Pharmacokinetics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1: Clinical Pharmacokinetics 1
1: CLINICAL PHARMACOKINETICS 1 General overview: clinical pharmacokinetics, 2 Pharmacokinetics, 4 Drug clearance (CL), 6 Volume of distribution (Vd), 8 The half-life (t½), 10 Oral availability (F), 12 Protein binding (PB), 14 pH and pharmacokinetics, 16 1 Clinical pharmacokinetics General overview General overview: clinical pharmacokinetics 1 The ultimate aim of drug therapy is to achieve effi cacy without toxicity. This involves achieving a plasma concentration (Cp) within the ‘therapeutic window’, i.e. above the min- imal effective concentration (MEC), but below the minimal toxic concentration (MTC). Clinical pharmacokinetics is about all the factors that determine variability in the Cp and its time-course. The various factors are dealt with in subsequent chapters. Ideal therapeutics: effi cacy without toxicity Minimum Toxic Concentration (MTC) Ideal dosing Minimum Effective Concentration (MEC) Drug concentration Time The graph shows a continuous IV infusion at steady state, where the dose-rate is exactly appropriate for the patient’s clearance (CL). Inappropriate dosing Dosing too high in relation to the patient’s CL – toxicity likely Minimum Toxic Concentration (MTC) Minimum Effective Concentration (MEC) Dosing too low in relation to the Drug concentration patient’s CL – drug may be ineffective Time Some reasons for variation in CL Low CL High CL Normal variation Normal variation Renal impairment Increased renal blood fl ow Genetic poor metabolism Genetic hypermetabolism Liver impairment Enzyme induction Enzyme inhibition Old age/neonate 2 General overview Clinical Pharmacokinetics Pharmacokinetic factors determining ideal therapeutics If immediate effect is needed, a loading dose (LD) must be given to achieve a desired 1 concentration. The LD is determined by the volume of distribution (Vd). -
Prediction of Clinical Transporter‐Mediated Drug–Drug Interactions
Citation: CPT Pharmacometrics Syst. Pharmacol. (2020) 9, 211–221; doi:10.1002/psp4.12505 ARTICLE Prediction of Clinical Transporter-Mediated Drug–Drug Interactions via Comeasurement of Pitavastatin and Eltrombopag in Human Hepatocyte Models Simon J. Carter1, Bhavik Chouhan2, Pradeep Sharma3 and Michael J. Chappell1,* A structurally identifiable micro-rate constant mechanistic model was used to describe the interaction between pitavastatin and eltrombopag, with improved goodness-of-fit values through comeasurement of pitavastatin and eltrombopag. Transporter association and dissociation rate constants and passive rates out of the cell were similar between pitavastatin and eltrom- bopag. Translocation into the cell through transporter-mediated uptake was six times greater for pitavastatin, leading to pronounced inhibition of pitavastatin uptake by eltrombopag. The passive rate into the cell was 91 times smaller for pitavas- tatin compared with eltrombopag. A semimechanistic physiologically-based pharmacokinetic (PBPK) model was developed to evaluate the potential for clinical drug–drug interactions (DDIs). The PBPK model predicted a twofold increase in the pita- vastatin peak blood concentration and area under the concentration-time curve in the presence of eltrombopag in simulated healthy volunteers. The use of structural identifiability supporting experimental design combined with robust micro-rate con- stant parameter estimates and a semimechanistic PBPK model gave more informed predictions of transporter-mediated DDIs. Study Highlights WHAT IS THE CURRENT KNOWLEDGE ON THE TOPIC? model fits through micro-rate constants compared with ✔ Currently, most in vitro models are not guided by macro-rate constants in human hepatocytes, with addi- structural identifiability analysis, relying on substrate-only tional information provided regarding transporter binding. -

Pharmacokinetics, Biodistribution, and Pharmacodynamics of Drug Delivery Systems
JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. The final version may differ from this version. JPET # 257113 Title: Pharmacokinetic and Pharmacodynamic Properties of Drug Delivery Systems Authors: Patrick M. Glassman, Vladimir R. Muzykantov Affiliation: Department of Systems Pharmacology and Translational Therapeutics, Perelman School of Medicine, University of Pennsylvania Address: 3400 Civic Center Boulevard, Bldg 421, Philadelphia, Pennsylvania 19104-5158, United States Downloaded from jpet.aspetjournals.org at ASPET Journals on September 24, 2021 1 JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. The final version may differ from this version. JPET # 257113 Running Title: PK/PD Properties of Drug Delivery Systems Corresponding Authors: Vladimir R. Muzykantov ([email protected], (215) 898-9823) and Patrick M. Glassman ([email protected]) # of Text Pages: 22 # of Tables: 2 # of Figures: 4 Word Count – Abstract: 144 Word Count – Introduction: 350 Word Count – Discussion: N/A Downloaded from Non-Standard Abbreviations: Absorption, Distribution, Metabolism, and Elimination (ADME) Biodistribution (BD) Drug Delivery Systems (DDSs) Enhanced Permeability & Retention (EPR) jpet.aspetjournals.org Gastrointestinal (GI) Intravenously (IV) Neonatal Fc Receptor (FcRn) Monoclonal Antibody (mAb) Reticuloendothelial System (RES) at ASPET Journals on September 24, 2021 Pharmacodynamics (PD) Pharmacokinetics (PK) Physiologically-Based Pharmacokinetic (PBPK) Subcutaneously (SC) Target-Mediated Drug Disposition (TMDD) Recommended Section: Drug Discovery and Translational Medicine 2 JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. -

Multidrug-Resistant Gram-Negative Bacteria
Multidrug-Resistant Gram-Negative Bacteria: Trends, Risk Factors, and Treatments A worldwide public health problem, antibiotic resistance leads to treatment-resistant infections associated with prolonged hospitalizations, increased cost, and greater risk for morbidity. Lee S. Engel MD, PhD CASE INTRODUCTION An 80-year-old female nursing home resident with Antibiotics have saved the lives of millions of people a history of dementia, anemia, atrial fibrillation, and have contributed to the major gains in life ex- hypertension, incontinence, and recurrent urinary pectancy over the last century. In US hospitals, 190 tract infections (UTIs), as well as a long-term Foley million doses of antibiotics are administered each catheter, is admitted because she was found to be day.1 Furthermore, more than 133 million courses febrile and less responsive than normal. The patient of antibiotics are prescribed each year for outpatients. has no drug allergies. Upon admission, she has a However, antibiotic use has also resulted in a major temperature of 38.9ºC, heart rate of 92 beats/min, health care challenge—the development and spread and blood pressure of 106/64 mm Hg. The patient of resistant bacteria. Worldwide, antimicrobial resis- opens her eyes to stimuli but does not speak. Aside tance is most evident in diarrheal diseases, respira- from poor dentition and an irregular heart rate, tory tract infections, meningitis, sexually transmitted findings on physical examination, which includes infections, and hospital and health care–acquired in- a pulmonary and abdominal examination, are nor- fections.2 Vancomycin-resistant enterococci, methi- mal. Serum chemistries demonstrate a white blood cillin-resistant Staphylococcus aureus, multidrug-resis- cell (WBC) count of 11,300 cells/mm3. -

Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development
Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development Gerlie Gieser, Ph.D. Office of Clinical Pharmacology, Div. IV Objectives • Outline the Phase 1 studies conducted to characterize the Clinical Pharmacology of a drug; describe important design elements of and the information gained from these studies. • List the Clinical Pharmacology characteristics of an Ideal Drug • Describe how the Clinical Pharmacology information from Phase 1 can help design Phase 2/3 trials • Discuss the timing of Clinical Pharmacology studies during drug development, and provide examples of how the information generated could impact the overall clinical development plan and product labeling. Phase 1 of Drug Development CLINICAL DEVELOPMENT RESEARCH PRE POST AND CLINICAL APPROVAL 1 DISCOVERY DEVELOPMENT 2 3 PHASE e e e s s s a a a h h h P P P Clinical Pharmacology Studies Initial IND (first in human) NDA/BLA SUBMISSION Phase 1 – studies designed mainly to investigate the safety/tolerability (if possible, identify MTD), pharmacokinetics and pharmacodynamics of an investigational drug in humans Clinical Pharmacology • Study of the Pharmacokinetics (PK) and Pharmacodynamics (PD) of the drug in humans – PK: what the body does to the drug (Absorption, Distribution, Metabolism, Excretion) – PD: what the drug does to the body • PK and PD profiles of the drug are influenced by physicochemical properties of the drug, product/formulation, administration route, patient’s intrinsic and extrinsic factors (e.g., organ dysfunction, diseases, concomitant medications, -

624.Full.Pdf
1521-009X/44/5/624–633$25.00 http://dx.doi.org/10.1124/dmd.115.068932 DRUG METABOLISM AND DISPOSITION Drug Metab Dispos 44:624–633, May 2016 Copyright ª 2016 by The American Society for Pharmacology and Experimental Therapeutics Development of a Rat Plasma and Brain Extracellular Fluid Pharmacokinetic Model for Bupropion and Hydroxybupropion Based on Microdialysis Sampling, and Application to Predict Human Brain Concentrations Thomas I.F.H. Cremers, Gunnar Flik, Joost H.A. Folgering, Hans Rollema, and Robert E. Stratford, Jr. Brains On-Line BV, Groningen, The Netherlands (T.I.F.H.C., G.F. J.H.A.F.); Rollema Biomedical Consulting, Mystic, Connecticut (H.R.); and Division of Pharmaceutical Sciences, Mylan School of Pharmacy, Duquesne University, Pittsburgh, Pennsylvania (R.E.S.) Received December 11, 2015; accepted February 24, 2016 Downloaded from ABSTRACT Administration of bupropion [(6)-2-(tert-butylamino)-1-(3-chlorophenyl) concentration ratio at early time points was observed with propan-1-one] and its preformed active metabolite, hydroxybupropion bupropion; this was modeled as a time-dependent uptake clear- [(6)-1-(3-chlorophenyl)-2-[(1-hydroxy-2-methyl-2-propanyl)amino]- ance of the drug across the blood–brain barrier. Translation of the 1-propanone], to rats with measurement of unbound concentrations model was used to predict bupropion and hydroxybupropion dmd.aspetjournals.org by quantitative microdialysis sampling of plasma and brain extra- exposure in human brain extracellular fluid after twice-daily cellular fluid was used to develop a compartmental pharmacoki- administration of 150 mg bupropion. Predicted concentrations netics model to describe the blood–brain barrier transport of both indicate that preferential inhibition of the dopamine and norepi- substances. -

Antimicrobial Stewardship Guidance
Antimicrobial Stewardship Guidance Federal Bureau of Prisons Clinical Practice Guidelines March 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant these guidelines for any other purpose, and assumes no responsibility for any injury or damage resulting from the reliance thereof. Proper medical practice necessitates that all cases are evaluated on an individual basis and that treatment decisions are patient-specific. Consult the BOP Clinical Practice Guidelines Web page to determine the date of the most recent update to this document: http://www.bop.gov/news/medresources.jsp Federal Bureau of Prisons Antimicrobial Stewardship Guidance Clinical Practice Guidelines March 2013 Table of Contents 1. Purpose ............................................................................................................................................. 3 2. Introduction ...................................................................................................................................... 3 3. Antimicrobial Stewardship in the BOP............................................................................................ 4 4. General Guidance for Diagnosis and Identifying Infection ............................................................. 5 Diagnosis of Specific Infections ........................................................................................................ 6 Upper Respiratory Infections (not otherwise specified) .............................................................................. -

A Primer on Pharmacology
A primer on pharmacology Universidade do Algarve Faro 2017 by Ferdi Engels, Ph.D. 1 2 1 3 Utrecht university campus ‘de Uithof’ Dept. of Pharmaceutical Sciences Division of Pharmacology 4 2 Bachelor and master education Ferdi Engels, PhD ‐ Associate professor of pharmacology ‐ Director of Undergraduate School of Science PhD training Research expertise 5 for today 1. Understand the main concepts of pharmacokinetics Main concept 2. Be able to apply this new knowledge 6 3 Pharmacology is about drugs………. Drugs = chemicals that alter physiological processes in the body for treatment, prevention, or cure of diseases input output (administration of the drug) (biological response) ‐ dose ‐ no effect ‐ frequency of administration ‐ beneficial effects ‐ route of administration ‐ adverse / toxic effects onset, intensity, and duration of therapeutic effects 7 Pharmacology is about drugs………. Drugs = chemicals that alter physiological processes in the body for treatment, prevention, or cure of diseases What does the body do to the drug? pharmacokinetics What does the drug do to the body? pharmacodynamics 8 4 Thursday, June 15 Lecture on topic 1 Workshop on topic 1 Friday, June 16 Lecture on topic 2 Workshop on topic 2 Course Topic 1 Course Topic 2 9 Rosenbaum ‐ Basic pharmacokinetics and pharmacodynamics: an integrated textbook and computer simulations, 1st ed. (2011) input output (administration of the drug) (biological response) ‐ dose ‐ no effect ‐ frequency of administration ‐ beneficial effects ‐ route of administration ‐ adverse / toxic effects -

Mechanism-Based Inactivation of Human Cytochrome P450 Enzymes and the Prediction of Drug-Drug Interactions□S
Supplemental material to this article can be found at: http://dmd.aspetjournals.org/content/suppl/2006/11/08/dmd.106.012633.DC1.html 0090-9556/07/3502-246–255$20.00 DRUG METABOLISM AND DISPOSITION Vol. 35, No. 2 Copyright © 2007 by The American Society for Pharmacology and Experimental Therapeutics 12633/3169778 DMD 35:246–255, 2007 Printed in U.S.A. Mechanism-Based Inactivation of Human Cytochrome P450 Enzymes and the Prediction of Drug-Drug Interactions□S R. Scott Obach, Robert L. Walsky, and Karthik Venkatakrishnan Pharmacokinetics, Dynamics, and Drug Metabolism (R.S.O., R.L.W.) and Clinical Pharmacology (K.V.), Pfizer, Inc., Groton, Connecticut Received August 30, 2006; accepted November 2, 2006 ABSTRACT: The ability to use vitro inactivation kinetic parameters in scaling to proaches to identifying mechanism-based inactivators were devel- in vivo drug-drug interactions (DDIs) for mechanism-based inacti- oped. Testing potential inactivators at a single concentration (IC25) vators of human cytochrome P450 (P450) enzymes was examined in a 30-min preincubation with human liver microsomes in the Downloaded from using eight human P450-selective marker activities in pooled hu- absence and presence of NADPH followed by assessment of P450 man liver microsomes. These data were combined with other pa- marker activities readily identified those compounds known to be rameters (systemic Cmax, estimated hepatic inlet Cmax, fraction mechanism-based inactivators and represents an approach that unbound, in vivo P450 enzyme degradation rate constants -

1. Disposition and Pharmacokinetics
1. DISPOSITION AND PHARMACOKINETICS The disposition and pharmacokinetics of 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and related compounds have been investigated in several species and under various exposure conditions. Several reviews on this subject focus on TCDD and related halogenated aromatic hydrocarbons (Neal et al., 1982; Gasiewicz et al., 1983a; Olson et al., 1983; Birnbaum, 1985; van den Berg et al., 1994). The relative biological and toxicological potency of TCDD and related compounds depends not only on the affinity of these compounds for the aryl hydrocarbon receptor (AhR), but on the species-, strain-, and congener-specific pharmacokinetics of these compounds (Neal et al., 1982; Gasiewicz et al., 1983a; Olson et al., 1983; Birnbaum, 1985; van den Berg et al., 1994, DeVito and Birnbaum, 1995). 2,3,7,8-TCDD and other similar compounds discussed here are rapidly absorbed into the body and slowly eliminated, making body burden (bioaccumulation) a reliable indicator of time- integrated exposure and absorbed dose. Because of the slow elimination kinetics, it will be shown in this section that lipid or blood concentrations, which are often measured, are in dynamic equilibrium with other tissue compartments in the body, making the overall body burden and tissue disposition relatively easy to estimate. Finally, it will be shown that body burdens can be correlated with adverse health effects (Hardell et al., 1995; Leonards et al., 1995), further leading to the choice of body burden as the optimal indicator of absorbed dose and potential effects. 1.1. ABSORPTION/BIOAVAILABILITY FOLLOWING EXPOSURE Gastrointestinal, dermal, and transpulmonary absorptions represent potential routes for human exposure to this class of persistent environmental contaminants. -

General a Number of Factors Could Reduce the Efficacy of This
AUSTRALIAN PRODUCT INFORMATION Administration It is strongly recommended that every time that GAMUNEX® is administered to a patient, the name Use in the elderly GAMUNEX® If dilution is required, GAMUNEX® may be diluted with 5% dextrose in water (D5/W). Do not and batch number of the product are recorded using the supplied tear off labels in order to maintain See Section 4.4 Special warnings and precautions for use: Use in renal impairment. a link between the patient and the batch of the product. (NORMAL IMMUNOGLOBULIN (HUMAN), 10%, INTRAVENOUS SOLUTION VIAL) dilute with saline. Paediatric use Anaphylaxis GAMUNEX® should be inspected visually for particulate matter and discoloration prior to adminis - No data available. GAMUNEX® should be administered only intravenously or subcutaneously. On rare occasions, tration, whenever solution and container permit. Do not use if turbid and/or if discoloration is Effects on laboratory tests 1 NAME OF THE MEDICINE observed. treatment with an immune globulin preparation may cause a precipitous fall in blood pressure and a Interference with serological testing Normal immunoglobulin (Human), 10%, for Intravenous or Subcutaneous Administration For intravenous or subcutaneous administration, GAMUNEX® should be at room temperature during clinical picture of anaphylaxis, even when the patient is not known to be sensitive to immune globulin administration. preparations. Adrenalin and other appropriate supportive care should be available for the treatment After injection of immunoglobulin the transitory rise of the various passively transferred antibodies of an acute anaphylactic reaction. in the patient’s blood may result in misleading positive results in serological testing. Passive Intravenous (IV) True anaphylactic reactions to GAMUNEX® may occur in recipients with documented prior histories transmission of antibodies to erythrocyte antigens e.g. -
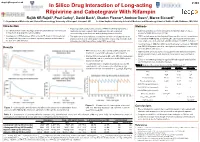
No Slide Title
[email protected] In Silico Drug Interaction of Long-acting # 458 Rilpivirine and Cabotegravir With Rifampin Rajith KR Rajoli1, Paul Curley1, David Back1, Charles Flexner2, Andrew Owen1, Marco Siccardi1 1 - Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, UK 2- Johns Hopkins University School of Medicine and Bloomberg School of Public Health, Baltimore, MD, USA Introduction Methods • Physiologically-based pharmacokinetic (PBPK) modelling represents a • Co-administration of anti-TB drugs and many antiretrovirals (ARVs) result mathematical tool to predict DDI magnitude through a detailed • 100 virtual individuals were simulated using Simbiology v.4.3.1, a in important drug-drug interactions (DDIs) understanding of mechanisms underpinning pharmacokinetics product of MATLAB (version 2013b) • Investigation of DDIs between ARVs and anti-TB drugs in individuals can • The objective of this study was to simulate the effect of rifampicin on the • PBPK models were qualified against literature data for oral formulations be complicated by numerous clinical, logistical barriers and also due to pharmacokinetics of cabotegravir and rilpivirine long-acting injectable (LAI) of rifampicin (600 mg OD, at day 6 & 14), cabotegravir and rilpivirine the risk of treatment failure intramuscular (IM) formulations using PBPK modelling (oral, single dose & steady state and IM compared to LATTE-2 studies)1-4 • Loading doses of 800 mg, 900 mg and maintenance doses of 400/800 Results mg, 600/900 mg were used for cabotegravir