A Descriptive Mixed-Methods Study Examining Resilience and Transitioning to Adulthood Among Emerging Adults with Disabilities Jennifer Emilie Mannino Ph.D., R.N
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Descriptive AI Ethics: Collecting and Understanding the Public Opinion
Descriptive AI Ethics: Collecting and Understanding the Public Opinion GABRIEL LIMA, School of Computing, KAIST and Data Science Group, IBS, Republic of Korea MEEYOUNG CHA, Data Science Group, IBS and School of Computing, KAIST, Republic of Korea There is a growing need for data-driven research efforts on how the public perceives the ethical, moral, and legal issues of autonomous AI systems. The current debate on the responsibility gap posed by these systems is one such example. This work proposes a mixed AI ethics model that allows normative and descriptive research to complement each other, by aiding scholarly discussion with data gathered from the public. We discuss its implications on bridging the gap between optimistic and pessimistic views towards AI systems’ deployment. 1 INTRODUCTION In light of the significant changes artificial intelligence (AI) systems bring to society, many scholars discuss whether and how their influence can be positive and negative [21]. As we start to encounter AI systems in various morally and legally salient environments, some have begun to explore how the current responsibility ascription practices might be adapted to meet such new technologies [19, 33]. A critical viewpoint today is that autonomous and self-learning AI systems pose a so-called responsibility gap [27]. These systems’ autonomy challenges human control over them [13], while their adaptability leads to unpredictability. Hence, it might infeasible to trace back responsibility to a specific entity if these systems cause any harm. Considering responsibility practices as the adoption of certain attitudes towards an agent [40], scholarly work has also posed the question of whether AI systems are appropriate subjects of such practices [15, 29, 37] — e.g., they might “have a body to kick,” yet they “have no soul to damn” [4]. -

An Invitation to Qualitative Research
CHAPTER 1 An Invitation to Qualitative Research n recent years, binge drinking has caused considerable concern among admin - istrators at colleges and universities, compelled by statistics that show marked Iincreases in such behavior. A qualitative researcher studying this topic would seek to go behind the statistics to understand the issue. Recently, we attended a fac - ulty meeting that addressed the problem of binge drinking and heard concerned faculty and administrators suggest some of the following solutions: • stricter campus policies with enforced consequences • more faculty-student socials with alcohol for those over 21 years old • more bus trips into the city to local sites such as major museums to get students interested in other pastimes Although well-intentioned, these folks were grasping at straws. This is because although they were armed with statistics indicating binge drinking was prevalent and thus could identify a problem, they had no information about why this trend was occurring. Without understanding this issue on a meaningful level, it is diffi - cult to remedy. At this point, we invite you to spend 5 to 10 minutes jotting down a list of questions you think are important to investigate as we try to better under - stand the phenomenon of binge drinking at college. What Is Qualitative Research? The qualitative approach to research is a unique grounding—the position from which to conduct research—that fosters particular ways of asking questions and particular ways of thinking through problems. As noted in the opening dis - cussion of binge drinking in college, the questions asked in this type of research usually begin with words like how, why, or what. -

CH 01 Study Guide
Okami Study Guide: Chapter 1 1 Chapter in Review 1. Psychology is the scientific study of mental processes and events (mind) and any potentially observable or measureable activity of a living organism (behavior). Psychological science uses methods grounded in modern scientific knowledge to conduct research in order to advance psychological knowledge. Variable topics and points of view characterize psychology. 2. Although people have always been interested in questions of mental life and the connection between mind and behavior, psychology as a concept did not exist in the ancient world. Early attempts to treat psychological questions include the teachings of Buddha, Aristotle, Chinese philosophers such as Confucius and Lao- tze, and Renaissance philosophers such as René Decartes (dualism) and John Locke (British empiricism). 3. Scientific psychology was born during the late 19th century as a union between philosophy and biology. Some important early schools of scientific psychology include structuralism (Titchener), functionalism (James), psychoanalysis (Freud), behaviorism (Watson, Skinner), and humanism (Rogers, Maslow). 4. Psychology today is distinguished by employment setting (university, hospital, business, clinic) and focus (research or application of research to solving real- world problems); by the psychologist’s field of study (e.g., developmental psychology, clinical psychology, cognitive psychology, etc.); and by the psychologist’s perspective, or point of view. Contemporary perspectives include cognitive, biobehavioral, psychodynamic, evolutionary, sociocultural, and positive psychology. 5. Science is an empirical method of gaining knowledge of the natural world. It is not the only empirical method of gaining this knowledge, but it is the best one. This is because science is less prone to bias than other methods, has built-in methods to change errors in thinking, and constantly refines knowledge gained in the past. -

Phenomenology: a Philosophy and Method of Inquiry
Journal of Education and Educational Developement Discussion Phenomenology: A Philosophy and Method of Inquiry Sadruddin Bahadur Qutoshi Karakorum International University, Pakistan [email protected] Abstract Phenomenology as a philosophy and a method of inquiry is not limited to an approach to knowing, it is rather an intellectual engagement in interpretations and meaning making that is used to understand the lived world of human beings at a conscious level. Historically, Husserl’ (1913/1962) perspective of phenomenology is a science of understanding human beings at a deeper level by gazing at the phenomenon. However, Heideggerian view of interpretive-hermeneutic phenomenology gives wider meaning to the lived experiences under study. Using this approach, a researcher uses bracketing as a taken for granted assumption in describing the natural way of appearance of phenomena to gain insights into lived experiences and interpret for meaning making. The data collection and analysis takes place side by side to illumine the specific experience to identify the phenomena that is perceived by the actors in a particular situation. The outcomes of a phenomenological study broadens the mind, improves the ways of thinking to see a phenomenon, and it enables to see ahead and define researchers’ posture through intentional study of lived experiences. However, the subjectivity and personal knowledge in perceiving and interpreting it from the research participant’s point of view has been central in phenomenological studies. To achieve such an objective, phenomenology could be used extensively in social sciences. Keywords: descriptive nature, interpretative nature, method of inquiry, phenomenology, philosophy Introduction Phenomenology as a philosophy provides a theoretical guideline to researchers to understand phenomena at the level of subjective reality. -

Qualitative Methodologies: Ethnography, Phenomenology, Grounded Theory and More
Page - 1 Qualitative methodologies: ethnography, phenomenology, grounded theory and more Have a look at my web page and follow the links to the teaching resources http://www.brown.uk.com I live in room 0.20b in the Hawthorn Building xtn 8755 or on [email protected] Aim of session: • To introduce some of the applications of qualitative methodologies to research questions the philosophical basis that underlies the qualitative methodology such as ethnography, phenomenology and grounded theory • To advance knowledge of key approaches to qualitative or descriptive research Learning Outcomes: By end of session students should be able to: • Be better equipped to make discerning choices about the appropriate methodology and analytic approach to their topic of enquiry. • Appreciate the contribution of these kinds of description to our knowledge of the social world Qualitative methods There are a great many of these, so I shall have to be selective. I’m sure you’ll find more, but some of my favourites are: Ethnography ‘The ethnographer participates overtly or covertly in people’s daily lives for extended periods of time watching what happens, listening to what is said, asking questions. In fact collecting whatever data are available to throw light on issues with which he or she is concerned’ (Hammersly & Atkinson 1983, p.2). ‘The social research style that emphasises encountering alien worlds and making sense of them is called ethnography or ‘folk description’. Ethnographers set out to show how social action in one world makes sense from the point of view of another’ (Agar 1986, p.12). How did it start? Various traces can be found within the history of ethnography and qualitative methodology: 1) Henry Mayhew – ‘London Labour and the London Poor’ – massive ethnographic study of low paid, unemployed, homeless etc. -

Madhu Guest Faculty, Department of Library & Information Science Patna
Madhu Guest Faculty, Department of Library & Information Science Patna University. Email Id – [email protected] Phone No. - 9308765287 MLIS Semester II (Paper – 1) Research Methods And Statistical Techniques Topic – Descriptive Method e-content Descriptive method Descriptive research is defined as a research method that describes the characteristics of the population or phenomenon that is being studied. This methodology focuses more on the “what” of the research subject rather than the “why” of the research subject. In other words, it is a type of research that describes a population, situation, or phenomenon that is being studied. It focuses on answering the how, what, when, and where questions. If a research problem, rather than the why. This is mainly because it is important to have a proper understanding of what a research problem is about before investigating why it exists in the first place. Characteristics Quantitative research: Descriptive research is a quantitative research method that attempts to collect quantifiable information to be used for statistical analysis of the population sample. It is an popular market research tool that allows to collect and describe the nature of the demographic segment. Uncontrolled variables: In descriptive research, none of the variables are influenced in any way. This uses observational methods to conduct the research. Hence, the nature of the variables or their behaviour is not in the hands of the researcher. Cross-sectional studies: Descriptive research is generally a Cross-sectional study where different sections belonging to the same group are studied and properly describe the research problem. Basis for further research: The data collected and analyzed from descriptive research can then be further researched using different research techniques. -

Definitions and Types of Research Articles
Definitions and Types of Research Articles Maidelina Nazario-Romero, Veteran Spouse Network Research Fellow June 21, 2016 Research studies are designed to find answers to a specific question or topics under investigation. Professionals across different settings conduct research to investigate topics relating to their field of study, increase knowledge to support evidence-based practices, test new hypotheses or to further understanding of existing theories. Researchers use different methods to conduct their investigations. Ideally, all research questions should be addressed using the scientific method to avoid inaccurate information; however, that it is not always the case. Some researchers seek to find answers through non- scientific approaches, which are often based on experts’ knowledge, instincts, beliefs, and professional reputation. In order to understand and evaluate the quality of research studies and apply findings effectively, it is necessary to become familiar with the characteristics that differentiate scientific research studies from nonscientific approaches. Methods of Acquiring knowledge Non-scientific Methods § Tenacity: Basing arguments on beliefs that have long been accepted as facts. § Intuition: Relying on one’s instincts to find answers. § Authority: Seeking answers from authority or experts on a specific subject. § Rationalism: Combining facts or assumptions with logical reasoning to find answers. § Empiricism: Relying on direct observations or personal experience. Scientific Method The scientific method uses empirical observation to develop hypotheses; then, researchers use hypotheses to generate predictions that can be empirically tested. Scientific methods are empirical, public, objective, and are based on previous theories. The main steps of the scientific method include: § Make observation of behaviors or other phenomena. § Construct a hypothesis (hypotheses must be testable and refutable). -

Quantitative Research Methods Distribute Student Learning Objectives Or
7 Quantitative Research Methods distribute Student Learning Objectives or After studying Chapter 7, students will be able to do the following: 1. Describe the defining characteristics of quantitative research studies 2. List and describe the basic steps in conducting quantitative research studies 3. Identify and differentiate among variouspost, approaches to conducting quantitative research studies 4. List and describe the steps and procedures in conducting survey, correlational, causal-comparative, quasi-experimental, experimental, and single-subject research 5. Identify and discusscopy, the strengths and limitations of various approaches to conducting quantitative research 6. Identify and explain possible threats to both internal and external validity 7. Design quantitativenot research studies for a topic of interest Do his chapter focuses on research designs commonly used when conducting quantitative research studies. The general purpose of quantitative research is to T investigate a particular topic or activity through the measurement of variables in quantifiable terms. Quantitative approaches to conducting educational research differ in numerous ways from the qualitative methods we discussed in Chapter 6. You will learn about these characteristics, the quantitative research process, and the specifics of several different approaches to conducting quantitative research. Copyright ©2016 by SAGE Publications, Inc. This work may not be reproduced or distributed in any form or by any means without express written permission of the publisher. 108 Part II • Designing A Research Study Characteristics of Quantitative Research Quantitative research relies on the collection and analysis of numerical data to describe, explain, predict, or control variables and phenomena of interest (Gay, Mills, & Airasian, 2009). One of the underlying tenets of quantitative research is a philosophical belief that our world is relatively stable and uniform, such that we can measure and understand it as well as make broad generalizations about it. -

Philosophy Henri Lefebvre
l\'11� philosophy T /-\ Henri Lefebvre Edited with an introduction by Stuart Elden METAPHILOSOPHY HENRI LEFEBVRE TRANSLATED BY DAVID FERNBACH EDITED WITH AN INTRODUCTION BY STUART ELDEN Y VERSO London • New York Cet ouvrage publie dans le cadre du programme d'aide a la publication beneficiedu soutien du Ministrere des Affaires Etrangereset du Service Culturel de l'Ambassade de France represente aux Etats-Unis. This work received support from the French Ministry of Foreign Affairs and the Cultural Services of the French Embassy in the United States through their publishing assistance programme. This English-language edition published by Verso 2016 Originally published in French as Metaphilosophie © Editions Syllepse 2000 Translation© David Fernbach 2016 Introduction© Stuart Elden 2016 All rights reserved The moral rights of the authors have been asserted 1 3 57 9 10 8 6 4 2 Verso UK: 6 Meard Street, London W 1F oEG US: 20 Jay Street, Suite 1010, Brooklyn, NY 11201 versobooks.com Verso is the imprint of New Left Books ISBN-13: 978-1-78478-274-0 (PBK) ISBN-13: 978-1-78478-273-3 (HBK) ISBN-13: 978-1-78478-276-4 (UK EBK) ISBN-13: 978-1-78478-275-7 (US EBK) British Library Cataloguing in Publication Data A catalogue record fo r this book is available from the British Library Library of Congress Cataloging-in-Publication Data A catalog record fo r this book is available from the Library of Congress Typset in Minion by Hewer Text UK, Ltd, Edinburgh Printed in the US by Maple Press Contents Introduction: A Study of Productive Tensions by Stuart Elden vii 1. -

Philosophical Rationalisation of a Geotechnical Narrative to Cost Overruns in Highway Projects
Review Article Civil Eng Res J Volume 10 Issue 3 - July 2020 Copyright © All rights are reserved by Alolote Amadi I DOI: 10.19080/CERJ.2020.10.555786 Philosophical Rationalisation of a Geotechnical Narrative to Cost Overruns in Highway Projects Alolote Amadi I* Department of Quantity Surveying, Rivers State University, Port Harcourt Submission: April 27, 2020; Published: July 28, 2020 *Corresponding author: Alolote Amadi I, Department of Quantity Surveying, Rivers State University, Port Harcourt Abstract Different methodological routes to the study of cost overruns are evident in the literature. A critical review reveals several gaps, particularly in highway projects. This study evaluates and select an adequate philosophical/methodological orientation relevant to provide a geotechnical narrativethe lack of to methodologically the phenomena robustof cost explanatoryoverruns in evidencehighway toprojects. support This the paperassertions thus thatsets geotechnicalout the underlying risks significantly philosophical impact and logicalon cost reasoning overruns that served as a guide on the conduct of a study, carried out to illuminate geotechnical trajectories to cost overruns in highway projects. Critical evaluation of the different philosophical stances evident in the literature was carried out, while factoring in the practicality and compatibility of the methods implicit in the various research strategies. The study adopted the philosophical stance of the critical realist, via the amalgamation of ontological positivism, with epistemological constructivism, in acknowledging the role that values and societal ideology play in the derivation of a geotechnical narrative to cost overruns, in view of its: wholesomeness in investigating the study phenomena; ability to incorporate requisite multipleempirical data knowledge sources on and cost research overruns. -
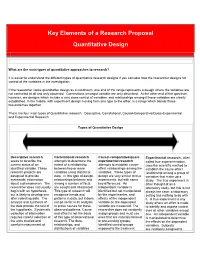
Key Elements of a Research Proposal Quantitative Design
Key Elements of a Research Proposal Quantitative Design What are the main types of quantitative approaches to research? It is easier to understand the different types of quantitative research designs if you consider how the researcher designs for control of the variables in the investigation. If the researcher views quantitative design as a continuum, one end of the range represents a design where the variables are not controlled at all and only observed. Connections amongst variable are only described. At the other end of the spectrum, however, are designs which include a very close control of variables, and relationships amongst those variables are clearly established. In the middle, with experiment design moving from one type to the other, is a range which blends those two extremes together. There are four main types of Quantitative research: Descriptive, Correlational, Causal-Comparative/Quasi-Experimental, and Experimental Research. Types of Quantitative Design Descriptive research Correlational research Causal-comparative/quasi- Experimental research, often seeks to describe the attempts to determine the experimental research called true experimentation, current status of an extent of a relationship attempts to establish cause- uses the scientific method to identified variable. These between two or more effect relationships among the establish the cause-effect research projects are variables using statistical variables. These types of relationship among a group of designed to provide data. In this type of design, design are very similar to true variables that make up a systematic information relationships between and experiments, but with some study. The true experiment is about a phenomenon. The among a number of facts key differences. -

Online Journalism: Research Methods
ONLINE JOURNALISM: RESEARCH METHODS Marcos Palacios Javier Díaz Noci (eds.) ONLINE JOURNALISM: RESEARCH METHODS A multidisciplinary approach in comparative perspective Contents INTRODUCTION 11 1. TYPOLOGY OF ONLINE MEDIA 15 1.1. Introduction 15 1.2.Relevance of the Typologies 17 1.3. Proposal for a Cybermedia Typology 19 1.3.1. Typologies Centred on the Actions or Development of the 19 Cybermedia 1.3.2. Typologies Centred on Communication Models 21 1.3.3. Typologies Centred on the Elements that Make Up the 23 Cybermedia 1.3.4. Typologies Centred on the Aim of the Cybermedia 23 2. GENRES IN ONLINE JOURNALISM: A TYPOLOGICAL PROPOSAL 25 2.1. Criteria for the Classific ation of Journalistic Genres 25 2.2. Theoretical and Methodological Framework of Research in Genres on 27 2.3. Analytical Proposal 30 2.3.1. Rhetorical Criteria 30 2.3.2. Hypertextuality 31 2.3.3. Multimediality 32 2.3.4. Interactivity and Participation 34 2.3.5. Temporality 35 2.4. Infographics 36 3. NEWS AND DATABASE ARCHITECTURE 39 3.1. Search methodologies for news architecture 39 3.1.1. Theoretical Context and State of the Question 39 3.1.2. Structure in the Cybermedia 42 3.1.3. Analysis of the Hierarchy of Elements 43 3.1.4. Applied Model for a Case Study 44 3.2. Methodologies of Database Analysis in Online Journalism 46 3.2.1. Theoretical Context and State of the Question 46 3.2.2. Databases as Paradigm and Metaphor 49 3.2.3. From the Syntactic Web to the Semantic Web 50 3.2.4.