Assessment of Maximal Aerobic Capacity in Ski Mountaineering: a Laboratory-Based Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ski Mountaineering Camp Packet
Mount Hood Intro to Ski Mountaineering Camp Mount Hood, Oregon June 22-24, 2021 Level: 14 and Older A girls-only introduction to ski mountaineering camp on Mount Hood, Oregon. The camp will include an all-female professional guide team and education on ski mountaineering fundamentals. Itinerary: June 22nd 3-5pm: Orientation Guides will meet the girls participating in this camp at 3pm to go over the following: • Expectations/ goals for the camp • Safety briefing • Gear check • Tips on how to pack your pack June 23rd: Ski Mountaineering Day School Meet time: TBD Guides will meet the girls at the base of Timberline ski area. From the top of the lifts they will tour above the ski area and review skills for the summit attempt the following day. This will include ice axe self-arrest, how to use crampons, basic skinning techniques, rope travel and other skills that the guides think will be important to cover before the summit attempt. Following the field day guides will review the day with the girls and review the plan for the summit day! June 24th: Summit Attempt Guides and athletes will meet at the base of Timberline ski area and make an attempt to ski off the summit (weather and route conditions depending). If all goes according to plan, guides and athletes will ride the chairlift to the top of the ski area. They will make their summit attempt from there dependent on conditions and weather. If conditions do not allow us to ski off the summit, guides will make that decision and we have the option to leave our skis at various places on the route. -

Backcountry and Ski Mountaineering Gear List
Joe Stock ◊ IFMGA Mountain Guide +1-907-830-0125 ◊ [email protected] www.stockalpine.com ◊ www.alaskaguidecollective.com Backcountry and Ski Mountaineering Gear List Please print the relevant sections to use as a checklist. Inquire with Joe about any questions. Anchorage Rentals ● Outdoor Gear: a laskaoutdoorgearrental.com ● Ski Gear: alaskamountaineering.com/rentals/ ● Split Boards: b lueandgoldak.com Provided by Stock Alpine ● Emergency shelter and communication ● Navigation, first aid, and repair kits ● BCA Link radios ● Camping tents and cook gear ● Glacier ropes ● Some gear is available for loan Pack your day trip gear t he night before so you’re less likely to forget things. You only have to remember three things: 1) Pack 2) Boots 3) Skis with skins on, strapped together with your poles. 1) Ski Gear: for all trips ____ Skis. Opt for Lightweight alpine touring (AT) skis with 100-110mm underfoot for Nov-March tours, and 90-100mm underfoot for April-July tours. Joe’s choice: G3 Blizzard Zero G, Atomic Backland 107. ____ Bindings. AT tech-style bindings preferred. Heavy, sidecountry, frame bindings are not recommended as they will limit your runs no matter how strong you are. Joe’s choice: G3 Zed binding, Dynafit Rotation binding, ATK. or ____ Splitboard and Bindings. A GC choice: G3 Blacksheep Splitboard, Spark bindings for backcountry use or Phantom for splitboard mountaineering with hard boots. ____ Binding Repair Kit. Recommended. Repair parts are scarce away from Anchorage and Girdwood. Backcountry Ski Gear List - 1 - May 2021 Joe Stock ◊ IFMGA Mountain Guide +1-907-830-0125 ◊ [email protected] www.stockalpine.com ◊ www.alaskaguidecollective.com ____ Brakes or Leashes. -

Jacksonhole Skier 2009
JacksonHole skier 2009 WINTER VISITOR’S GUIDE FREE . Inviting you to our 35th Anniversary Shearling Sale 20 W. Broadway Downtown Jackson Across from the Wort Hotel Est. 1973 www.jollyjumbuckleathers.com 307.733.6562 Experience the Old West in a New Way. Mesquite grilled Steaks, Game, and other New West selections, all served in our authentic lodge. Enjoy our extensive collection of scotch, bourbon and draft beer & extensive wine selection. 862 W. BROADWAY • 733-3287 STEAK & GAME HOUSE 2 JACKSON HOLE SKIER 2009 CUSTOM JEWELRY BY JETER CASE In the log cabin next to Teton Theatre just off the town square 132 N. Cache Jackson Hole, Wyoming 307-733-5933 www.jcjewelers.com 800-358-5715 www. focusproductions. com 2009 JACKSON HOLE SKIER 3 H SKI • BIKE • BOARD • HIKE “The Locals’ Shop” SKIS, BOOTS, 520 W. BROADWAY & BINDINGS: OPEN DAILY Volkl • Rossignol 733-5335 r e • g Dalbello Tecnica e L On Broadway f f e J • • : Marker Salomon Full Tilt across from r e i k Bubba’s S s n o i SNOWBOARDS: t c u d o r Burton • Arbor • Prior P s u c o F Nitro • Salomon• Vans / y o K c M e CLOTHING: d a W : o • • t Obermeyer Orage Bonfire o h P Sherpa • Burton • Oakley www.hobacksports.com DEMOS A RENTALS RENTALSA REPAIR A SKIS A SNOWBOARDSA OUTWEAR 4 JACKSON HOLE SKIER 2009 32 years of inspiration at 6,000 feet Jewelry Originals Downtown Jackson 125 N.Cache, Gaslight Alley 307.733.2259 www.DanShelley.com [email protected] ALL DESIGNS COPYRIGHTED jackson hole skier 2008/2009 the resorts 24 Jackson Hole 34 The Tram Builders 38 Vertical-Foot Ski Records 40 Open-Boundary Protocol 41 Terrain Park & Superpipe 42 Snow King 46 Grand Targhee 52 White Pine the backcountry 12 Teton Skiing 54 Mountain Guides 64 Teton Pass Ambassador 66 Avalanche Education 68 Helicopter & Snowcat Skiing Skiers: Cover—Jason Tattersall Contents—Lynsey Dyer staff other stuff Publishers: Bob Woodall and Wade McKoy 8 Wildlife and National Parks d.b.a. -

International Ski Mountaineering Federation
Sporting Rules & Regulations – Approved by ISMF PA 16/06/2018 International Ski Mountaineering Federation Sporting Rules & Regulations Any change requested by the organiser regarding itineraries or schedule in the following regulation has to be presented to and approved by the ISMF technical team in advance. NB : All rules and regulations may be subject to modification of the language used, in so much as the context and the content of the rule/regulation will remain unaltered but the English language used within in said rules and regulations may be subject to improvement in terms of grammar and clarity. 1 Sporting Rules & Regulations – Approved by ISMF PA 16/06/2018 INDEX 1. INTRODUCTION ................................................................................................................................................. 3 1.1 DEFINITIONS ............................................................................................................................................................. 3 1.2 ABBREVIATIONS ........................................................................................................................................................ 3 1.3 REFERENCES ............................................................................................................................................................. 3 2. EVENTS AND COMPETITIONS ............................................................................................................................ 4 2.1 GENERAL FEATURES OF ISMF RACES .............................................................................................................................. -

From: Lee Greenwald To
From: Lee Greenwald To: FS-objections-pnw-mthood Subject: Twilight Parking lot Date: Monday, March 03, 2014 11:44:20 PM Attachments: 2013 International Report on Snow Mountain Tourism.pdf Cross-country skiing experiencing a Nordic renaissance Olympian.pdf Twilight Parking Lot OBJECTION 3-1-14 EAE v2.doc Dear objections official, I previously raised several objections concerning Mt Hood Meadows application to build the Twilight Parking lot. Though some, not all, of these objections were ostensibly addressed in their responses, they were not addressed fully nor adequately. I raised concerns regarding Meadows assumptions on growth in demand for Alpine skiing. The last ten years MHM stated continued growth trends, but actually the most recent previous two years that has not been the trend. The true growth is in Nordic skiing. The majority of the Nordic community is against the creation of the Twilight lot without a comprehensive analysis of potential future use of this terrain, and nearby Nordic trails and connecting trails. This type of analysis has not been done, and would be precluded by proceeding with the construction of the Twilight lot before all future use options have been considered. Second, I asked that MHM be required by the FS to place the funds, $500,000, for a Nordic center in a designated account for a future Nordic center building, and a restrictive timeline for construction. If the parking lot is to be built, the Nordic community should have some prior input on the Nordic facility to be built prior to the lots final approval. The response that was posted simply stated that "a" facility would be built within three years. -

CRANS-MONTANA Altus Publi-Reportage
2019 Français / English CRANS-MONTANA ALTUS Publi-reportage ALTUS Édito Chaque année, nous pensons à vous ! CRANS-MONTANA HIVER 2019 - N° 6 Concevoir un magazine comme Altus, nécessite une bonne dose de passion ! Passionnés de montagne nous le sommes jusque dans le désir de partage, de vous ouvrir les portes de notre territoire et de Retrouvez ALTUS vous connaître. Chaque année, nous pensons à vous lorsque nous décidons des sujets des éditions sur votre mobile. de l’hiver suivant. Qu’est-ce qui motive votre venue dans cette station en particulier ? Quels sont les www.altus-magazines.com reportages qui allient découverte et plaisir ? Comment vous proposer une lecture à la fois intelligente et distrayante ? Fabriquer Altus constitue un travail de longue haleine qui nous mobilise tout au DIRECTION long de l’année. Dès le mois de janvier, nous concevons le sommaire des magazines de décembre, Directeur de la publication : Alain Poncet afin de produire des articles dont les textes comme les photos collent à la saison. Une anticipation [email protected] nécessaire pour vous livrer des magazines au plus près de leur territoire, de leur actualité, de leur Directeur d’édition vivacité, de leurs lumières au pluriel. Roland Claude Durand-Terrasson [email protected] Nous aimons aussi notre métier, car il est un lien entre vous et ce que nous chérissons : la montagne. RÉDACTION Vous découvrez notre vallée à travers nos pages, vous aimez cet endroit parce qu’il est devenu un peu Rédactrice en chef : Sylvie Piaget le vôtre, peut-être en partie grâce à nous, voilà ce qui motive notre volonté de poursuivre l’aventure. -
Calendar of Events
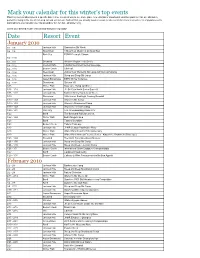
Mark your calendar for this winter's top events Planning your vacation around a specific date in time is a great way to see some place new. And ski or snowboard vacation spots like Vail are absolutely perfect for being in the mix of non-stop fun and excitement. And not that you actually need a reason to take a vacation, here is an entire list of popular events and traditions you can plan your trip around for fun, fun fun - all winter long. Select your desired month of travel and start planning today! Date Resort Event January 2010 1/2 - 1/9 Jackson Hole Snowriders Ski Week 1/4 - 1/9 Steamboat 11th Annual Musicfest at Steamboat Park City PCMR Freestyle Classic 1/4 - 1/10 1/4 - 1/11 Snowbird Western Region Tech Series 1/4 - 1/12 Crested Butte USASA Southwest Series Superpipe 1/4 - 1/13 Beaver Creek Ullr Fest 1/4 - 1/14 Steamboat 26th Annual Women's Ski Camp with Deb Armstrong 1/4 - 1/15 Jackson Hole Steep and Deep Ski Camp 1/4 - 1/16 Aspen/Snowmass ESPN Winter X Games 1/4 - 1/17 Steamboat Ski Jam VII 1/16 Winter Park Mary Jane Bump Jamboree 1/16 - 1/18 Jackson Hole JH Ski Club North Series Super G 1/16 - 1/22 Jackson Hole National Safety Awareness Week 1/19 Steamboat 36th Annual Bud Light Cowboy Downhill 1/19 - 1/23 Jackson Hole Women's Ski Camp 1/19 - 1/23 Jackson Hole Women's Snowboard Camp 1/19 - 1/23 Jackson Hole Women's Telemark Camp 1/20 - 1/21 Park City U.S. -

The Avalanche Review a Single Round of Russian P.O
® 6"1 ÊÎä]Ê "°Ê{ÊUÊ*,ÊÓä£Ó RISKRISK TOLTOLERERANCANCEE This HS-N-D3/R3-G/I, about 5' deep, failed on an early season facet layer during the January 18-20 cycle in the Tetons. This northeast-facing bowl in South Fall Creek, elevation approx 9700', is known as “New Years.” Photo by Doug Workman see Teton stories starting on page 14 In This Issue Story by Charlie Ziskin From the President...............................................................2 From the Editor ........................................................................2 Every time an avalanche fatality hits the newswire, the skiing community tries to AAA News......................................................................................3 make some sense out of what happened. Some people want to know precisely what mistakes What’s New . 3 the victims made so they can avoid the same fate. Others want to know how anyone in Snow Science Alta is for Science ......................................................................6 their right mind could even conceive of backcountry skiing in Considerable conditions. The Tipping Point .......................................................................7 Enhanced Avalanche Survival from Airbags ...........8 As someone who often skis pretty big lines under a Considerable forecast, I find myself Kootenay Surface Hoar ....................................................... 10 attempting to explain the process my partners and I employ when making decisions in Crown Profiles Close Call on Petes North .................................................... -

Advanced Ski Mountaineering Course Course Syllabus
Advanced Ski Mountaineering Course Course Syllabus Location and Course Overview This course will take place in the heart of the Beartooth Mountains in Cooke City, Montana. The alpine routes and ski mountaineering objectives in this area are the perfect place to develop the skills necessary to safely climb and ski classic ski mountaineering routes throughout the world. The objective of the course is to climb and ski/snowboard some of the classic ski mountaineering lines in the Beartooths. Course Topics ● Proper use of Ice axe and crampons ● Rope Skills ● Spring weather and snowpack assessment ● Route finding/safe uphill and downhill travel ● Steep Skiing techniques ● Snow climbing and protection ● Goal setting and planning ● Evaluating Avalanche Hazards and terrain risks Course Itinerary Day 1 ● 0800- Meet at Beartooth Powder Guides office at 304 East main Street, across from The Super 8 Motel. Course Overview, introductions, weather forecast/avalanche advisory discussion. ● 0930- Gear check ● 1000- Rest of Day.- Rope skills and steep Skiing workshop workshop to include anchor building, basic knots, belaying and rappelling) Negotiating tricky terrain and downhill skiing management in groups ● 1700- Debrief Day Day 2 ● 0700- Weather and Snowpack discussion. Discuss daily objectives ● 0730- Depart for the day's objective of skiing/riding a “Beartooth Classic Line” If weather and snow stability allows discussion and implementation of ice axes & crampons in appropriate terrain. Discuss, demonstrate and practice self-arrest techniques. Route decisions and conditions will be discussed throughout the day with an emphasis on safe travel techniques in the mountains. Lunch will be in the field. ● 1700- Debrief Day ● 1730- Route planning discussion and trip plan for next day Day 3 ● 0700- Weather and Snowpack discussion. -

Aspen Skiing Company Operations Opening Plan Winter 2020/2021
Aspen Skiing Company Operations Opening Plan Winter 2020/2021 2020/2021 ASPEN SKIING COMPANY OPENING PLAN TABLE OF CONTENTS COVID 19 State & County Guidelines Recommendations .................................................3 State Requirement Grid........................................................................................................4 Expected Operations ............................................................................................................6 Ability to Scale ....................................................................................................................6 Capacity ...............................................................................................................................7 Guest Communications Plan ................................................................................................8 LPHA collaboration .............................................................................................................8 Community Engagement .....................................................................................................9 Operations for On Mountain Divisions..............................................................................10 Mountain Operations o HVAC COVID19 Procedures ..........................................................10 o Product Sales & Services .................................................................12 o Parking & Shuttles ...........................................................................13 o Employee -

Off-Piste Skiing for Mountaineerstrek and Mountain
MountainSkills TRAINING DAYS Skiing for mountaineers Wanting to step up from ski touring to ski mountaineering, Katy Dartford enrolled on a course designed to improve technique in varied terrain and snow conditions... WORDS KATY DARTFORD PICTURES LUKASZ WARZECHA kiing will be the death of British with remote high-mountain descents, far treeline skiing of Les Houches to the Alpinism”, exclaims Andy from the cameras, and often involved a off-piste bowls of the Grands Montets. The Kirkpatrick in his book ‘Cold dangerous technical climb just to access the BASS Chamonix course promises to teach Wars’. In an amusing exchange ski route. This led to th birth 36 years ago how to ski ice, bumps, powder, chopped-up Sbetween himself and British mountain the sport of extreme skiing, when Sylvain powder and whatever other snow you come guide and 11 times Everest summiter, Saudan skied the Spencer Couloir on the across when off-piste, as well as skiing Kenton Cool, Kenton suggests “you Aiguille de Blatiere. For most mountaineers smoothly through trees and tight spaces, should try it mate,” but Andy “doesn’t however, this is the problem. We already and on steep ground. have any time for fun…” have a good understanding of the mountains Andy probably hadn’t tried ski and the hazards they can present – its the WHITE TIME mountaineering, where the pain of an skiing element that we’re worried about! It was one of those ‘white out’ days when arduous climb is rewarded by the freedom our group of six met at Grands Montets, and speed of an off-piste descent from a COURSE OF ACTION with more and more snow falling as the mountain summit. -

Ski Mountaineering Equipment List Ski Gear
Ski Mountaineering Equipment List is extremely important to the success and safety of your course that you bring all the items listed below. The weather can vary dramatically. Be prepared to encounter all types of conditions. Any questions give us a call at: 877-686-2546 The items noted with an * can be provided at no cost by IAG/CAG as noted and are subject to availability. You must notify us no later than 7 days before your trip of any gear you require from us. Please answer the Gear Request Question in your reservation terminal to advise us of any gear you require from us. The examples listed below are suggestions of options for each category and represent the most ideal equipment and clothing items for your trip. However, there are many other options that will also work great, as well! Ski Gear Skis Alpine touring or Telemark skis no wider than 105mm wide underfoot without too much tip and tail rocker. Example: Black Diamond Helio 88 Carbon Ski or Dynafit Tour 88 Ski Women Skins Some ski manufacturers make skins precut for your skis. Otherwise they need to have coverage over most of the ski. The edge needs to be showing but no base showing between the edge of the ski and the skin for about 80% of the skis length. Example: Black Diamond Ascension STS Climbing Skin Bindings Alpine touring or telemark bindings. For AT, the pin style toes are the lightest and tour the best, but there are other styles as well. Example: Salomon S/Lab Shift MNC 13 Ski Boots Lightweight 2-3 buckle touring boots are the best, but any alpine touring or Telemark boot will do.