Hidden Hunger World Review of Nutrition and Dietetics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report on the Implementation of the 2030 Agenda for Sustainable Development
Report on the implementation of the 2030 Agenda for sustainable development German Voluntary National Review to the HLPF 2021 1 German Voluntary National Review to the HLPF 2021 All states are called upon to take swifter and more ambitious action to implement the Agenda. With the update to the German Sustainable Development Strategy [adopted in March 2021], the German Government therefore aims to pick up the pace on the path to greater sustainability, both at home and in international cooperation. [...] If we are to achieve the goals of the German Sustainable Development Strategy and the 2030 Agenda for Sustainable Development, we must embark on a truly demanding transformation of key areas such as energy, the circular economy, housing, transport, food and agriculture. In Germany we plan to advance the transformation process by updating our German Sustainable Development Strategy and by harnessing education, research and innovation. (Federal Chancellor Dr. Angela Merkel in her foreword to the updated German Sustainable Development Strategy) German Voluntary National Review to the HLPF 2021 3 4 Content 1. Key messages 7 1.1 The twofold challenge: Pandemic response and the transition to sustainable development for a better and green recovery 8 1.2 Main areas of transition, unhalted by the pandemic response, within the leitmotifs of the 2030 Agenda: People, planet, prosperity, peace and partnership 9 1.3 Joint action; global responsibility; peace and security 14 2. Institutional and procedural aspects 17 3. Important changes 23 4. Pursuit -
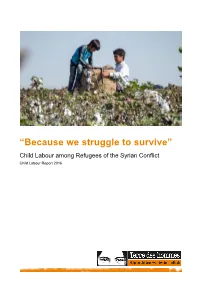
'Because We Struggle to Survive'
“Because we struggle to survive” Child Labour among Refugees of the Syrian Conflict Child Labour Report 2016 Disclaimer terre des hommes Siège | Hauptsitz | Sede | Headquarters Avenue de Montchoisi 15, CH-1006 Lausanne T +41 58 611 06 66, F +41 58 611 06 77 E-mail : [email protected], CCP : 10-11504-8 Research support: Ornella Barros, Dr. Beate Scherrer, Angela Großmann Authors: Barbara Küppers, Antje Ruhmann Photos : Front cover, S. 13, 37: Servet Dilber S. 3, 8, 12, 21, 22, 24, 27, 47: Ollivier Girard S. 3: Terre des Hommes International Federation S. 3: Christel Kovermann S. 5, 15: Terre des Hommes Netherlands S. 7: Helmut Steinkeller S. 10, 30, 38, 40: Kerem Yucel S. 33: Terre des hommes Italy The study at hand is part of a series published by terre des hommes Germany annually on 12 June, the World Day against Child Labour. We would like to thank terre des hommes Germany for their excellent work, as well as Terre des hommes Italy and Terre des Hommes Netherlands for their contributions to the study. We would also like to thank our employees, especially in the Middle East and in Europe for their contributions to the study itself, as well as to the work of editing and translating it. Terre des hommes (Lausanne) is a member of the Terre des Hommes International Federation (TDHIF) that brings together partner organisations in Switzerland and in other countries. TDHIF repesents its members at an international and European level. First published by terre des hommes Germany in English and German, June 2016. -

General 27 July 2010 English
United Nations E/C.12/DEU/5* Economic and Social Council Distr.: General 27 July 2010 English Original: French Committee on Economic, Social and Cultural rights Implementation of the Covenant on Economic, Social and Cultural Rights Fifth periodic report submitted by States parties under articles 16 and 17 of the Covenant Germany ** *** [16 September 2008] * Re-issued for technical reasons. ** In accordance with the information given to States Parties on the preparation of their reports, this document has not been reviewed by the Editing Section before transmission to the translation services of the United Nations. *** The annexes may be consulted at the secretariat. GE.10-46278 (EXT) E/C.12/DEU/5* Contents Paragraphs Page I. Introduction............................................................................................................... 1-2 3 II. Application of the Covenant in German domestic law ............................................ 3-42 3 III. Developments affecting the individual rights guaranteed by the Covenant ............ 43-368 10 A. General provisions of the Covenant................................................................. 43-76 10 Article 1. [Right of peoples to self-determination]........................... 43 10 Article 2. [Non-discrimination in the exercise of rights].................. 44-72 10 Article 3. [Equality between men and women]................................. 73-76 15 B. Individual rights guaranteed by the provisions of the Covenant..................... 77-368 15 Article 6. [Right to work] .................................................................. 77-114 15 Article 7. [Right to just and favourable conditions of work]............ 115-135 22 Article 8. [Right to take part in trade union activities] ..................... 136-145 26 Article 9. [Right to social security] ................................................... 146-209 28 Article 10. [Right of families, mothers, children and young people to protection and assistance] ............................................. 210-241 39 Article 11. -

Poverty and Well-Being: Panel Evidence from Germany*
Poverty and Well-Being: * Panel Evidence from Germany ANDREW E. CLARK Paris School of Economics - CNRS [email protected] CONCHITA D’AMBROSIO Università di Milano-Bicocca, DIW Berlin and Econpubblica [email protected] SIMONE GHISLANDI Università Bocconi and Econpubblica [email protected] This version: March 2013 Abstract We consider the link between poverty and subjective well-being, and focus in particular on the role of time. We use panel data on 42,500 individuals living in Germany from 1992 to 2010 to uncover four empirical relationships. First, life satisfaction falls with both the incidence and intensity of contemporaneous poverty. There is no evidence of adaptation within a poverty spell: poverty starts bad and stays bad in terms of subjective well-being. Third, poverty scars: those who have been poor in the past report lower life satisfaction today, even when out of poverty. Last, the order of poverty spells matters: for a given number of poverty spells, satisfaction is lower when the spells are concatenated: poverty persistence reduces well-being. These effects differ by population subgroups. Keywords: Income, Poverty, Subjective well-being, SOEP. JEL Classification Codes: I31, D60. * We thank Markus Grabka, Peter Krause, Nico Pestel and seminar participants at IARIW (Boston), Duisburg-Essen, Keio, Manchester, Osaka and VID (Vienna) for many valuable suggestions. The German data used in this paper were made available by the German Socio-Economic Panel Study (SOEP) at the German Institute for Economic Research (DIW), Berlin: see Wagner et al. (2007). Neither the original collectors of the data nor the Archive bear any responsibility for the analyses or interpretations presented here. -

THE PERCEPTION of CHILD POVERTY AMONG CAMEROONIAN FAMILIES Children´S Capabilities in Cameroonian Households in Berlin
THE PERCEPTION OF CHILD POVERTY AMONG CAMEROONIAN FAMILIES Children´s Capabilities in Cameroonian households in Berlin Doctoral Thesis Submitted in fulfilment for the degree of Doctor Philosophiae (Dr. Phil.) At the Micro-sociology Institute of the Philosophical Faculty III, Humboldt University to Berlin / Germany By Diane Flora Brahms, born Nsong Supervisors: 1st: Mr Professor Doctor Hans Bertram 2nd: Mrs Professor Doctor sec. Karin Lohr President of the Humboldt University to Berlin: Mr Prof. Dr. Jan-Hendrick Olbertz (2012) Dean of the Philosophical faculty at the Humboldt University in Berlin: Mrs Prof. Dr. Julia von Blumenthal (2012) Berlin / Germany, October 2015 Date of the oral exam: October 16th 2015 ABSTRACT Why should the perception of child poverty in Cameroonian families in Germany be analysed? This is a question we had to deal with all through this research phase. Why does it matter to take time trying to understand how Cameroonian people perceive child poverty and how it can impacts the Capabilities of their children in the German setting? Although the concept of poverty may seem obvious, experiencing it is a different story because of the way people perceive it. An interesting point in Cameroonian families in Berlin is that the concept of child poverty does not exist in their cultural background based on their languages. This is because children are viewed as their wealth. This study is an investigation of the Cameroonian perception of child poverty in Berlin and the application of the Capability Approach on it. The aim is to find out according to this, the future life opportunities of children with Cameroonian background in Germany. -
Gender and Multidimensional Poverty in Nicaragua: an Individual-Based Approach
Munich Personal RePEc Archive Gender and Multidimensional Poverty in Nicaragua: An Individual-based Approach Espinoza-Delgado, Jose and Klasen, Stephan University of Goettingen, Germany 15 February 2018 Online at https://mpra.ub.uni-muenchen.de/85263/ MPRA Paper No. 85263, posted 17 Mar 2018 23:06 UTC Gender and Multidimensional Poverty in Nicaragua: An Individual-based Approach José Espinoza-Delgado & Stephan Klasen University of Goettingen, Germany Revised February 2018 Abstract Most existing multidimensional poverty measures use the household as the unit of analysis so that the multidimensional poverty condition of the household is equated with the multidimensional poverty condition of all its members. For this reason, household-based poverty measures ignore the intra-household inequalities and are gender-insensitive. Gender equality, however, is at the center of the sustainable development, as it has been emphasized by the Goal 5 of the SDGs: “Achieve gender equality and empower all women and girls” (UN, 2015, p. 14); therefore, individual-based measures are needed in order to track the progress in achieving this goal. Consequently, in this paper, we contribute to the literature on multidimensional poverty and gender inequality by proposing an individual-based multidimensional poverty measure for Nicaragua and estimate the gender differentials in the incidence, intensity, and inequality of multidimensional poverty. Overall, we find that in Nicaragua, the gender gaps in multidimensional poverty are lower than 5%, and poverty does not seem to be feminized. However, the inequality among the multi-dimensionally poor is clearly feminized, especially among adults, and women are living in very intense poverty when compared with men. -

Towards a Multidimensional Poverty Index for Germany
Oxford Poverty & Human Development Initiative (OPHI) Oxford Department of International Development Queen Elizabeth House (QEH), University of Oxford OPHI WORKING PAPER NO. 98 Towards a Multidimensional Poverty Index for Germany Nicolai Suppa* September 2015 Abstract This paper compiles a multidimensional poverty index for Germany. Drawing on the capability approach as conceptual framework, I apply the Alkire-Foster method using German data. I propose a comprehensive operationalization of a multidimensional poverty index for an advanced economy like Germany, including a justification for several dimensions. Income, however, is rejected as a dimension on both conceptual and empirical grounds. I document that insights obtained by the proposed multidimensional poverty index are consistent with earlier findings. Moreover, I exploit the decomposability of the Alkire-Foster measure for both a consistently detection of specific patterns in multidimensional poverty and the identification of driving factors behind its changes. Finally, the results suggest that using genuine multidimensional measures makes a difference. Neither a single indicator nor a dashboard seem capable of replacing a multidimensional poverty index. Moreover, I find multidimensional and income-poverty measures to disagree on who is poor. Keywords: multidimensional poverty, Alkire-Foster method, capability approach, SOEP. JEL classification: I3, I32, D63, H1. * TU Dortmund, Department of Economics, 44221 Dortmund, Germany, e-mail: [email protected], phone: +49 231 -

Parallel Report of the Alliance for Economic, Social and Cultural Rights in Germany (Wsk-Allianz)
PARALLEL REPORT OF THE ALLIANCE FOR ECONOMIC, SOCIAL AND CULTURAL RIGHTS IN GERMANY (WSK-ALLIANZ) complementing the 5th Report of the Federal Republic of Germany on the International Covenant on Economic, Social and Cultural Rights (ICESCR) 1 PARALLEL REPORT ON ECONOMIC, SOCIAL AND CULTURAL RIGHTS IMPRINT ORGANISATIONS CONTRIBUTING TO THE REPORT: Amnesty International, Sektion der Bundesrepublik Deutschland e.V. Ban Ying e.V. Behandlungszentrum für Folteropfer Berlin (bzfo) Berliner Rechtshilfefonds Jugendhilfe e.V. (BRJ) BPE - Bundesverband Psychiatrie-Erfahrener e.V. Bund demokratischer WissenschaftlerInnen (BdWi) Diakonisches Werk der EKD FIAN Deutschland e.V. Forum Menschenrechte Frauenhauskoordinierung e.V. Gesellschaft zum Schutz von Bürgerrecht und Menschenwürde (GBM) Gewerkschaft Erziehung und Wissenschaft (GEW) GEW Landesverband Bayern Humanistische Union e.V. Intersexuelle Menschen e.V. IPPNW, Deutsche Sektion der Internationalen Ärzte für die Verhütung des Atomkrieges / Ärzte in sozialer Verantwortung e.V. KOK e.V. (Bundesweiter Koordinierungskreis gegen Frauenhandel und Gewalt an Frauen im Migrationsprozess) Lesben- und Schwulenverband in Deutschland (LSVD) e.V. Unter Druck – Kultur von der Straße e.V. Zentrum für Postgraduale Studien Sozialer Arbeit e.V. Berlin (ZPSA) GROUP OF COORDINATORS: Sibylle Gurzeler, ZPSA e.V. Ute Hausmann, FIAN Deutschland e.V. Ingo Stamm, Diakonisches Werk der EKD Frank Uhe, IPPNW Michael Windfuhr, Brot für die Welt (until Dec. 31, 2010) KONTAKT [email protected] www.wsk-allianz.de TRANSLATION German into English by: Ekpenyong Ani LAYOUT: Anne Tritschler PREFACE The Alliance for Economic, Social and Cultural Rights in Germany (in German: WSK-Allianz) is an ad-hoc network with 20 member organization (NGOs) from various fields of work. The Alliance is mainly based in Berlin und began its work in fall 2008, according to a initiative by the German Institute for Human Rights. -

Report of the German Federal Government to the High-Level Political Forum on Sustainable Development 2016
12 July 2016 Report of the German Federal Government to the High-Level Political Forum on Sustainable Development 2016 INDEX INTRODUCTION …………………………………………………………………………………………… p. 2 FULL REPORT ………………………………………………………………………………………………… p. 5 1. Our starting point: general information on Germany’s national context … p. 6 1a) The status quo in Germany …………………………………………………………………………… p. 6 1b) The existing National Sustainable Development Strategy ………………………………… p. 6 1c) Dialogue with civil society groups …………………………………………………………………… p. 8 1d) Ongoing support for other countries ……………………………………………………………… p. 10 2. Details on how this report was produced: process, participation, methodology, structure …………………………………………… p. 11 2a) Focus of the report ……………………………………………………………………………………… p. 12 2b) The involvement of state and non-governmental actors …………………………………… p. 12 3. What the SDGs are changing in Germany: steps and contributions towards implementation ……………………………………………………………………………… p. 12 3a) Integrating the Agenda and its SDGs into national implementation ..................... p. 12 3-a- aa) Measures with impacts in Germany ………………………………………………………… p. 13 3-a-bb) Germany’s engagement for the global level ……………………………………………… p. 14 3-a-cc) International cooperation for sustainable development ……………………………… p. 15 3b) Multi-stakeholder approach …………………………………………………………………………… p. 16 3c) Cross-cutting issue and 2016 thematic focus area – leave no one behind ………… p. 18 4. Report on the goals and associated targets ……………………………………………… p. 19 5. Next steps ………………………………………………………………………………………………… p. 59 1 INTRODUCTION The globalised world we live in is characterised by numerous and complex interdependencies. These are times of great challenges, and overcoming them will determine the future of humankind and the planet. But we are also living in a world of new and diverse opportuni- ties. The adoption of Transforming our World: The 2030 Agenda for Sustainable De- velopment was a milestone in the recent history of the United Nations. -
Did the Pattern of Poverty in West Germany Change Because of the Reunification?
Did the pattern of poverty in West Germany change because of the reunification? A cross-sectional study of poverty in West Germany Authors: Claire Collet and Kimberlay Duquennoy Supervisor: Magnus Carlsson Examiner: Dominique Anxo Term: VT19 Subject: Economics Level: Bachelor Course code: 2NA12E Abstract The reunification of West Germany and East Germany occurred in 1990 and had a great impact on the country. This essay investigates the impact that reunification had on the poverty structure of West Germany on the long-run. The results indicate that reunification had a negative impact on poverty since it increased the poverty rate by 4.88 percentage point in 2000 and by 6.16 percentage point in 2005. The structure of the poor population slightly changed the year following the reunification. Five years later, the structure of the poor population was similar to what it was before the reunification. However, during this period, the income transfer became more efficient since it decreased poverty by 6 percentage point to 16 percentage point more after reunification than it used to do before. Key words Poverty rate, poverty structure, West Germany, reunification, transfer income, difference-in-differences, linear probability regression. Acknowledgments Our gratitude is extended towards... ...Professor Dominique Anxo of Linnaeus University for the time given to us as well as the feedback given during the seminars. ...Professor Magnus Carlsson of Linnaeus University for his supervision and his help to structure our essay ...Discussant Estelle Ottou for constructive criticism about our essay. Contents 1 Introduction .................................................................................... 1 2 Literature review ............................................................................ 2 2.1 Poverty in East and West Germany after the reunification ..... -

“Germany Is Turning Its Back on the Fight Against Poverty and Social Exclusion”
“Germany is turning its back on the fight against poverty and social exclusion” Statement by the Nationale Armutskonferenz (nak) on the draft for a German National Reform Programme as part of the Europe 2020 strategy 31 May 2011 Author: Prof. Walter Hanesch, isasp - Institute for Social Work and Social Policy, Darmstadt University of Applied Sciences 1 Outline The European Year for Combating Poverty and Social Exclusion had not yet even come to an end when the German government abandoned the goal of effectively reducing and overcoming poverty and social exclusion in Germany. Thus – unnoticed by the German media – the government has relinquished a central social policy goal contained within the German social welfare model. At the same time, the policy on poverty has been trimmed back to its 1998 level. Until the late 1990s the various governments in the Federal Republic of Germany consistently denied the existence of poverty in the country and declared that a national policy against poverty was superfluous, given the presence of the safety net of social welfare benefits. In 1998, however, the newly formed SPD-Green coalition government put the topic of poverty on the national political agenda for the first time. It introduced a national poverty and wealth reporting system and adopted a programme to combat poverty and social exclusion. Around the same time, in 2000, the EU member states committed themselves to implementing a national policy to combat poverty and social exclusion when they introduced the Lisbon Strategy. Since then, as part of the open coordination to ensure the goal of cohesion, they have regularly introduced “national action plans for fighting against poverty and social exclusion” and, since 2006, “national strategy reports on social protection and social inclusion” where they report on their goals, programmes and successes. -

Annual Review 2001-2002
UNICEF INNOCENTI PUBLICATIONS ANNUAL REVIEW 2001-2002 UNICEF International Research Centre Piazza SS. Annunziata, 12 50122 Florence, Italy Tel.: +39 055 203 30 Fax: +39 055 244 817 E-mail (general information): [email protected] E-mail (publication orders): [email protected] Website: www.unicef-icdc.org ISBN: 88-85401-82-1 UNICEF INNOCENTI PUBLICATIONS ANNUAL REVIEW 2001-2002 i The UNICEF Innocenti Research Centre in Florence, Italy, was estab- lished in 1988 to strengthen the research capability of the United Nations Children’s Fund (UNICEF) and to support its advocacy for chil- dren worldwide. The Centre (formally known as the International Child Development Centre) helps to identify and research current and future areas of UNICEF’s work. Its prime objectives are to improve international understanding of issues relating to children’s rights and to help facilitate the full implementation of the United Nations Con- vention on the Rights of the Child in both industrialized and develop- ing countries. The Centre collaborates with its host institution in Florence, the Istituto degli Innocenti, in selected areas of work on child rights. Core funding for the Centre’s work is provided by the Government of Italy, while financial support for specific projects is also provided by other governments, international institutions and private sources, including UNICEF National Committees. This Annual Review provides a brief outline of the UNICEF Inno- centi Research Centre’s ongoing work, as well as work completed in 2001. For further details please consult the Centre’s website; www.unicef-icdc.org or contact Centre staff via email. UNICEF Innocenti Research Centre Piazza SS.