Madhya Pradesh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Madhya Pradesh Guna Kumar Shashwat 9826900549 Pass Raod,Guna (MP)-473001
State District Coordinator Mobile No. Dispatch Address C/o Ajay vajpayee,vajpayee house,sai township,BG by Madhya pradesh Guna Kumar Shashwat 9826900549 pass raod,Guna (MP)-473001 HDFC ERGO General Insurance Co Ltd. Sanmati palace, Madhya pradesh Damoh Rajesh Gupta/Awanindra Singh 8533067990/7990994472 beside SBI ATM,Station Road Damoh, M.P. 470675 Jawahar Road Circut House chok In Front of ICICI Bank Madhya pradesh Chhatarpur Dileep Kumar Sen 8828002460 Hdfc Ergo Gic Ltd Chhatarpur HDFC ERGO General Insurance Co Ltd.House no 1779 Opp NCC Group head Qtr near cine city talkies, Madhya pradesh Sagar Rajesh jaiswal/Pandav kumar 7722996662/8819089222 Rajakhedi , Makornia Sagar 470003 , MP, 3rd floor Guptaji building in front of MP electricity board rest house,old RTO office,Satna road,Panna- Madhya pradesh Panna Vikash Kushwaha 7355598324 488001 C/o santosh kumar raghuwanshi guna road ward no 1 Madhya pradesh Ashoknagar Dharmendra Shrivastava/Sachin Kushwah 9713856610/758180023 ramraja agro ke samne,Ashoknagar, M.P. 473331 Madhya Pradesh Katni Ward No. 28, Housing Board Colony, Bajrang Nagar, Narayan Patel 8964070516 Madhya Pradesh Umariya Nepali Mohalla, Katni Madhya Pradesh Shahdol Village Paraswada, Post Rakhi, Tehsil Gotegaon, Arvind Kumar Vishwakarma 9977747496 Madhya Pradesh Jabalpur Narsinghpur, 487118 At Ambedkar Colony, Loniya Karbal, Near Cold Storage, Madhya Pradesh Narsinghpur Nitesh Giri 9165365343 Parasiya Road, Chhindwara, 480001 H. No. 70, Ward No. 16, Kushmeli, Near Krishi Upaj Madhya Pradesh Chhindwara Rakesh Singh Raghuwanshi 9424456722 Mandi, Chhindwara M.P. 480001 Madhya Pradesh Dindori S/O Nemilal Singour, Hanumanji Ward No. 22, H. No. Jageshwar Singour 9165775243 Madhya Pradesh Mandla 156, Basori Mohalla, Mahrajpur, Mandla, 481665 Madhya Pradesh Sheopur HDFC ERGO GIC LTD. -

CIN/BCIN Company/Bank Name Investor First Name Investor Middle
Note: This sheet is applicable for uploading the particulars related to the amount credited to Investor Education and Protection Fund. Make sure that the details are in accordance with the information already provided in e-form IEPF-1 CIN/BCIN L99999MH1962GOI012398 Prefill Company/Bank Name MOIL LIMITED Sum of unpaid and unclaimed dividend 0.00 Sum of interest on matured debentures 0.00 Sum of matured deposit 0.00 Sum of interest on matured deposit 0.00 Sum of matured debentures 0.00 Sum of interest on application money due for refund 0.00 Sum of application money due for refund 6759361.25 Redemption amount of preference shares 0.00 Sales proceed for fractional shares 0.00 Validate Clear Date of event (date of declaration of dividend/redemption date of preference shares/date of Investor First Investor Middle Investor Last Father/Husband Father/Husband Father/Husband Last DP Id-Client Id- Amount Address Country State District Pin Code Folio Number Investment Type maturity of Name Name Name First Name Middle Name Name Account Number transferred bonds/debentures/application money refundable/interest thereon (DD-MON-YYYY) SHIVKUMAR KAWALE NA VINOBA BHAVE NAGAR,PLOT NO 650INDIA MAHARASHTRA NAGPUR 440002 DPID-CLID-IN301330209Amount for application mone 2231.25 11-DEC-2010 CHANDRAPALSINGGAYAPRASAD SINGH NA MOIL DONGRI BUZRUK MINE,TAH TUINDIA MAHARASHTRA BHANDARA 441902 DPID-CLID-IN301330209Amount for application mone 5100.00 11-DEC-2010 SINHA NANDKISHOR BIRJU NA 692 A,BAZARTOLA,TA TUMSAR,DIST INDIA MAHARASHTRA BHANDARA 441907 DPID-CLID-IN301330209Amount -

District Population Statistics, 22 Allahabad, Uttar Pradesh
.------·1 Census of India, 1951 I DISTRICT POPULATION STATISTICS UTTAR PRADESH 22-ALLAHABAD DISTRICT t I 315.42 ALLAHABAD: PluNnNG AND STATIONERY, UTTAR PRADESH, INDIA 1951 1953 ALL CPS Price, Re.1-S. FOREWORD THE Uttar Pradesh Government asked me in March, 1952, to supply them for the purposes of elections to local bodies population statistics with separation for scheduled castes (i) mohalla/ward -wise for urban areas, and (ii) village-wise for rural areas. The Census Tabulation Plan did not provide for sorting of scheduled castes population for areas smaller than a tehsil or urban tract and the request from the Uttar Pradesh Government came when the slip sorting had been finished and the Tabulation Offices closed. As the census slips are mixed up for the purposes of sorting in one lot for a tehsil or urban tract, collection of data regarding scheduled castes population by mohallas/wards and villages would have involved enormous labour and expense if sorting of the slips had been taken up afresh. Fortunately, however, a secondary census record, viz. the National Citizens' Register, in which each slip has been copied, was available. By singular foresight it had been pre pared mohalla/ward-wise for urban areas and village-wise for rural areas. The required information has, therefore, been extracted from this record. 2. In the above circumstances there is a slight difference in the figures of population as arrived at by an earlier sorting of the slips and as now determined by counting from the National Citizens' Register. This difference has been accen tuated by an order passed by me during the later count. -

Jiwaji University, Gwalior Centre List for B.A
JIWAJI UNIVERSITY, GWALIOR CENTRE LIST FOR B.A. I, II & III YEAR ------------------------------------------------------------------------------------------------------------------------------ ** CENTRE : 501 : GOVT. NEHRU DEGREE COLLEGE, ASHOKNAGAR 501 GOVT. NEHRU DEGREE COLLEGE, ASHOKNAGAR 502 GOVT. COLLEGE, MUNGAWALI (ASHOKNAGAR) 503 GOVT. MADHAV COLLEGE, CHANDERI (ASHOKNAGAR) 504 I.C.S.M.COLLEGE, ASHOKNAGAR 505 SHRI VARDHMAN GIRLS COLLEGE, ASHOKNAGAR 506 SHRI LAL SHUKLA COLLEGE, ASHOKNAGAR 507 EXCELLENCE COLLEGE OF SCIENCE & MGMT.,ASHOKNAGAR 508 INDIRA GANDHI PROFESSIONAL COLLEGE, CHANDERI 509 SHRI DWARIKA PRASAD YADAV MAHAVIDHLAYA,ASHOK NAGAR 510 YUVA MAHAVIDHLAYA,ASHOK NAGAR 511 INDIAN COLLEGE, ASHOK NAGAR 904 VEDANTA MAHAVIDHLAYA,ISHAGARH, ASHOK NAGAR ---------------------------------------------------------------------------------------------------------------------------- ** CENTRE : 521 : GOVT. M.J.S. COLLEGE, BHIND 521 GOVT. M.J.S. COLLEGE, BHIND 522 GOVT. GIRLS COLLEGE, BHIND 523 JAIN DEGREE COLLEGE, BHIND 524 KUSUMBAI JAIN GIRLS COLLEGE, BHIND 525 MAHARSHI ARVIND GOVT. COLLEGE, GOHAD (BHIND) 526 GOVT. SHRI GANDHI COLLEGE,BALAJI-MIHONA(BHIND) 527 GOVT. COLLEGE, AALAMPUR 528 GOVT. COLLEGE, MEHGAON (BHIND) 529 DURGAPRASAD SARRAF COLLEGE, DABOH, BHIND 530 RISHISHWAR COLLEGE, PHOOF (BHIND) 531 GOVT. COLLEGE, ATER 532 CHOUDHARY DILIP SINGH GIRLS COLLEGE, BHIND 533 CHOUDHARY YADUNATH SINGH COLLEGE, BHIND 534 CH.KAMAL SINGH COLLEGE, MOU, BHIND 535 SMT. VIJYARAJE SYNDIA COLLEGE, ADOKHAR 536 BIHARI COLLEGE, BHIND 537 VIDYAWATI COLLEGE, -

Current Affairs - One Liner 6-9 Advertisement, Contact:- Spotlight 10 [email protected] the People 11-18 Ph.: 09208037962 News Bites 19-49
CONTENTS VOL-17 ISSUE -02 Editor Key Highlights of Padma Awards 2021 N.K. Jain Economic Survey 2020-21 Advisors Neeraj Chabra K.C.Gupta Registered Office Mahendra Publication Pvt. Ltd. 103, Pragatideep Building, Union Budget 2021 Plot No. 08, Laxminagar, District Centre, New Delhi - 110092 TIN-09350038898 w.e.f. 12-06-2014 Branch Office Mahendra Publication Pvt. Ltd. E-42,43,44, Sector-7, Noida (U.P.) Interview 5 For queries regarding promotion, distribution & Current Affairs - One Liner 6-9 advertisement, contact:- Spotlight 10 [email protected] The People 11-18 Ph.: 09208037962 News Bites 19-49 Owned, printed & published by Designation : Who's Who 50 N.K. Jain Word of English - Etymology 51 103, Pragatideep Building, Plot No. 08, Laxminagar, Padma Awards 2021 52-54 District Centre, New Delhi - 110092 Key Highlights of Economic Survey 2020-21 55-63 Please send your suggestions and grievances to:- Union Budget 202154-56 64-74 Mahendra Publication Pvt. Ltd. Quiz Time - General Awareness 75-86 CP-9, Vijayant Khand, RRB Clerk Mains - Model Paper 2020 87-120 Gomti Nagar Lucknow - 226010 E-mail:[email protected] SSC CGL Pre - Model Paper 2020 121-132 © Copyright Reserved # No part of this issue can be printed in whole or in part without the written permission of the publishers. # All the disputes are subject to Delhi jurisdiction only. Mahendra Publication Pvt. Ltd. Editorial “One should constantly strive to acquire knowledge and by doing so one shall be praised and respected amongst by scholars.” - Rig Veda Dear Aspirants, We feel delighted to present to you the "February 2020" edition of "Master in Current Affairs". -
Change Story Name.Xlsx
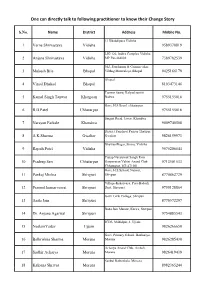
One can directly talk to following practitioner to know their Change Story S.No. Name District Address Mobile No. 13 Khakdipura Vidisha 1 Varna Shrivastava Vidisha 9589370819 LIG 126, Indira Complex Vidisha 2 Anjana Shrivastava Vidisha MP Pin-464001 7389782539 302, Panchanan & Gramin vikas 3 Mukesh Bile Bhopal Vibhag Mantralaya, Bhopal 9425166179 Bhopal 4 Vinod Dhakad Bhopal 8103473146 Tanwar Samaj Kalyad samiti 5 Kamal Singh Tanwar Khargoan Badwa 9755155016 Govt. H.S.Scool chhatarpur 6 R.B.Patel Chhatarpur 9755155016 Singaji Road, Jawar, Khandwa 7 Narayan Farkale Khandwa 9009740508 District Panchyat Parisar Thatipur 8 A.K.Sharma Gwalior Gwalior 9826159973 BhawaniNagar, Sironj, Vidisha 9 Rajesh Patel Vidisha 9575206544 Pratap Navyuwak Sangh Evm 10 Pradeep Sen Chhatarpur Oaryavaran Vahini Anand Club 9713501533 Chhatarpur, MP-471001 Govt. H.S.School, Natwar, 11 Pankaj Mishra Shivpuri Shivpuri 8770862729 Village-Kakarvaya, Post-Badodi, 12 Pramod kumar rawat Shivpuri Distt. Shivpuri 9755128804 Govt. Girls College, Shivpuri 13 Anita Jain Shivpuri 8770572297 Bada Jain Mandir, Karira, Shivpuri 14 Dr. Anjana Agarwal Shivpuri 9754885543 ICDS, Mahidpur-1, Ujjain 15 NeelamYadav Ujjain 9826266650 Govt. Primary School, Banbariya, 16 Balkrishna Sharma Morena Morena 9826285430 Acharya Anand Club, Ambah, 17 Sudhir Acharya Morena Morena 9826419439 Sankul Rathorkala, Morena 18 Kalpana Shrivas Morena 8982365244 One can directly talk to following practitioner to know their Change Story S.No. Name District Address Mobile No. Govt. Primary School Kakarwara , 19 Vijit Jain Shivpuri Shivpuri 9406965576 LIG-126, Indira Complex, Vidisha 20 Sadhna Shrivastava Vidisha 9868751037 Behind Satyam Road, Ashok 21 Rahul Sharma Ashoknagar Nagar 9685021646 70-Suraj Market, Barwaha, 22 Parvati Khetwas Khargoan Khargone 9111277718 Main Road Aamkheda, Post- 23 Rambabu Kushwah Vidisha banskhedi, Aspal Sironj, Vidisha 9009510425 Lav-Kush Chok, Custom Path, 24 Abhishek Kushwah Vidisha Sironj, Vidisha 7354526108 Govt. -

Final Electoral Roll
FINAL ELECTORAL ROLL - 2021 STATE - (S12) MADHYA PRADESH No., Name and Reservation Status of Assembly Constituency: 16-GWALIOR Last Part EAST(GEN) No., Name and Reservation Status of Parliamentary Service Constituency in which the Assembly Constituency is located: 3-GWALIOR(GEN) Electors 1. DETAILS OF REVISION Year of Revision : 2021 Type of Revision : Special Summary Revision Qualifying Date :01/01/2021 Date of Final Publication: 15/01/2021 2. SUMMARY OF SERVICE ELECTORS A) NUMBER OF ELECTORS 1. Classified by Type of Service Name of Service No. of Electors Members Wives Total A) Defence Services 1202 74 1276 B) Armed Police Force 0 0 0 C) Foreign Service 2 1 3 Total in Part (A+B+C) 1204 75 1279 2. Classified by Type of Roll Roll Type Roll Identification No. of Electors Members Wives Total I Original Mother roll Integrated Basic roll of revision 1200 75 1275 2021 II Additions Supplement 1 After Draft publication, 2021 11 0 11 List Sub Total: 11 0 11 III Deletions Supplement 1 After Draft publication, 2021 7 0 7 List Sub Total: 7 0 7 Net Electors in the Roll after (I + II - III) 1204 75 1279 B) NUMBER OF CORRECTIONS/MODIFICATION Roll Type Roll Identification No. of Electors Supplement 1 After Draft publication, 2021 0 Total: 0 Elector Type: M = Member, W = Wife Page 1 Final Electoral Roll, 2021 of Assembly Constituency 16-GWALIOR EAST (GEN), (S12) MADHYA PRADESH A . Defence Services Sl.No Name of Elector Elector Rank Husband's Address of Record House Address Type Sl.No. Officer/Commanding Officer for despatch of Ballot Paper (1) (2) (3) -

Agenda for 671 SEIAA Meeting Dated
Agenda for 671 st SEIAA Meeting dated 01.04.2021 1. Case No 7864/2020 M/s K.P.Singh Bhadoria Contractor, E-46 A, Balvant Nagar, Thatipur, Dist. Gwalior, MP - 474002 Prior Environment Clearance for Sand Quarry in an area of 6.0 ha. (1,20,000 cum per annum) (Khasra No. 546), Village - Kamkomohniya, Tehsil - Dindori, Dist. Dindori (MP) 2. Case No 8216/2021 Shri Samir Giri S/o Shri Ramesh Giri, B-2/1102, Maple Woods, Nipaniya, Dewas Naka, Dist. Indore, MP - 452016 Prior Environment Clearance for Stone Quarry in an area of 2.0 ha. (20000 cum per annum) (Khasra No. 314), Village - Murmari, Tehsil - Mohkhed, Dist. Chhindwara (MP) 3. Case No 8360/2021 M/s Parmar Construction, Prop., Shri Krishna Kumar Parmar, Madiyasaar, Tehsil & Dist. Dindori, MP - 480880 Prior Environment Clearance for Stone Quarry in an area of 1.720 ha. (5004 cum per annum) (Khasra No. 22), Village - Khirsari Mal, Tehsil - Dindori, Dist. Dindori (MP) 4. Case No 8372/2021 M/s Madhav Infra Project Ltd, Madhav House, Plot No. 04, Near Panchratna Building, Shubhanpur, Dist. Badauda - 390023 Prior Environment Clearance for Soil/Murrum Quarry in an area of 4.609 ha. (130000 cum per annum) (Khasra No. 119), Village - Bansara, Tehsil - Shadhaura, Dist. Ashoknagar (MP) 5. Case No 8361/2021 Shri Nandkishore Chandel S/o Shri Rammilan Chandel, Sarhari, Tehsil & Dist. Dindori, MP - 481880 Prior Environment Clearance for Stone Quarry in an area of 1.480 ha. (5000 cum per annum) (Khasra No. 1560), Village - Bahera Mal, Tehsil - Dindori, Dist. Dindori (MP). 6. -

LIST of MINING PROJECTS - MPSEAC PENDING S.No
LIST OF MINING PROJECTS - MPSEAC PENDING S.No. Case No Category Name of Project Proponent Activity 1 59/2008 1(a) Agrawal Mineral process, Manganese ore mine 5.00 ha. Gwari-wadhana, 1(a) NagpurRoad , Chhindwara M.P. Teh-Sausar, Distt-Chhindwara M.P. 2 70/20081 1(a) M/s Ismail & Sons MissionChowk, Lime stone mine 10-748 ha. Village Bhatgaon (a) Katni M.P. Sunehra Teh-Murwada Katni M.P. 3 99/2008 1(a) M/s Nirmala Minerals Dubiyara Iron Ore Mine 32.375 ha. at 1(a) PathalewardKatni M.P. DubiyaraTalluka-Sihora Jabalpur M.P. 4 104/2008 1(a) Anand mining corporation Dubiyara-Tikaria Iron ore mine 26.00 ha at Village 1(a) Pathakward, Katni- M.P. Dubiyara Tikaria Jabalpur 5 411/2009 1(a) Shri Kishore Kumar Station Road , Limestone & Dolomite mine 5.605 ha. 6200 TPA 1(a) Katni-M.P. at Village- Chandan Teh- Murwara, Distt-Katni- M.P. 6 412/2009 1(a) M/s Kamal lime Industries Station Lime stone & Dolomite mine 7.205 11500 TPA at 1(a) Road Katni-M.P. Village ChandanTeh-Murwara Katni-M.P. 7 434/2009 1(a) Smt. Rekha Sharma 192, Second Laterite, clay and Red ochre deposit mine 6.83 ha. 1(a) Floor, Rachna Nagar Bhopal-M.P. at village Salebhar Teh- Bahoriband, Distt-Katni- M.P. 8 472/2009 1(a) N.M. Dubash Stone & Lime Co. Pvt Lime stone & Dolomite mine 7.42 ha. production 1(a) Ltd Station Raod, Maihar Satna capacity 1.6 lakhs TPA at village Kachhgawan, –M.P. -

Jaetal Vihar
https://www.propertywala.com/jaetal-vihar-gwalior Jaetal Vihar - Thatipur, Gwalior Safe haven Jaetal Vihar presented by Jaetal Group offer 1, 2 & 3 Bhk apartments available in Thatipur, Gwalior Project ID : J399841118 Builder: Jaetal Group Location: Jaetal Vihar, Thatipur, Gwalior - 474001 (Madhya Pradesh) Completion Date: Nov, 2016 Status: Started Description Jaetal Vihar is a popular residential project by Jaetal Group in Thatipur, Gwalior. This residential project offers spacious 1, 2 & 3 Bhk apartments ranging between 612-1260 sq.ft. equipped with basic amenities for the comfort of residents. The facilities within the project are well designed. RERA ID: P-GWL-19-2098 Amenities Children's Play Area 24*7 Security Power Backup Rain Water Harvesting Club House Swimming Pool Gymnasium Sewage Jaetal Group is a leading real estate developer with a significant presence in other segments, including services, consumer products and manufacturing. Jaetal Group is known for its flagship companies like Jaetal Construction Private Limited, Jaetal Holdings Limited and Jaetal Chemicals Private Limited among others. The Group focuses on quality across all its business endeavours. The Group has always emphasized on the qualitative aspect of real estate development Features Luxury Features Security Features Power Back-up Centrally Air Conditioned Lifts Security Guards Electronic Security RO System High Speed Internet Wi-Fi Intercom Facility Lot Features Interior Features Balcony Woodwork Modular Kitchen Feng Shui / Vaastu Compliant Recreation Maintenance -

271120191113351031248261119
Data under the Central Sector Scheme of Scholarship for College and University Students S.No.. Application ID Board Name Applicant Name Father's Name Categroy Gender Annual Applicant's Applicant's Applicant's Institute Name Institute Address Applicant's Applicant's Renewal Application Status Family Address District Domicile State Mobile Email Status Income 1 MP201819008150636 BOARD OF SECONDARY SAPNA PANCHAL MAHESH OBC F 35000 WARD NO 5 AGARMALWA MADHYA MATA JEEJA BAI moti tabela indore (m.p.) 9424074178 sapnapanchal62 Renewed Application Under EDUCATION , BHOPAL PANCHAL MACHALPURA PRADESH GOVT. P.G. GIRLS [email protected] Process for ROAD DIST COLLEGE MOTI Verification at AGARMALWA TABELA, INDORE Institute Level MP 2 MP201819000786710 BOARD OF SECONDARY RAJU PRAJAPATI BAISAKHU SC M 40000 JANUNA ANUPPUR MADHYA GOVT. Civil Lines - Pachpedi, 9179792038 praju6181@gm Renewed Application Under EDUCATION , BHOPAL PRAJAPATI COLLIERY WARD PRADESH AUTONMOUS Jabalpur ail.com Process for NO 05 ANUPPUR SCIENCE COLLEGE, Verification at CIVIL LINESR, Institute Level 3 MP201819008030317 BOARD OF SECONDARY SOURABH MAHESH SINGH GENERAL M 40000 GRAM DERKA ASHOKNAGAR MADHYA GOVT. NEHRU Govt. Nehru Degree 7828270629 SOURABHRAGH Renewed Application Under EDUCATION , BHOPAL RAGHUWANSHI ASHOKNAGAR PRADESH DEGREE COLLEGE College, Near Bypass, UWANSHI@GM Process for Eshagarh Road, AIL.COM Verification at Ashoknagar, Ashoknagar Institute Level 4 MP201819008715789 BOARD OF SECONDARY PRIYAM JAIN pawan jain GENERAL F 50000 ward no 4 jain ASHOKNAGAR MADHYA GOVT. NEHRU Govt. Nehru Degree 8827902908 Renewed Application Under EDUCATION , BHOPAL mandir ke pass PRADESH DEGREE COLLEGE College, Near Bypass, Process for piprai Eshagarh Road, Verification at Ashoknagar, Ashoknagar Institute Level 5 MP201819001892162 BOARD OF SECONDARY RISHI KUMAR SAHU shambhu dayal OBC M 40000 near jain ASHOKNAGAR MADHYA NATIONAL National Institute of 8878134349 iitianrishi50@g Renewed Application Under EDUCATION , BHOPAL sahu tempaln ,gram PRADESH INSTITUTE OF Technology Raipur G.E. -

Gram Panchayat Spatial Development Plan Dec 2020 for Ministry of Panchayati Raj Government of India
Gram Panchayat Spatial Development Plan Dec 2020 for Ministry of Panchayati Raj Government of India Shankarnarayana Gram Panchayat Spatial Development Plan-2020 Shankaranarayana ii PROJECT TEAM Manipal School of Architecture and Planning(MSAP), Udupi District, Karnataka Overall Co-ordination: Dr. Deepika Shetty, Director and Professor, MSAP, Manipal Project Team: Dr. Udaya Shankara HN, Professor, Department of Civil Engineering, MIT, Manipal Shri. Lino Yovan, Research Associate, MIT, Manipal Ms. Joicy KJ, Associate Professor, MSAP Shri. Shanta Pragyan Dash, Assistant Professor, MSAP Ms. Ipsitaa Priyadarsini Das, Assistant Professor, MSAP Shri. Amarnath Sharma, Assistant Professor, MSAP Ms. Rituka Kapur, Assistant Professor, MSAP Shri. Satyaprakash Das, Assistant Professor, MSAP Ms. Sanjana Shetty, Assistant Professor, MSAP Ms. Sasmita Chand, Assistant Professor, MSAP Ms. Krutika Madkaiker, Assistant Professor, MSAP Ms. Sharvani Bhat, Student Intern, MSAP Masters students from second year Masters in urban design and development. (M.Arch. MUDD), MSAP Aadityaraj Jain Kotian Gaurav Srinivasa Rahul Menon Sidhartha Sunil Dutt Praveen Kumar R Harnoor Dhillon Pooja Pankajbhai Mehta Kanchi Madhulika R Auna Sando Abhijna Tanya .M. Thimmaiah Aayushman Singh Bhati Gayathrie J R P Harini Sarvani Gundu Pinki Bose Akkamahadevi Aman Kashyap Debjani Das Regional Remote Sensing Centre - South / NRSC / ISRO, Bengaluru Overall Co-ordination: Dr. Sudha R., Scientist ‘SG’ Project Team: Dr. K.S. Ramesh Head, Applications Dr. Rama Subramoniam S. Scientist ‘SF’ Smt. Shivam Trivedi Scientist ‘SE’ Smt. Manjula V. Bhagwat Scientist ‘SD’ RC-North (New Delhi) Team and RC- Hyderabad Team: Provided inputs on satellite datasets and thematic layers (SIS-DP Phase-I), household survey data and results of run-off estimation. Overall Technical Guidance: Dr.