in my thesis. Requests for permission to copy or to make other use of material in this thesis in whole or part should be addressed to: Head of the Department of Biochemistry University of Saskatchewan Saskatoon, Saskatchewan, S7N 5E5 i ABSTRACT The human Fyn-related kinase (FRK) is a member of subfamily of Src-related kinases family. -

PTK7-Src Signaling at Epithelial Cell Contacts Mediates Spatial Organization of Actomyosin and Planar Cell Polarity
Developmental Cell Article PTK7-Src Signaling at Epithelial Cell Contacts Mediates Spatial Organization of Actomyosin and Planar Cell Polarity Anna Andreeva,1,4 Jianyi Lee,1,4 Madhura Lohia,2 Xiaoji Wu,3,5 Ian G. Macara,2,6 and Xiaowei Lu1,* 1Department of Cell Biology, P.O. Box 800732, University of Virginia, Charlottesville, VA 22908, USA 2Department of Microbiology, Center for Cell Signaling, University of Virginia, Charlottesville, VA 22908, USA 3School of Life Sciences, Peking University, Beijing, China, 100871 4Co-first authors 5Present address: PhD Program in Biological and Biomedical Sciences, Harvard Medical School, Boston, MA 02115, USA 6Present address: Department of Cell and Developmental Biology, Vanderbilt University Medical Center, Nashville, TN 37232, USA *Correspondence: [email protected] http://dx.doi.org/10.1016/j.devcel.2014.02.008 SUMMARY of the cell apex, results in bending and invagination of an epithe- lial cell sheet (Martin et al., 2009; Sawyer et al., 2010). During Actomyosin contractility plays a key role in tissue embryonic axis elongation in Drosophila and Xenopus, aniso- morphogenesis. During mammalian development, tropic contractile forces mediate directional cell intercalation PTK7 regulates epithelial morphogenesis and planar and convergent extension (Blankenship et al., 2006; Rauzi cell polarity (PCP) through modulation of actomyosin et al., 2010; Skoglund et al., 2008). However, mechanisms contractility, but the underlying mechanism is un- underlying precise spatial and temporal control of actomyosin known. Here, we show that PTK7 interacts with the assembly on a tissue scale remain poorly understood. Emerging evidence indicates that planar cell polarity (PCP) tyrosine kinase Src and stimulates Src signaling signaling plays an important role in spatial regulation of actomy- along cell-cell contacts. -

Catalytically Defective Receptor Protein Tyrosine Kinase PTK7 Enhances
www.impactjournals.com/oncotarget/ Oncotarget, Vol. 7, No. 45 Research Paper Catalytically defective receptor protein tyrosine kinase PTK7 enhances invasive phenotype by inducing MMP-9 through activation of AP-1 and NF-κB in esophageal squamous cell carcinoma cells Won-Sik Shin1, Yuri Hong1, Hae Won Lee2, Seung-Taek Lee1 1Department of Biochemistry, College of Life Science and Biotechnology, Yonsei University, Seoul, Republic of Korea 2Department of Thoracic Surgery, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Republic of Korea Correspondence to: Seung-Taek Lee, email: [email protected] Keywords: PTK7, MMP-9, NF-κB, AP-1, esophageal squamous cell carcinoma (ESCC) Received: June 04, 2016 Accepted: September 21, 2016 Published: September 28, 2016 ABSTRACT Protein tyrosine kinase 7 (PTK7), a member of the catalytically defective receptor protein tyrosine kinase family, is upregulated in various cancers including esophageal squamous cell carcinoma (ESCC). Here, we have explored the molecular mechanism of PTK7-dependent invasiveness in ESCC cells. PTK7 knockdown reduced gelatin degradation and MMP-9 secretion in cultures of ESCC TE-10 cells, and showed reduced levels of MMP9 mRNA using real-time RT-PCR and luciferase reporter assays. PTK7 knockdown decreased not only phosphorylation of NF-κB, IκB, ERK, and JNK, but also nuclear localization of NF-κB and AP-1 consisting of c-Fos and c-Jun. Activation of AP-1 and NF-κB requires PTK7-mediated activation of tyrosine kinases, including Src. In addition, NF-κB activation by PTK7 involves the PI3K/Akt signaling pathway. PTK7-mediated upregulation of MMP9 was also observed in other ESCC cell lines and in three-dimensional cultures of TE-10 cells. -

Taqman® Human Protein Kinase Array
TaqMan® Gene Signature Arrays TaqMan® Human Protein Kinase Array This array is part of a collection of TaqMan® Gene Signature these kinases are from receptor protein-tyrosine kinase (RPTK) Arrays that enable analysis of hundreds of TaqMan® Gene families: EGFR, InsulinR, PDGFR, VEGFR, FGFR, CCK, NGFR, Expression Assays on a micro fluidic card with minimal effort. HGFR, EPHR, AXL, TIE, RYK, DDR, RET, ROS, LTK, ROR and MUSK. The remaining 15 kinases are Ser/Thr kinases from the Protein kinases are one of the largest families of genes in kinase families: CAMKL, IRAK, Lmr, RIPK and STKR. eukaryotes. They belong to one superfamily containing a eukaryotic protein kinase catalytic domain. The ability of kinases We have also selected assays for 26 non-kinase genes in the to reversibly phosphorylate and regulate protein function Human Protein Kinase Array. These genes are involved in signal has been a subject of intense investigation. Kinases are transduction and mediate protein-protein interaction, transcrip- responsible for most of the signal transduction in eukaryotic tional regulation, neural development and cell adhesion. cells, affecting cellular processes including metabolism, References: angiogenesis, hemopoiesis, apoptosis, transcription and Manning, G., Whyte, D.B., Martinez, R., Hunter, T., and differentiation. Protein kinases are also involved in functioning Sudarsanam, S. 2002. The Protein Kinase Complement of the of the nervous and immune systems, in physiologic responses Human Genome. Science 298:1912–34. and in development. Imbalances in signal transduction due to accumulation of mutations or genetic alterations have Blume-Jensen, P. and Hunter, T. 2001. Oncogenic kinase been shown to result in malignant transformation.