Fraser Health Authority
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
AUTHORIZATION for the RELEASE of HEALTH RECORDS Please Fax Or Mail Your Completed Request to Each Hospital/Facility You Are Requesting Records From
AUTHORIZATION FOR THE RELEASE OF HEALTH RECORDS Please fax or mail your completed request to each hospital/facility you are requesting records from. ATTENTION: Health Information Management, Release of Information Office Part 1. Patient / Resident Information LAST NAME OF PATIENT FIRST NAME ALSO KNOWN AS / ALIAS MAILING ADDRESS CITY / PROVINCE / COUNTRY POSTAL CODE TELEPHONE NO. (INCLUDING AREA CODE) DATE OF BIRTH DAY | MONTH | YEAR PERSONAL HEALTH NUMBER (CARECARD) | | Part 2. Records Requested HOSPITAL(S)/FACILITY: □ VISIT SUMMARY □ EMERGENCY VISIT INFORMATION □ DIAGNOSTIC REPORTS (LAB/RADIOLOGY) □ PROOF OF VISIT □ OUTPATIENT □ OTHER (PLEASE SPECIFY): (fees may apply) DATE(S) OF RECORDS REQUESTED: ______________________ TO ___________________________________________ If you do not know exact dates please provide your best estimate Part 3. Person Receiving Records □ MYSELF OR □ NAME OF PERSON RECEIVING THE RECORDS NAME OF COMPANY OR ORGANIZATION (IF APPLICABLE) (LAST, FIRST) MAILING ADDRESS CITY / PROVINCE / COUNTRY POSTAL CODE TELEPHONE NO. (INCLUDING AREA CODE) RECORDS TO BE: □ MAILED □ PICKED UP (Picture ID Required) Part 4. Patient Authorization (12 years of age or older) I, the patient, authorize the Hospital(s)/Facility to release the records requested to the person named in the “Person Receiving Records” section. SIGNATURE OF PATIENT: ___________________________________________ DATE SIGNED: ____________________________ Part 5. Authorization on behalf of Patient (Please complete page 2 of form) (If patient is under 12 years of age or unable to authorize the release of personal information.) By signing below I confirm that I have legal authority to act on behalf of the patient and I hereby authorize the Hospital(s)/Facility to release the records requested to the person named in the “Person Receiving Records” section. -
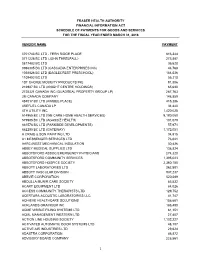
2018 Schedule of Vendor Payments.Xlsx
FRASER HEALTH AUTHORITY FINANCIAL INFORMATION ACT SCHEDULE OF PAYMENTS FOR GOODS AND SERVICES FOR THE FISCAL YEAR ENDED MARCH 31, 2018 VENDOR NAME PAYMENT 0701743 BC LTD - FERN RIDGE PLACE 816,344 0771226 BC LTD (JOHN THRELFALL) 273,887 0817482 BC LTD 36,628 0986305 BC LTD (CASCADIA ENTERPRISES INC) 44,768 1038826 BC LTD (EAGLECREST PRESCHOOL) 184,036 1109402 BC LTD 56,210 1ST CHOICE MOBILITY PRODUCTS INC 91,806 216987 BC LTD (KNIGHT CENTRE HOLDINGS) 65,630 2725321 CANADA INC (QUADREAL PROPERTY GROUP LP) 287,763 3M CANADA COMPANY 148,859 484017 BC LTD (KIMBEE PLACE) 415,386 4REFUEL CANADA LP 34,440 4TH UTILITY INC 1,420,028 514965 BC LTD (WE CARE HOME HEALTH SERVICES) 9,180,060 579985 BC LTD (AGASSIZ HEALTH) 101,079 661576 BC LTD (PARKSIDE DEVELOPMENTS) 57,971 662290 BC LTD (GATEWAY) 1,172,051 A CRAIG & SON PAINTING LTD 34,915 A1 MESSENGER SERVICES LTD 76,041 AARC-WEST MECHANICAL INSULATION 30,426 ABBEY MEDICAL SUPPLIES LTD 138,824 ABBOTSFORD ASSOC EMERGENCY PHYSICIANS 274,320 ABBOTSFORD COMMUNITY SERVICES 1,395,023 ABBOTSFORD HOSPICE SOCIETY 2,360,180 ABBOTT LABORATORIES LTD 262,801 ABBOTT VASCULAR DIVISION 937,237 ABBVIE CORPORATION 520,589 ABDULLA MUNIR CARE SOCIETY 85,532 ACART EQUIPMENT LTD 84,026 ACCESS COMMUNITY THERAPISTS LTD 129,752 ACERTARA ACOUSTIC LABORATORIES LLC 41,747 ACHIEVE HEALTHCARE SOLUTIONS 158,681 ACKLANDS-GRAINGER INC 185,490 ACME VISIBLE FILING SYSTEMS LTD 81,151 ACML MANAGEMENT WESTERN LTD 27,457 ACTION LINE HOUSING SOCIETY 1,102,227 ACTIVATED AUTOMATIC DOOR SYSTEMS LTD 48,107 ACTIVE AIR INDUSTRIES LTD 29,624 -

Residential Care in Fraser Health
RESIDENTIAL CARE i n FRASER HEALTH Choices for adults who need 24-hour nursing care, personal care assistance and support TABLE OF CONTENTS About residential care 1 Options for residential care Subsidized 2 Private Pay 3 The first step toward moving to subsidized residential care Moving from home 4 Moving from hospital or temporary care 5 Preparing for the move to a residential care facility Before the move 6 Settling into the residential care setting 7 Moving to another residential care facility or to more independent living 8 Typical living costs in residential care 8 Some commonly used terms 9 Notes 11 Further Information inside back cover RESIDENTIAL CARE i n FRASER HEALTH About residential care IS RESIDENTIAL CARE THE RIGHT CHOICE? When a person’s ongoing health care needs become more complex, When the amount of daily a residential care facility may become the best health care choice. care needed is more than Residential care is sometimes also referred to as intermediate care, can be safely managed at extended care, special care or a nursing home. home, or in a supportive Residential care provides: or assisted living setting, a safe and secure living environment residential care may be 24-hour nursing care, personal care the most appropriate assistance and support nutritious meals care option. basic linen and personal laundry services recreational and activity programs Fraser Health operates and funds many residential care facilities, which together accommodate more than 7,500 adults throughout Fraser Health communities. All residential facilities in British Columbia operate within and provide care that meets established standards. -

Births by Facility 2015/16
Number of Births by Facility British Columbia Maternal Discharges from April 1, 2015 to March 31, 2016 Ü Number of births: Fort Nelson* <10 10 - 49 50 - 249 250 - 499 500 - 999 Fort St. John 1,000 - 1,499 Wrinch Dawson Creek 1,500 - 2,499 Memorial* & District Mills Chetwynd * ≥ 2,500 Memorial Bulkley Valley MacKenzie & 1,500-2,499 Stuart Lake Northern Prince Rupert District * Births at home with a Haida Gwaii* University Hospital Registered Healthcare Provider of Northern BC Kitimat McBride* St. John G.R. Baker Memorial Haida Gwaii Shuswap Lake General 100 Mile District Queen Victoria Lower Mainland Inset: Cariboo Memorial Port Golden & District McNeill Lions Gate Royal Invermere St. Paul's Cormorant Inland & District Port Hardy * Island* Lillooet Ridge Meadows Powell River Vernon VGH* Campbell River Sechelt Kootenay Elk Valley Burnaby Lake Squamish Kelowna St. Joseph's General BC Women's General Surrey Penticton Memorial West Coast East Kootenay Abbotsford Royal General Regional Richmond Columbian Regional Fraser Creston Valley Tofino Canyon * Peace Langley Nicola General* Boundary* Kootenay Boundary Arch Memorial Nanaimo Lady Minto / Chilliwack Valley * Regional Gulf Islands General Cowichan Saanich District Victoria 0 62.5 125 250 375 500 Peninsula* General Kilometers * Hospital does not offer planned obstetrical services. Source: BC Perinatal Data Registry. Data generated on March 24, 2017 (from data as of March 8, 2017). Number of Births by Facility British Columbia, April 1, 2015 - March 31, 2016 Facility Community Births 100 Mile -

It's Our Time Under the Lights
ROYAL COLUMBIAN HOSPITAL FOUNDATION N atio ND fou L ita P os N H ia B um L co L oya IMAGE COURTESY OF R Royal Columbian Hospital is one of B.C.’s top critical care hospitals, serving a population of It’s Our Time more than 1.8 million people — one in three British Under the Lights Columbians. Traditionally B.C.’s unsung hero of healthcare, Royal Columbian Hospital has begun an unprecedented and transformational redevelopment ospital upgrades are always an comprise the largest government-funded Royal Columbian, which is also the important undertaking, as well health care redevelopment project ever province’s oldest hospital (established in as being elaborate in terms of approved in B.C. — are for the only hospital 1862); but the bottom line is that with it logistics. But the impact of the in the province with Level 1 trauma, cardiac serving about one third of the total three-phase, $1.35-billion care, neurosurgery, high-risk obstetrics, population of B.C., the upgrades — Phase 1 improvement for New Westmin- neonatal intensive care, and acute mental- of which is already underway — will take Hster-based Royal Columbian Hospital is health care services, all on one site. Royal these services to stratospheric new heights. such that it recently prompted Tom Columbian is B.C.’s busiest cardiac care As far as Royal Columbian site medical Sparrow, the hospital’s redevelopment centre; it is the only hospital in B.C. that director and critical care physician Dr. chief project officer, to remark, “What’s cares for certain critically ill pregnant Steve Reynolds is concerned, the upgrades taking place is spectacular and of significant women and their unborn children; and it is are also drawing much-needed attention to benefit to New Westminster, Metro one of the province’s busiest emergency the hospital’s achievements. -

Working Group DE Report, and the Working Group DE Report Resulting from the Fraser Health Authority Review
Memorandum Ministry of Health Office of the Deputy Minister June 2014 To: Honourable Terry Lake Minister of Health Re: Fraser Health Authority Review I am pleased to transmit for your consideration a summary of Working Group DE Report, and the Working Group DE Report resulting from the Fraser Health Authority Review. The review committee was guided by the Fraser Health Authority Special Directions Regulation which, in addition to a variety of other requirements, instructed the committee to consider the relationship of Fraser Health and neighbouring health authorities in the lower mainland. Specifically, the regulation states: (d) whether there is duplication or redundancy in the delivery of health programs and services between the board and neighbouring regional health boards; (e) whether the health needs of the region's population would be met more effectively or efficiently by changing the area of British Columbia that constitutes the region; In executing the mandate set out in clause (d), the Working Group focused its analysis on duplication and redundancy in select high intensity services (trauma, stroke and cardiac) and on academic health science activities. In its evaluation of regional considerations as described in clause (e), the Working Group sought to explore and understand the health needs and current utilization patterns of patients originating in Fraser Health. The analysis has resulted in ten recommendations which range from system-level strategic direction to site-specific actions. The recommendations highlight a number of meaningful opportunities for Fraser Health to work collaboratively with Vancouver Coastal and the Provincial Health Services Authority to improve sector planning, and service and program delivery activities. -

Surrey Memorial Hospital Emergency Department And
LOCATION ARCHITECTS SURREY MEMORIAL Surrey, British Columbia CEI Architecture Planning Interiors; Parkin Architects SIZE HOSPITAL 59,400 m2 WOOD SUPPLIER StructureCraft Builders Inc. CAPACITY EMERGENCY 151 additional beds (including ENGINEER intensive care), expanded Bush Bohlman and Partners laboratory, added academic space DEPARTMENT AND B.C. GOVERNMENT MINISTRY COMPLETION Ministry of Health CRITICAL CARE TOWER 2013 Project Overview Visiting a hospital can be a stressful experience, so when the visual presence of wood in a room is both psychologically and British Columbia Ministry of Health was designing the Surrey physiologically beneficial2. Memorial Hospital expansion, the architects were asked to When construction began in 2011, the Emergency Department come up with a warm, natural facility that would also meet and Critical Care Tower expansion was the largest health care rigorous building performance demands. project in the history of British Columbia, serving Fraser To achieve these ends, the design used wood in structural and Health Authority’s fastest growing community. The project decorative components. The lobby features exposed wood adds acute care beds, a new emergency department, a and provides a sense of calm for all in a stressful environment. specialized mental health and pediatric area, an adult Wood use throughout the public areas of the hospital intensive care unit, a neonatal centre of excellence, more expansion reinforces the connection to nature, helping to space for the clinical academic campus of the University of reduce stress and anxiety for both visitors and patients1. British Columbia’s School of Medicine, and a laboratory with the latest medical technology. Research shows people respond emotionally to wood and are attracted to its visual variety and natural expressiveness; the Photos: Ed White Photographics, courtesy of CEI Architecture and Parkin Architects “The use of exposed wood in a project is one of the ways that we can improve conditions for our patients. -

Fraser Health Together
Fraser Health Together Fraser Health’s online booking tool is going through important maintenance to ensure there is a comprehensive transition to the provincial online booking and registration system set to launch on April 6th. This information is for your convenience please click on the link to be directed to the Fraser Health website for the most current updates: https://www.fraserhealth.ca/vaccine#.YGS-6a9KiUn Booking your immunization appointment if you live in the Fraser Health region Effective immediately, and until 7:00 a.m. on April 6, eligible people in the Fraser Health region* who would like to book their COVID-19 immunization appointment can do so one of two ways: • Between 7:00 am and 7:00 p.m. (Daytime): Call our immunization booking phone line at 1-855-755-2455. The phone line will operate from 9:00 a.m. to 5:00 p.m. on Friday, April 2 and Monday, April 5 to align with the statutory holidays. • Between 7:00 pm and 7:00 a.m. (Nighttime): Access Fraser Health’s self-serve online booking tool. The online tool will operate from 5:00 p.m. to 9:00 a.m. on Friday, April 2 and Monday, April 5. On Saturday, April 3 and Sunday, April 4 it will run from 7:00 pm to 7:00 am. To date we have booked just over 222,070 immunization appointments and we acknowledge that people in our communities want to book appointments as quickly as they become eligible. We appreciate everyone’s patience as we schedule very sizable populations into immunization appointments. -

COVID-19 School Cluster and Transmission Analysis
COVID-19 school cluster and transmission analysis May 7, 2021 1 Purpose Retrospective analysis of COVID-19 cases in K-12 school settings to determine clusters and transmission dynamics 2 Inclusion criteria COVID-19 cases reported to Public Health between January 1 and March 7, 2021 in students and staff who attended school (K- 12 public/independent) 3 Methods . Identified all schools with >1 case within a 14-day period (excluding cases from the same household) . Determined whether in-school transmission occurred based on standardized transmission/acquisition definitions . Cases reviewed by team of epidemiologists, analysts and MHO over 6 week period . MHO consulted for complex and ambiguous cases 4 Definitions . Suspect in-school acquisition/transmission defined as: . Case attended school during acquisition period . Case has no known exposure to a household or community case with symptom onset two or more days earlier . Possible in-school acquisition/transmission event defined as: . Suspect definition above AND . When 2 or more cases within the same classroom/admin areas/school bus/other school supervised venue or activity or with confirmed contact between cases in school based setting with similar symptom onset within 2 calendar day window without any other known acquisition . Likely in-school acquisition/transmission defined as: . Suspect definition above AND . Acquisition period of case overlaps with infectious period of another case in the same classroom/admin areas/school bus/other school supervised venue or activity or with confirmed contact between cases in school based setting *Does not include cases who were en route to school together (e.g. car-pooled or walking – excludes school bus use) as these are considered as community transmission and not issues with school based safety measures. -

BCNU - EDMP Contact List
BCNU - EDMP Contact List Representative Region Sites Vancouver Coastal (VCHA) Dawn Tonge Coastal Mountain/ Richmond: Acute, Community & [email protected] RIVA Long-Term Care (Minoru, Lions Cell: 604 862 1063 Manor), Lions Gate Hospital, Sunshine Coast-Sechelt, Powell River, Whistler, Pemberton/ Squamish, Bella Bella, Bella Coola Silvia Kuntze Central Vancouver/ Vancouver Acute, UBC, TCU– [email protected] RIVA Koerner Pavilion, Mary Pack, Cell: 604 862 0186 Broadway Corporate Offices, CST, Tertiary Mental Health (Willow/Segal), Banfield Jaspreet Gill Central Vancouver/ Community Care, George [email protected] RIVA Pearson Centre, G.F. Strong Cell: 604 312 0826 Vancouver Island (VIHA) Elaine Greer South Islands Victoria (except RJH & Mental [email protected] Health), SPH, Lady Minto, PHS Cell: 250 889 0228 Holly Anderson Pacific Rim NRGH, Oceanside, Port Alberni [email protected] (except Westhaven), Tofino/ Cell: 250 713 8772 Ucleulet, Comox/Courtenay, Campbell River, Mt. Waddington Laura Rachwalski Pacific Rim/ RJH, Victoria Mental Health (all [email protected] South Islands sites & programs), Duncan, Cell: 250 893 1774 Chemainus, Ladysmith, Nanaimo (except NRGH), Trillium, Westhaven, Eagle Park Fraser Health (FHA) Nicole Ng Fraser Valley/ Ridge Meadows Hospital, ARH, [email protected] South Fraser Valley/ Abbotsford Community, Langley Cell: 604 785 7644 Simon Fraser Memorial Hospital, Langley Community, Cottage/Worthington October 2020 Representative Region Sites Cathy Ellen Queen South Fraser Valley Delta Hospital -

Trauma Services BC a Service of the Provincial Health Services Authority Contents
2015 ANNUAL REPORT Trauma Services BC A service of the Provincial Health Services Authority Contents 3 Foreword 4 Overview 5 BC’s system of organized trauma care 6 Trauma Services BC 7 Vision for BC’s trauma system 8 Governance 9 Trauma Services BC council 10 Strategic plan (2014-2016) 11 Partnerships & collaborations 12 BC Trauma Registry 13 Overview 14 Registry data quality monitoring 15 BC Trauma Registry operations 16 Key achievements 17 Future plans 18 Mechanism of Injury – Provincial overview 19 Regional health authority and partners trauma program report 20 Fraser Health 22 Interior Health 24 Island Health 26 Northern Health 28 Vancouver Coastal Health 30 BC Children’s Hospital 32 Special initiatives 33 Specialist Services Committee Project 34 Performance monitoring & evaluation plan 36 Accreditation Canada Trauma Distinction program 38 Looking forward 40 References and photo credits 42 Appendices 43 Appendix 1 – Inclusion/exclusion criteria for the BC Trauma Registry 44 Appendix 2 – Data quality 46 Appendix 3 – BC trauma program membership Foreword The 2015 annual report describes events and activities Our editor “in-situ” Mr. Beide Bekele, Trauma Services that took place within the calendar year supported by BC’s project manager, who discretely pushed us data from 2013/14. 2015 has been an exciting year of on timelines, content and continuity while working acquisition and building infrastructure for Trauma Services with our graphic artist, Mr. Ernest Stelzer, and PHSA BC with a strategic focus on advancing: communications, all of whom contributed to the look • Optimal service delivery for BC residents reflected in and tone of the report. -

Fraser Valley Rotation (FVR) (Burnaby General Hospital, Surrey Memorial Hospital, Royal Columbian Hospital, Eagle Ridge Hospital
THE UNIVERSITY OF BRITISH COLUMBIA Department of Urologic Sciences Faculty of Medicine Gordon & Leslie Diamond Health Care Centre Level 6, 2775 Laurel Street Vancouver, BC, Canada V5Z 1M9 Tel: (604) 875-4301 Fax: (604) 875-4637 Fraser Valley Rotation (FVR) (Burnaby General Hospital, Surrey Memorial Hospital, Royal Columbian Hospital, Eagle Ridge Hospital) Rotation Goals & Objectives Preamble: General Objectives The elective at FVR provides training in both pediatric and adult general and specialty urology. There is a particular emphasis on laparoscopic, genitourinary reconstructive surgery for renal and pelvic disorders. There is also training in broad-based, general urologic practice including uro- oncology, reconstructive surgery for male/female incontinence, benign prostatic diseases, congenital reconstruction, and men’s health. The resident will be evaluated according to the goals and objectives appropriate for his/her level. The “elective” at FVR is better described as a longitudinal experience. A resident will typically spend one or more elective blocks in a senior role. An ITER will be issued at the end of each block and the resident will utilize these rotations in order to amass ongoing competencies required for progressive achievement in the Program. It should be recognized that much of the teaching during this elective will occur during, or a result of, direct patient care. The resident will recognize that their own education is intricately linked to delivery of patient care and that, through service, their education will be optimized. SPH/MSJ Goals and Objectives This document refers to the RCPSC Objectives of Training in Urology (2009) Locations Burnaby General Hospital is located in Burnaby, British Columbia and is a large 314 bed community hospital affiliated with UBC.