Review: Multiple Daily Doses of Antidepressants Are Not More Effective Than Single Daily Doses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

850 Physical Examination Or Selective Physical Examin Ation, and Special
850 CORRESPONDENCE mental state examination and, where indicated, a issue —¿wouldchanging to an SSRI be equally as physical examination or selective physical examin effective as adding one? One influential study (Nolen ation, and special investigations. This applies as eta!,1988)foundno benefitinchangingtofluvo much to people with Down's syndrome as it does to xamine for patients who were tricycic antidepressant the general population. non-responders, and is frequently cited to dismiss the We hope our papers help to establish that people strategy.However,a number ofotherauthorshave with Down's syndrome experience increased rates of found that a clinically significant proportion of tri certain psychiatric disorders, and that the pattern cyclic non-responders do respond to a subsequent of adaptive behaviour in these individuals changes SSRI given alone (Lingjaerde eta!, 1983; Delgado et with age. There is, of course, a distinction between al, 1988; Beasley et a!, 1990; White et a!, 1990). descriptive psychopathology by which a psychiatric Admittedly these have been open studies but I would diagnosis is made, and aetiological factors which argue that it is premature to dismiss changing to contribute to the described illness. Having estab another non-monoamine oxidase inhibitor anti lished different rates of psychiatric disorders, the depressant in favour of combination drug treatment next stage is to determine the relevant aetiological on current evidence. Further research is required factors. The view of Drs Prasher & Krishnan, that to determine the best ‘¿second-step'treatmentfor sensory impairment and medical illness account for patients failing to respond to an adequate trial of a the altered rates of psychiatric disorders, is specu tricyclic antidepressant drug. -

Inhibitory Action of Antidepressants on Mouse Betaine/GABA Transporter (BGT1) Heterologously Expressed in Cell Cultures
Int. J. Mol. Sci. 2012, 13, 2578-2589; doi:10.3390/ijms13032578 OPEN ACCESS International Journal of Molecular Sciences ISSN 1422-0067 www.mdpi.com/journal/ijms Article Inhibitory Action of Antidepressants on Mouse Betaine/GABA Transporter (BGT1) Heterologously Expressed in Cell Cultures Gerile 1, Chiharu Sogawa 1, Kazumi Ohyama 2, Takashi Masuko 3, Tadashi Kusama 3, Katsuya Morita 4, Norio Sogawa 1 and Shigeo Kitayama 1,* 1 Department of Dental Pharmacology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama 700-8525, Japan; E-Mails: [email protected] (G.); [email protected] (C.S.); [email protected] (N.S.) 2 RI Research Center, Okayama University Dental School, Okayama 700-8525, Japan; E-Mail: [email protected] 3 Laboratory of Physiology and Anatomy, College of Pharmacy, Nihon University, Funabashi 274-8555, Japan; E-Mails: [email protected] (T.M.); [email protected] (T.K.) 4 Department of Dental Pharmacology, Hiroshima University Graduate School of Biomedical Sciences, Hiroshima 734-8553, Japan; E-Mail: [email protected] * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel: +81-86-235-6660; Fax: +81-86-235-6664. Received: 29 December 2011; in revised form: 28 January 2012 / Accepted: 17 February 2012 / Published: 24 February 2012 Abstract: Betaine/γ-aminobutyric acid (GABA) transporter (BGT1, SLC6A12) is a member of the Na+- and Cl−-dependent neurotransmitter transporter gene family with a homology to the GABA transporters (GATs), GAT1 (SLC6A1), GAT2 (SLC6A13) and GAT3 (SLC6A11) (HUGO nomenclature). -

Serotonin Transporter Occupancy with Tcas and Ssris: a PET Study in Patients with Major Depressive Disorder
International Journal of Neuropsychopharmacology (2012), 15, 1167–1172. f CINP 2012 BRIEF REPORT doi:10.1017/S1461145711001945 Serotonin transporter occupancy with TCAs and SSRIs: a PET study in patients with major depressive disorder Johan Lundberg, Mikael Tiger, Mikael Lande´n, Christer Halldin and Lars Farde Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden Abstract The aim of the present clinical positron emission tomography study was to examine if the 5-HTT is a common target, both for tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). Serotonin transporter (5-HTT) occupancy was estimated during treatment with TCA, SSRI and mirtazapine in 20 patients in remission from depression. The patients were recruited from out-patient units and deemed as responders to antidepressive treatment. The radioligand [11C]MADAM was used to determine the 5-HTT binding potential. The mean 5-HTT occupancy was 67% (range 28–86%). There was no significant difference in 5-HTT occupancy between TCA (n=5) and SSRI (n=14). 5-HTT affinity correlated with the recommended clinical dose. Mirtazapine did not occupy the serotonin transporter. The results support that TCAs and SSRIs have a shared mechanism of action by inhibition of 5-HTT. Received 13 November 2011; Reviewed 7 December 2011; Accepted 7 December 2011; First published online 16 January 2012 Key words: 5-HTT, depression, PET, SSRI, TCA. Introduction Molecular imaging methods such as positron emission tomography (PET) allow for measurement of The era of pharmacological treatment of depression drug binding to target proteins in the human brain. began with the tricyclic antidepressant (TCA), Recent advancements include the development of the imipramine, which was found to be effective in the radioligand [11C]DASB, for selective imaging of 5-HTT treatment of endogenous depression (Kuhn, 1958). -

Serum Fluoxetine and Norfluoxetine Levels Support the Safety of Fluoxetine in Overdose Stephanie Pope* and Solomon G
Pope and Zaraa Ann Gen Psychiatry (2016) 15:30 DOI 10.1186/s12991-016-0117-z Annals of General Psychiatry CASE REPORT Open Access Serum fluoxetine and norfluoxetine levels support the safety of fluoxetine in overdose Stephanie Pope* and Solomon G. Zaraa Abstract Background: Previous literature has found fluoxetine to be relatively safe in overdose. This study hopes to examine this idea along with support from published pharmacokinetic information including serum fluoxetine and norfluox- etine levels based on information from a clinical case series. Methods: Four cases are presented along with vital abnormalities, electrocardiogram abnormalities, and physical exam abnormalities along with amount of overdose and resulting serum fluoxetine and norfluoxetine levels. Case Presentation: In these four cases, serum fluoxetine and norfluoxetine days after overdose were found to be in a range believed to be within the treatment range. No abnormalities were found on electrocardiogram but some patients (3) were found to have slight elevations in heart rate. Conclusion: Fluoxetine is relatively safe in overdose. This study supports previous literature. Future directives for research can be directed towards when serotonergic, including fluoxetine, medications can be introduced or restarted in patients who have overdosed. Research could also focus on if the introduction of another medication, such as carbamazepine, to induce metabolism of a medication, such as fluoxetine, after an overdose. Background adults in this study, the mean dose ingested was 544 mg, Previous research has provided ample evidence to con- while 30 were asymptomatic, 15 were found to have tach- clude fluoxetine without tricyclic antidepressants as ycardia, 14 reported drowsiness, five with tremor, four relatively safe in overdose. -

Selective Serotonin Reuptake Inhibitors Are Effective for Mixed Chronic Pain
Review: Selective serotonin reuptake inhibitors are effective for Evid Based Med: first published as 10.1136/ebm.1998.3.12 on 1 February 1998. Downloaded from mixed chronic pain Jung AC, Staiger T, Sullivan M. The myalgia; patient numbers; and clini- ever, in 2 other studies, patients efficacy of selective serotonin cal response. received paroxetine or citaioprarr reuptake inhibitors for the manage- improved pain reduction comparec ment of chronic pain, J Gen Intern Main results those who received placebo (P < Med. 1997Jun;12:384-9. 19 studies met die selection criteria. 10 and P = 0.02, respectively). 3 stud studies with 550 patients evaluated the 83 patients with fibromyalgia were t effectiveness of SSRIs in patients with 2 studies found no differences bet Objective chronic headache. In 3 separate studies, SSRIs (fluoxetine and citalopram To determine the effectiveness of se- improvement in chronic tension-type placebo for fibromyalgia, wher lective serotonin reuptake inhibitors headache was found with paroxetine study found improvement with fli (SSRIs) in the management of chronic (P < 0.05), fluoxetine (P = 0.029), and tine, especially when used with am pain. fluvoxamine (P < 0.05). However, in tyline. 3 studies of 119 patients 1 placebo-conn-oiled study, no improve- mixed chronic pain showed more Data sources ment was found with citalopram relief and improvement in intens Studies were identified by searching (P = 0.68). Studies on migraine head- patients who received zimelidine MEDLINE (1966 to 1997) using the ache had conflicting results. 1 study oxetine, or amitriptyline comparec keywords pain, neuropathy, migraine, found that fluoxetine improved head- placebo (P < 0.05). -

Neonatal Antidepressant Exposure Has Lasting Effects on Behavior and Serotonin Circuitry
Neuropsychopharmacology (2006) 31, 47–57 & 2006 Nature Publishing Group All rights reserved 0893-133X/06 $30.00 www.neuropsychopharmacology.org Neonatal Antidepressant Exposure has Lasting Effects on Behavior and Serotonin Circuitry Dorota Maciag1,4, Kimberly L Simpson2,4, David Coppinger3, Yuefeng Lu2, Yue Wang2, Rick CS Lin2 ,1,3 and Ian A Paul* 1Department of Psychiatry & Human Behavior, University of Mississippi Medical Center, Jackson, MS, USA; 2Department of Anatomy, University of Mississippi Medical Center, Jackson, MS, USA; 3Department of Pharmacology & Toxicology, University of Mississippi Medical Center, Jackson, MS, USA A significant fraction of infants born to mothers taking selective serotonin reuptake inhibitors (SSRIs) during late pregnancy display clear signs of antidepressant withdrawal indicating that these drugs can penetrate fetal brain in utero at biologically significant levels. Previous studies in rodents have demonstrated that early exposure to some antidepressants can result in persistent abnormalities in adult behavior and indices of monoaminergic activity. Here, we show that chronic neonatal (postnatal days 8–21) exposure to citalopram (5 mg/kg, twice daily, s.c.), a potent and highly selective SSRI, results in profound reductions in both the rate-limiting serotonin synthetic enzyme (tryptophan hydroxylase) in dorsal raphe and in serotonin transporter expression in cortex that persist into adulthood. Furthermore, neonatal exposure to citalopram produces selective changes in behavior in adult rats including increased locomotor activity and decreased sexual behavior similar to that previously reported for antidepressants that are nonselective monoamine transport inhibitors. These data indicate that the previously reported neurobehavioral effects of antidepressants are a consequence of their effects on the serotonin transporter. -
Neurotransmitters Mechanisms and Antidepressants
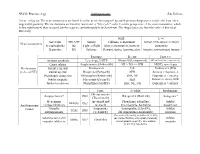
SP.236: Pharmacology Antidepressants Zak Fallows A note on layout: The neurotransmitters are listed from the most often targeted by antidepressant drugs (serotonin) to the least often targeted (dopamine). The mechanisms are listed in functional or “life cycle” order from the perspective of the neurotransmitter, which is first synthesized, then released, binds receptors, and ultimately is broken down. The drug classes are listed in order of historical discovery. High: Low: Serotonin SER, 5-HT Satiety Fullness, contentment Anxiety, OCD, aggression, hungry Neurotransmitters Norepinephrine NE Fight or flight Alert, concentration, memory Inattentive Dopamine DA Salience Reward, desire, learning, alert Inactive, unmotivated, hungry Example: Boosts: Used for: Increase synthesis Levodopa, 5-HTP DA and SER, respectively PD and useless, respectively Cause release Amphetamine (Adderall®) NE > DA >> SER ADHD, narcolepsy Mechanisms Receptor agonist Pramipexole DA Parkinson’s (PD) (to boost NT) Partial agonist Buspirone (BuSpar®) SER Anxiety > depression Presynaptic antagonist Mirtazapine (Remeron®) SER, NE Depression > anxiety Inhibit reuptake Fluoxetine (Prozac®) SER Depression, anxiety, OCD Inhibit breakdown Phenelzine (Nardil®) SER, NE, DA Depression > anxiety First: Notable: Mechanism: Chlorpromazine Antipsychotics* 1952 Haloperidol (Haldol®) Antagonist* (Thorazine®) Monoamine Iproniazid and Phenelzine, selegiline, Inhibit MAOIs 1953 Antidepressant oxidase inhibitors isoniazid moclobemide, harmaline breakdown Tricyclic Imipramine Amitriptyline (Elavil®), Inhibit classes TCAs 1955 antidepressants (Tofranil®) chlomipramine (Anafranil®) reuptake Fluoxetine (Prozac®), sertraline (Zoloft®), Selective serotonin paroxetine (Paxil®), citalopram (Celexa®), Inhibit SSRIs 1977 Zimelidine reuptake inhibitors escitalopram (Lexapro®), fluvoxamine reuptake (Luvox®), dapoxetine MIT OpenCourseWare http://ocw.mit.edu ES.S10 Drugs and the Brain Spring 2013 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms.. -

Trazodone Hydrochloride in the Treatment of Dysesthetic Pain in Traumatic Myelopathy: a Randomized, Double-Blind, Placebo-Controlled Study
Pain, 29 (1987) 151-161 151 Elsevier PA1 01026 Trazodone hydrochloride in the treatment of dysesthetic pain in traumatic myelopathy: a randomized, double-blind, placebo-controlled study Gary Davidoff * , Mary Guarracini * *, Elliot Roth * * * , James Sliwa * * * and Gary Yarkony * * * * Department of Physical Medicine and Rehabilitation, University of Michigan Medical Center, Ann Arbor, MI 48109 (U.S.A.), ** Helen Hayes Rehabilitation Hospital, West Haverstraw, NY 10993 (U.S.A.), and * * * Department of Rehabilitation Medicine, Northwestern University Medical School, Chicago, IL 60611 (U.S.A.) (Received 12 May 1986, revised received 9 September 1986, accepted 17 September 1986) SummarY Dysesthetic pain following traumatic myelopathy is characterized by diffuse burning and tingling sensations distal to the level of spinal injury. The dysesthetic pain syndrome (DPS) can compromise performance of functional abilities and inhibit participation in rehabilitation programs. Recent laboratory evidence suggests that antidepressant medications with selective inhibition of serotonin reuptake in the brain may be associated with superior analgesic effect compared to such non-selective agents as amitriptyline. Trazodone hydrochloride is a potent presynaptic serotonin reuptake blocker with few anticholinergic and cardiovascular side effects. This study was a randomized, double-blind, placebo- controlled trial of trazodone hydrochloride for the treatment of DPS. Following a 2-week placebo lead-in period, patients were randomized to a 6-week course of 150 mg trazodone hydrochloride/day or placebo. Evaluations of pain quality and intensity were performed at 2-week intervals, utilizing the McGill Pain Questionnaire, Stembach Pam Intensity Scale, and Zung Pam and Distress Index. Neurologic examina- tion and assessment of side effects were performed at each evaluation session. -

Antagonism of Nicotinic Acetylcholine Receptors by Inhibitors of Monoamine Uptake HE Lo´Pez-Valde´S and J Garcı´A-Colunga
Molecular Psychiatry (2001) 6, 511–519 2001 Nature Publishing Group All rights reserved 1359-4184/01 $15.00 www.nature.com/mp ORIGINAL RESEARCH ARTICLE Antagonism of nicotinic acetylcholine receptors by inhibitors of monoamine uptake HE Lo´pez-Valde´s and J Garcı´a-Colunga Centro de Neurobiologı´a, Universidad Nacional Auto´noma de Me´xico, Campus Juriquilla, Apartado Postal 1–1141, Juriquilla, Quere´taro 76001, Me´xico A study was made of the effects of several monoamine-uptake inhibitors on membrane cur- rents elicited by acetylcholine (ACh-currents) generated by rat neuronal ␣24 and mouse mus- cle nicotinic acetylcholine receptors (AChRs) expressed in Xenopus laevis oocytes. For the two types of receptors the monoamine-uptake inhibitors reduced the ACh-currents albeit to different degrees. The order of inhibitory potency was norfluoxetine Ͼ clomipramine Ͼ inda- traline Ͼ fluoxetine Ͼ imipramine Ͼ zimelidine Ͼ 6-nitro-quipazine Ͼ trazodone for neuronal ␣24 AChRs, and norfluoxetine Ͼ fluoxetine Ͼ imipramine Ͼ clomipramine Ͼ indatraline Ͼ zimelidine Ͼ trazodone Ͼ 6-nitro-quipazine for muscle AChRs. Thus, the most potent inhibitor was norfluoxetine, whilst the weakest ones were trazodone, 6-nitro-quipazine and zimelidine. Effects of the tricyclic antidepressant imipramine were studied in more detail. Imipramine inhibited reversibly and non-competitively the ACh-current with a similar inhibiting potency for both neuronal ␣24 and muscle AChRs. The half-inhibitory concentrations of imipramine were 3.65 ± 0.30 M for neuronal ␣24 and 5.57 ± 0.19 M for muscle receptors. The corre- sponding Hill coefficients were 0.73 and 1.2 respectively. -

Inhibition of G Protein-Activated Inwardly Rectifying K+ Channels By
Neuropsychopharmacology (2004) 29, 1841–1851 & 2004 Nature Publishing Group All rights reserved 0893-133X/04 $30.00 www.neuropsychopharmacology.org Inhibition of G Protein-Activated Inwardly Rectifying K þ Channels by Various Antidepressant Drugs Toru Kobayashi*,1, Kazuo Washiyama1 and Kazutaka Ikeda2 1 2 Department of Molecular Neuropathology, Brain Research Institute, Niigata, University, Niigata, Japan; Department of Molecular Psychiatry, Tokyo Institute of Psychiatry, Tokyo, Japan þ G protein-activated inwardly rectifying K channels (GIRK, also known as Kir3) are activated by various G protein-coupled receptors. GIRK channels play an important role in the inhibitory regulation of neuronal excitability in most brain regions and the heart rate. Modulation of GIRK channel activity may affect many brain functions. Here, we report the inhibitory effects of various antidepressants: imipramine, desipramine, amitriptyline, nortriptyline, clomipramine, maprotiline, and citalopram, on GIRK channels. In Xenopus oocytes injected with mRNAs for GIRK1/GIRK2, GIRK2 or GIRK1/GIRK4 subunits, the various antidepressants tested, except fluvoxamine, zimelidine, and bupropion, reversibly reduced inward currents through the basal GIRK activity at micromolar concentrations. The inhibitions were concentration-dependent with various degrees of potency and effectiveness, but voltage- and time-independent. In contrast, Kir1.1 and Kir2.1 channels in other Kir channel subfamilies were insensitive to all of the drugs. Furthermore, GIRK current responses activated by the cloned A1 adenosine receptor were similarly inhibited by the tricyclic antidepressant desipramine. The inhibitory effects of desipramine were not observed when desipramine was applied intracellularly, and were not affected by extracellular pH, which changed the proportion of the uncharged to protonated desipramine, suggesting its action from the extracellular side. -

Duloxetine Increases Serotonin and Norepinephrine Availability in Healthy Subjects: a Double-Blind, Controlled Study
Neuropsychopharmacology (2003) 28, 1685–1693 & 2003 Nature Publishing Group All rights reserved 0893-133X/03 $25.00 www.neuropsychopharmacology.org Duloxetine Increases Serotonin and Norepinephrine Availability in Healthy Subjects: A Double-Blind, Controlled Study ,1 1 1 2 2 Stephan A Chalon* , Luc-Andre´ Granier , Franc¸ois R Vandenhende , Peter R Bieck , Frank P Bymaster , Melissa J Joliat2, Christine Hirth3, William Z Potter2 1 2 3 Lilly Research Laboratories, Mont-Saint-Guibert, Belgium; Lilly Research Laboratories, Indianapolis, IN, USA; Universite´ Louis Pasteur, Strasbourg, France Evidence suggests that compounds that increase the synaptic availability of more than one neurotransmitter have greater efficacy in the treatment of depression than single-acting drugs. Preclinical studies indicate that duloxetine acts to inhibit serotonin (5-HT) and norepinephrine (NE) transporters. The ability of duloxetine to alter 5-HT and NE reuptake was tested in 12 healthy male subjects. Placebo, desipramine 50 mg b.i.d., and duloxetine (80 mg q.d. or 60 mg b.i.d.) were compared in a randomized, double-blind, three- period crossover study in 12 healthy male subjects. Whole-blood 5-HT, urinary excretion of NE and major metabolites, and TYR PD30 (IV tyramine pressor dose needed to increase systolic blood pressure by 30 mmHg) were measured at steady state. Vital signs were measured periodically. Duloxetine affected 5-HT reuptake, with whole-blood 5-HT depletion vs placebo (80 mg q.d.: p ¼ 0.07; 60 mg b.i.d.: p ¼ 0.02; combined regimens: p ¼ 0.01). Cardiovascular changes reflecting increased sympathetic tone were observed with both duloxetine and desipramine, and both treatments significantly decreased whole body NE turnover (po0.01). -
A Historical Note on the Development of Zimelidine, the First Selective
The historyof physicaltreatments in psychiatry 235s a methadone prescription dispensed from a community pharmacy. Methods: A consecutive series of 20 long-term opiate addicts regular counselling appointments with a community nurse and a currently enrolled in MMT was recruited from a closed ward. treatment objective of detoxification or a place in a methadone During the study period of four days. craving was assessed 10 maintenance programme where they attended daily to take their times per day using the experience sample methodology. On the methadone on the premises and had stable maintenance as the treat first day. psychopathology was measured with the 28 item General ment goal. Subjects who refused to accept their allocated treatment Health Questionnaire (GHQ-28) and the 90 item Symptom Check were offered the other condition. They were assessed at intake and List (SCl-90). During the second day 8-9 plasma samples were again I. 2, 3, 6. and 12 months after entering treatment. drawn and plasma methadone concentrations were determined using Results: 119 subjects entered the trial. 75 went to COT treatment. a newly developed high pressure liquid chromatography (HPlC) 47 randomised 28 chosen, and 44 to MMC treatment 33 randomised procedure. and II chosen. The COT group stayed in treatment for a mean of5.76 Results: A significant positive relationship was observed between months, the MMC group for 8.69 months. 91% of the whole sample oral methadone dose and craving (r = 0.55). No significant rela were contacted for follow up at 12 months. Data on the conduct of tions were found between craving and pharmacokinetic parameters the study will be presented.