Covidview Week 44, Ending October 31, 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Copy of 2020-2021 Semi-Monthly Calendar.Xlsx
Employee Time Sheet/Leave Sheet Schedule Supervisor Approval Deadline/ Pay Period Employee Submittal Deadline Paper Leave Request Due to HR by 11:59 PM 12 Noon Pay Day Wednesday, July 1, 2020 to Wednesday, July 15, 2020 Thursday, July 16, 2020 Friday, July 17, 2020 Friday, July 31, 2020 Thursday, July 16, 2020 to Friday, July 31, 2020 Monday, August 3, 2020 Tuesday, August 4, 2020 Friday, August 14, 2020 Saturday, August 1, 2020 to Saturday, August 15, 2020 Monday, August 17, 2020 Tuesday, August 18, 2020 Monday, August 31, 2020 Sunday, August 16, 2020 to Monday, August 31, 2020 Tuesday, September 1, 2020 Wednesday, September 2, 2020 Tuesday, September 15, 2020 Tuesday, September 1, 2020 to Tuesday, September 15, 2020 Wednesday, September 16, 2020 Thursday, September 17, 2020 Wednesday, September 30, 2020 Wednesday, September 16, 2020 to Wednesday, September 30, 2020 Thursday, October 1, 2020 Friday, October 2, 2020 Thursday, October 15, 2020 Thursday, October 1, 2020 to Thursday, October 15, 2020 Friday, October 16, 2020 Monday, October 19, 2020 Friday, October 30, 2020 Friday, October 16, 2020 to Saturday, October 31, 2020 Monday, November 2, 2020 Tuesday, November 3, 2020 Friday, November 13, 2020 Sunday, November 1, 2020 to Sunday, November 15, 2020 Monday, November 16, 2020 Tuesday, November 17, 2020 Monday, November 30, 2020 Monday, November 16, 2020 to Monday, November 30, 2020 Tuesday, December 1, 2020 Wednesday, December 2, 2020 Tuesday, December 15, 2020 Tuesday, December 1, 2020 to Tuesday, December 15, 2020 Wednesday, December -

Illinois Weather Trivia for October
Illinois Weather Trivia for October October 1 1890: The U.S. Weather Bureau was established by an act of Congress, and assigned as part of the Department of Agriculture. Weather observations and forecasts were previously issued by the Army Signal Service. October 2 1922: Strong southerly winds brought very warm air from the Gulf region into Illinois. Rockford reached 91 degrees, the all-time warmest temperature recorded during the month of October. The heat wave across the region persisted through the 5th. October 3 1954: A late-season heat wave was found across central Illinois. Champaign's high temperature of 93 degrees established a record for the month of October. Springfield reported a high temperature of 93 degrees, also setting a monthly record, which was tied on the same date in 2006. 2000: A small area of very strong thunderstorms developed in west central Illinois during the early evening hours, and moved into north central Illinois. A predominate gust front developed ahead of these storms, which brought considerable winds across La Salle County. State Police estimated the winds to be 90 mph, maintaining that strength as the gust front moved across the county. Near Oglesby, a semi-tractor trailer was overturned on Interstate 39, and several secondary roads leading to Starved Rock State Park were closed due to downed trees and power lines. Near Ottawa, a $100,000 machine shed was destroyed. October 4 1941: A 4.74 inch deluge of rain marked Springfield's wettest October day on record. Records in Springfield date back to 1879. 1991: Severe thunderstorms moved across parts of central and northern Illinois. -
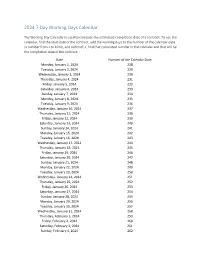
2024 7 Day Working Days Calendar
2024 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Monday, January 1, 2024 228 Tuesday, January 2, 2024 229 Wednesday, January 3, 2024 230 Thursday, January 4, 2024 231 Friday, January 5, 2024 232 Saturday, January 6, 2024 233 Sunday, January 7, 2024 234 Monday, January 8, 2024 235 Tuesday, January 9, 2024 236 Wednesday, January 10, 2024 237 Thursday, January 11, 2024 238 Friday, January 12, 2024 239 Saturday, January 13, 2024 240 Sunday, January 14, 2024 241 Monday, January 15, 2024 242 Tuesday, January 16, 2024 243 Wednesday, January 17, 2024 244 Thursday, January 18, 2024 245 Friday, January 19, 2024 246 Saturday, January 20, 2024 247 Sunday, January 21, 2024 248 Monday, January 22, 2024 249 Tuesday, January 23, 2024 250 Wednesday, January 24, 2024 251 Thursday, January 25, 2024 252 Friday, January 26, 2024 253 Saturday, January 27, 2024 254 Sunday, January 28, 2024 255 Monday, January 29, 2024 256 Tuesday, January 30, 2024 257 Wednesday, January 31, 2024 258 Thursday, February 1, 2024 259 Friday, February 2, 2024 260 Saturday, February 3, 2024 261 Sunday, February 4, 2024 262 Date Number of the Calendar Date Monday, February 5, 2024 263 Tuesday, February 6, 2024 264 Wednesday, February -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -
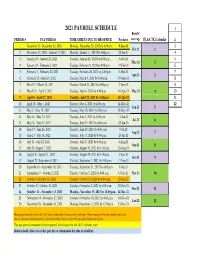
Payroll Calendar 2021
2021 PAYROLL SCHEDULE 1 Benefit PERIOD # PAY PERIOD TIME SHEETS DUE TO HR OFFICE Paydates coverage FLSA 7K Calendar 2 1 December 13- December 26, 2020 Monday, December 28, 2020 by 4:00 p.m. 8-Jan-21 3 Feb-21 1 2 December 27, 2020 - Janurary 9, 2021 Monday, January 11, 2021 by 4:00 p.m. 22-Jan-21 4 3 January 10 - January 23, 2021 Tuesday, January 26, 2021 by 4:00 p.m. 5-Feb-21 5 Mar-21 2 4 January 24 - February 6, 2021 Tuesday, February 9, 2021 by 4:00 p.m. 19-Feb-21 6 5 February 7 - February 20, 2021 Tuesday, February 26, 2021 by 4:00 p.m. 5-Mar-21 7 Apr-21 3 6 February 21 - March 6, 2021 Tuesday, March 9, 2021 by 4:00 p.m. 19-Mar-21 8 7 March 7 - March 20, 2021 Tuesday, March 23, 2021 by 4:00 p.m. 2-Apr-21 9 8 March 21 - April 3, 2021 Tuesday, April 6, 2021 by 4:00 p.m. 16-Apr-21 May-21 4 10 9 April 4 - April 17, 2021 Tuesday, April 20, 2021 by 4:00 p.m. 30-Apr-21 11 10 April 18 - May 1, 2021 Tuesday, May 4, 2021 by 4:00 p.m. 14-May-21 12 Jun-21 5 11 May 2 - May 15, 2021 Tuesday, May 18, 2021 by 4:00 p.m. 28-May-21 12 May 16 - May 29, 2021 Tuesday, June 1, 2021 by 4:00 p.m. 11-Jun-21 Jul-21 6 13 May 30 - June 12, 2021 Tuesday, June 15, 2021 by 4:00 p.m. -
Week of October 25, 2020
Police Department Patrick Nikolai, Chief of Police POLICE BLOTTER Week of October 25, 2020 The Police Blotter highlights a partial list of incidents in the city and is distributed on a weekly basis. The Blotter provides the date, time, approximate location, a narrative summary of the incident, case number and the most serious arrest charge. Meanwhile, the Arrest Log provides a timely, chronological summary of all the arrests made by the Santa Clara Police Department. It includes the name of the suspect(s), date of birth, city in which they reside, arrest date, time, location, case number as well as all the charge(s) associated with the arrest. This information, located on the Santa Clara Police Department’s home page (www.scpd.org), is updated daily and serves as the most comprehensive list of arrests made. Based on the mandatory orders from Santa Clara County Public Health, the City of Santa Clara has implemented many service level changes, limited to essential services. Since the preparation and distribution of a Police Blotter is not an essential service, it will be produced as resources are available. Sunday, October 25, 2020 Drug Sales Location: Warburton Avenue and Sanchez Place An officer on routine patrol observed an occupied vehicle parked near the dead end of a street. As the officer approached the vehicle, there was a strong odor of burnt marijuana. The officer contacted the three male subjects in the vehicle. The front passenger could be seen with a beer in his hands and a fixed blade knife was visible on the floorboard. As a precautionary measure, the subject’s were placed in handcuffs until additional assistance arrived. -
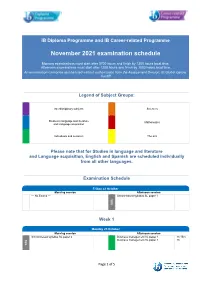
November 2021 Examination Schedule
IB Diploma Programme and IB Career-related Programme November 2021 examination schedule Morning examinations must start after 0700 hours and finish by 1300 hours local time. Afternoon examinations must start after 1200 hours and finish by 1800 hours local time. An examination cannot be rescheduled without authorization from the Assessment Division, IB Global Centre, Cardiff Legend of Subject Groups: Interdisciplinary subjects Sciences Studies in language and literature Mathematics and Language acquisition Individuals and societies The arts Please note that for Studies in language and literature and Language acquisition, English and Spanish are scheduled individually from all other languages. Examination Schedule Friday 22 October Morning session Afternoon session --- No Exams --- School-based syllabus SL paper 1 SBS Week 1 Monday 25 October Morning session Afternoon session School-based syllabus SL paper 2 Business management HL paper 1 1h 15m Business management SL paper 1 1h SBS Page 1 of 5 Tuesday 26 October Morning session Afternoon session Business management HL paper 2 1h 45m Language B HL paper 1 1h 30m Business management SL paper 2 1h 15m Language B HL paper 2 - Reading comprehension 1h Global politics HL paper 2 1h 45m Language B SL paper 1 1h 15m Global politics SL paper 2 1h 45m Language B SL paper 2 - Reading comprehension 1h Language ab initio SL paper 1 45m Language ab initio SL paper 2 - Reading comprehension 1h * Except: English & Spanish Latin HL paper 2 2h Latin SL paper 2 1h 30m Wednesday 27 October Morning session -

2020-21 Key Sports Dates
2020-2021 Sports Starting Dates Cross Country Class 4A Class 3A Class 2A Class 1A Class A Eight Player 1st Practice August 10, 2020 August 10, 2020 August 10, 2020 August 10, 2020 1st Competition August 24, 2020 August 24, 2020 August 24, 2020 August 24, 2020 Playing Dates 10 10 10 10 Scrimmages None None None None Post Season Tournament October 22, 2020 October 22, 2020 October 22, 2020 October 22, 2020 State Tournament October 31, 2020 October 31, 2020 October 31, 2020 October 31, 2020 Fall Golf 1st Practice August 10, 2020 1st Competition August 13, 2020 Playing Dates 12 Scrimmages None Post Season Tournament October 6, 2020 State Tournament October 9-10, 2020 Football 1st Practice August 10, 2020 August 10, 2020 August 10, 2020 August 10, 2020 August 10, 2020 August 10, 2020 1st Competition August 27, 2020 August 27, 2020 August 27, 2020 August 27, 2020 August 27, 2020 August 27, 2020 Playing Dates 9 9 9 9 9 9 Scrimmages 1 after 10 days of practice 1 after 10 days of practice 1 after 10 days of practice 1 after 10 days of practice 1 after 10 days of practice 1 after 10 days of practice Post Season Tournament Oct. 30, Nov. 6, 13 Oct. 30, Nov. 6, 12 Oct. 30, Nov. 6, 14 Oct. 30, Nov, 6, 14 Oct. 30, Nov. 6, 13 Oct. 30, Nov. 6, 12 State Tournament November 20, 2020 November 19, 2020 November 20, 2020 November 20, 2020 November 19, 2020 November 19, 2020 2020-2021 Sports Starting Dates Class 4A Class 3A Class 2A Class 1A Class A Eight Player Basketball 1st Practice November 16, 2020 November 16, 2020 November 16, 2020 November 16, 2020 1st Competition November 30, 2020 November 30, 2020 November 30, 2020 November 30, 2020 Playing Dates 21 21 21 21 Scrimmages 3--Anytime During Season 3--Anytime During Season 3--Anytime During Season 3--Anytime During Season Post Season Tournament Feb. -

The Johnsonian October 31, 1925
Winthrop University Digital Commons @ Winthrop University Browse all issues of the Johnsonian The oJ hnsonian 10-31-1925 The ohnsoniJ an October 31, 1925 Winthrop University Follow this and additional works at: https://digitalcommons.winthrop.edu/thejohnsonian Recommended Citation Winthrop University, "The oJ hnsonian October 31, 1925" (1925). Browse all issues of the Johnsonian. 72. https://digitalcommons.winthrop.edu/thejohnsonian/72 This Newspaper is brought to you for free and open access by the The oJ hnsonian at Digital Commons @ Winthrop University. It has been accepted for inclusion in Browse all issues of the Johnsonian by an authorized administrator of Digital Commons @ Winthrop University. For more information, please contact [email protected]. The Johnsonian THE OFFICIAL PUBLICATION OF THE STUDENT BODY OF WINTHROP COLLEGE VOLUME III, NUMBER 8 ROCK HILL, SOUTH CAROLINA. SATURDAY, OCTOBER 31, SUBSCRIPTION, 11.50 A YEA* JOHN DRINKWATER GHOSTS WILL WALK HAPPY BAL MASQUE IS EXAMINERS' TEST LITERARY SOCIETIES FINANCE COMMITTEE PLEASING SPEAKER IN GHOULISH ARRAY STAGED BY MASQUERS Mr. Sain Myerson, proprietor GIVENLIFE SAVERS ADMIT NEW MEMBERSSUBMIT S NEW BUDGET of the Ladies Shop, who is of- Celebrated British Poet Shows Psy- Weird Apparitions May Appear "Rudolph Valentino" Wins Prize fering $17.50 in cash prizes for Mrs. Cecelia Deublg, of National Red Varied Elements in Programs of !lic Puts Bon on Rallies and Other Sen- chological Basis ot Arts and Tonight—Halloween, the Night for Rest Costume—Much the best advertisements writ- Cross, Administers Rigid Tests; Th ree Societies — Prizes satic.ial Means—Canvas Was Reads His Own Poems of Witches, Is Here Cayety In Evidence ten by Winlhrop students fea- Fourteen Qualify Arc Offered Made This Week John Drinkwater, prominent Eng- Halloween, the very word sounds Last Saturday night Johnson Hall turing Mrs. -

2018 - 2019 Days of Rotation Calendar
2018 - 2019 DAYS OF ROTATION CALENDAR Day # Date Rotation Day Type Notes Day # Date Rotation Day Type Notes Saturday, October 13, 2018 Sunday, October 14, 2018 Monday, September 3, 2018 Holiday/Vaca Labor Day 27 Monday, October 15, 2018 Day 3 In Session 1 Tuesday, September 4, 2018 Day 1 In Session 28 Tuesday, October 16, 2018 Day 4 In Session 2 Wednesday, September 5, 2018 Day 2 In Session 29 Wednesday, October 17, 2018 Day 5 In Session 3 Thursday, September 6, 2018 Day 3 In Session 30 Thursday, October 18, 2018 Day 6 In Session 4 Friday, September 7, 2018 Day 4 In Session 31 Friday, October 19, 2018 Day 1 In Session Saturday, September 8, 2018 Saturday, October 20, 2018 Sunday, September 9, 2018 Sunday, October 21, 2018 Monday, September 10, 2018 Day Holiday/Vaca Rosh Hashanah 32 Monday, October 22, 2018 Day 2 In Session 5 Tuesday, September 11, 2018 Day 5 In Session 33 Tuesday, October 23, 2018 Day 3 In Session 6 Wednesday, September 12, 2018 Day 6 In Session 34 Wednesday, October 24, 2018 Day 4 In Session 7 Thursday, September 13, 2018 Day 1 In Session 35 Thursday, October 25, 2018 Day 5 In Session 8 Friday, September 14, 2018 Day 2 In Session 36 Friday, October 26, 2018 Day 6 In Session Saturday, September 15, 2018 Saturday, October 27, 2018 Sunday, September 16, 2018 Sunday, October 28, 2018 9 Monday, September 17, 2018 Day 3 In Session 37 Monday, October 29, 2018 Day 1 In Session 10 Tuesday, September 18, 2018 Day 4 In Session 38 Tuesday, October 30, 2018 Day 2 In Session Wednesday, September 19, 2018 Day Holiday/Vaca Yom Kippur 39 Wednesday, October 31, 2018 Day 3 In Session 11 Thursday, September 20, 2018 Day 5 In Session 40 Thursday, November 1, 2018 Day 4 In Session 12 Friday, September 21, 2018 Day 6 In Session 41 Friday, November 2, 2018 Day 5 In Session Saturday, September 22, 2018 Saturday, November 3, 2018 Sunday, September 23, 2018 Sunday, November 4, 2018 13 Monday, September 24, 2018 Day 1 In Session 42 Monday, November 5, 2018 Day 6 In Session 14 Tuesday, September 25, 2018 Day 2 In Session Tuesday, November 6, 2018 Prof Dev. -

Julian Date Cheat Sheet for Regular Years
Date Code Cheat Sheet For Regular Years Day of Year Calendar Date 1 January 1 2 January 2 3 January 3 4 January 4 5 January 5 6 January 6 7 January 7 8 January 8 9 January 9 10 January 10 11 January 11 12 January 12 13 January 13 14 January 14 15 January 15 16 January 16 17 January 17 18 January 18 19 January 19 20 January 20 21 January 21 22 January 22 23 January 23 24 January 24 25 January 25 26 January 26 27 January 27 28 January 28 29 January 29 30 January 30 31 January 31 32 February 1 33 February 2 34 February 3 35 February 4 36 February 5 37 February 6 38 February 7 39 February 8 40 February 9 41 February 10 42 February 11 43 February 12 44 February 13 45 February 14 46 February 15 47 February 16 48 February 17 49 February 18 50 February 19 51 February 20 52 February 21 53 February 22 54 February 23 55 February 24 56 February 25 57 February 26 58 February 27 59 February 28 60 March 1 61 March 2 62 March 3 63 March 4 64 March 5 65 March 6 66 March 7 67 March 8 68 March 9 69 March 10 70 March 11 71 March 12 72 March 13 73 March 14 74 March 15 75 March 16 76 March 17 77 March 18 78 March 19 79 March 20 80 March 21 81 March 22 82 March 23 83 March 24 84 March 25 85 March 26 86 March 27 87 March 28 88 March 29 89 March 30 90 March 31 91 April 1 92 April 2 93 April 3 94 April 4 95 April 5 96 April 6 97 April 7 98 April 8 99 April 9 100 April 10 101 April 11 102 April 12 103 April 13 104 April 14 105 April 15 106 April 16 107 April 17 108 April 18 109 April 19 110 April 20 111 April 21 112 April 22 113 April 23 114 April 24 115 April -

Ril May June July August September October
NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY NOVEMBER DECEMBER JANUARY