Subcutaneous Administration of Biotherapeutics: an Overview of Current Challenges and Opportunities
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
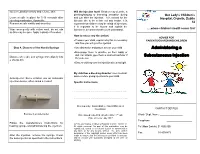
Administering a Subcutaneous Injection
Inject medication slowly and release skin Will the injection hurt? Children may describe a pinching/stinging or bee-sting sensation during Our Lady’s Children’s Leave needle in place for 5-10 seconds after and just after the injection. It is normal for the Hospital, Crumlin, Dublin injecting medication, if possible injection site to be a little red and tender. It is 12 Remove needle swiftly and smoothly expected that children may be afraid of injections. It is important to be honest and explain the Wipe area gently with cotton wool, do not rub injection in a manner that they can understand. ….where children’s health comes first as this may be sore. Apply a plaster if needed. How to reduce any discomfort: ADVICE FOR • Prepare your child, explain why this is necessary PARENTS/GUARDIANS/CHILDREN and how you will give the injection Step 4. Dispose of the Needle/Syringe • Use distraction and play to amuse your child Administering a • Encourage them to practice on their teddy or doll. For infants, give them a soother/comforter if Subcutaneous Injection Dispose of needle and syringe immediately into they use one a sharps bin • Ensure clothing over the injection site is not tight My child has a bleeding disorder: seek medical advice before giving injections to your child. Auto-injector: Some children use an automatic injection device, often called a ‘rocket’. Specific Instructions: ……………………………………………………………………… ………………………………………………………………………. Developed by: Naomi Bartley, Clinical Placement Coordinator. CONTACT DETAILS Example of an Auto-Injector st Date issued: July 2014, October 2012 : 1 edn. Ward / Dept. Name: _________________ Date of review: July 2017 Telephone: ___________________ Follow the manufacture’s instructions for ©2014, Our Lady’s Children’s Hospital Crumlin, Dublin 12. -

Fascia Iliaca Block in the Emergency Department for Hip Fracture
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Serveur académique lausannois Pasquier et al. BMC Geriatrics (2019) 19:180 https://doi.org/10.1186/s12877-019-1193-0 RESEARCH ARTICLE Open Access Fascia iliaca block in the emergency department for hip fracture: a randomized, controlled, double-blind trial Mathieu Pasquier1, Patrick Taffé2, Olivier Hugli1, Olivier Borens3, Kyle Robert Kirkham4 and Eric Albrecht5* Abstract Background: Hip fracture causes moderate to severe pain and while fascia iliaca block has been reported to provide analgesic benefit, most previous trials were unblinded, with subsequent high risks of performance, selection and detection biases. In this randomized, control double-blind trial, we tested the hypothesis that a fascia iliaca block provides effective analgesia for patients suffering from hip fracture. Methods: Thirty ASA I-III hip fracture patients over 70 years old, who received prehospital morphine, were randomized to receive either a fascia iliaca block using 30 ml of bupivacaine 0.5% with epinephrine 1:200,000 or a sham injection with normal saline. The fascia iliaca block was administered by emergency medicine physicians trained to perform an anatomic landmark-based technique. The primary outcome was the comparison between groups of the longitudinal pain score profiles at rest over the first 45 min following the procedure (numeric rating scale, 0–10). Secondary outcomes included the longitudinal pain score profiles on movement and the comparison over 4 h, 8 h, 12 h, and 24 h after the procedure, along with cumulative intravenous morphine consumption at 24 h. Results: At baseline, the fascia iliaca group had a lower mean pain score than the sham injection group, both at rest (difference = − 0.9, 95%CI [− 2.4, 0.5]) and on movement (difference = − 0.9, 95%CI [− 2.7; 0.9]). -
Technical Considerations for Pen, Jet, and Related Injectors Intended for Use with Drugs and Biological Products
Guidance for Industry and FDA Staff: Technical Considerations for Pen, Jet, and Related Injectors Intended for Use with Drugs and Biological Products Additional copies are available from: Office of Combination Products Office of Special Medical Programs Office of the Commissioner Food and Drug Administration 10903 New Hampshire Avenue, WO-32 Hub 5129 Silver Spring, MD 20993 (Tel) 301-796-8930 (Fax) 301-796-8619 http://www.fda.gov/CombinationProducts/default.htm This document finalizes the draft guidance issued in April 2009. For questions regarding this document, contact the Office of Combination Products at [email protected] or Patricia Y. Love, MD at 301-796-8933 or [email protected] U.S. Department of Health and Human Services Food and Drug Administration Center for Devices and Radiological Health, Center for Drug Evaluation Research, Center for Biologics Evaluation and Research, and Office of Combination Products in the Office of the Commissioner June 2013 Contains Nonbinding Recommendations Table of Contents INTRODUCTION.....................................................................................................................3 BACKGROUND .......................................................................................................................4 SECTION I: SCIENTIFIC AND TECHNICAL CONSIDERATIONS.............................5 A. INJECTOR DESCRIPTION .............................................................................................5 B. DESIGN FEATURES.........................................................................................................9 -

Changes in Serum Micrornas After Anti-IL-5 Biological Treatment of Severe Asthma
International Journal of Molecular Sciences Article Changes in Serum MicroRNAs after Anti-IL-5 Biological Treatment of Severe Asthma Manuel J. Rial 1,2, José A. Cañas 2,3 , José M. Rodrigo-Muñoz 2,3 , Marcela Valverde-Monge 1 , Beatriz Sastre 2,3 , Joaquín Sastre 1,3 and Victoria del Pozo 2,3,* 1 Allergy Unit, Hospital Universitario Fundación Jiménez Díaz, 28040 Madrid, Spain; [email protected] (M.J.R.); [email protected] (M.V.-M.); [email protected] (J.S.) 2 Department of Immunology, IIS-Fundación Jiménez Díaz, 28040 Madrid, Spain; [email protected] (J.A.C.); [email protected] (J.M.R.-M.); [email protected] (B.S.) 3 CIBER de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, 28029 Madrid, Spain * Correspondence: [email protected]; Tel.: +34-9155-048-91 Abstract: There is currently enough evidence to think that miRNAs play a role in several key points in asthma, including diagnosis, severity of the disease, and response to treatment. Cells release different types of lipid double-membrane vesicles into the extracellular microenvironment, including exosomes, which function as very important elements in intercellular communication. They are capable of distributing genetic material, mRNA, mitochondrial DNA, and microRNAs (miRNAs). Serum miRNA screening was performed in order to analyze possible changes in serum miRNAs in 10 patients treated with reslizumab and 6 patients with mepolizumab after 8 weeks of treatment. The expression of miR-338-3p was altered after treatment (p < 0.05), although no significant differences between reslizumab and mepolizumab were found. Bioinformatic analysis showed that miR-338-3p regulates important pathways in asthma, such as the MAPK and TGF-β signaling pathways and the Citation: Rial, M.J.; Cañas, J.A.; biosynthesis/degradation of glucans (p < 0.05). -

MEP-AST Mepolizumab Versus Placebo for Asthma
MEP-AST Mepolizumab versus placebo for asthma Mepolizumab versus placebo for asthma Review information Review type: Intervention Review number: MEP-AST Authors Colin Powell1, Stephen J Milan2, Kerry Dwan3, Lynne Bax4, Nicola Walters5 1Department of Child Health, Institute of Molecular and Experimental Medicine, Cardiff University School of Medicine, Cardiff, UK 2Lancaster Health Hub, Lancaster University, Lancaster, UK 3Department of Biostatistics, University of Liverpool, Liverpool, UK 4Lancashire Care NHS Foundation Trust, Preston, UK 5Chest Unit, St George's University Hospitals NHS Foundation Trust, London, UK Citation example: Powell C, Milan SJ, Dwan K, Bax L, Walters N. Mepolizumab versus placebo for asthma. Cochrane Database of Systematic Reviews 2015 , Issue 7 . Art. No.: CD010834. DOI: 10.1002/14651858.CD010834.pub2 . Contact person Colin Powell Senior Lecturer Department of Child Health Institute of Molecular and Experimental Medicine, Cardiff University School of Medicine Cardiff UK E-mail: [email protected] Dates Assessed as Up-to-date:19 November 2014 Date of Search: 19 November 2014 Next Stage Expected: 6 June 2017 Protocol First Published:Issue 11 , 2013 Review First Published: Issue 7 , 2015 Last Citation Issue: Issue 7 , 2015 What's new Date Event Description History Date Event Description Abstract Background Mepolizumab is a human monoclonal antibody against interleukin-5 (IL-5), the main cytokine involved in the activation of eosinophils, which in turn causes airway inflammation. Recent studies have suggested these agents may have a role in reducing exacerbations and improving health-related quality of life (HRQoL). There are no recommendations for the use of mepolizumab in adults or children in the recent update of the BTS/SIGN guidelines (BTS/SIGN 2014). -

Refi Ning Procedures for the Administration of Substances
WORKINGPARTY REPORT Rening procedures for theadministration of substances Report of the BVAAWF =FRAME=RSPCA=UFAW JointWorking Group on Renement Members of theJoint Working Groupon Renement: D.B.Morton (Chairman), M.Jennings (Secretary),A. Buckwell, R.Ewbank, C.Godfrey, B.Holgate, I. Inglis, R.James, C.Page,I. Sharman, R.Verschoyle, L.Westall &A.B.Wilson Contents Preface 2 3.6 Intraperitoneal 19 1Introduction and aimsof thereport 2 3.7 Intratracheal 20 3.8 Intravaginal 20 2Generalprinc iplesof `good practice’ 3 2.1 Planningand preparation 3 3.9 Intravenous and intra-arterial 21 2.1.1 Experimental aims 3 3.10 Oral routes 25 2.1.2 Theroute 3 3.10.1 Inclusionin an animal’s food orwater 25 2.1.3 Thesubstance 3 3.10.2 Dosingdirectly into 2.1.4 Theanimal 5 the pharynx 27 2.1.5 Thetechnique 7 3.10.3 Oral gavage 28 2.1.6 Staff and training 7 3.11 Osmotic minipumps 30 2.2 Technical preparation 3.12 Respiratory routes 31 andaftercare 8 3.12.1 Wholebody exposure 31 2.3 Generalre® nem entfor 3.12.2 Noseonly =Snout only all routes 9 exposure 32 3Re®nem entfor individual routes 3.12.3 Mask exposure 33 and procedures 13 3.13 Subcutaneous 34 3.1 Intra-articular 13 3.14 TopicalÐderm al 35 3.2 Intracerebral (intracerebro- 3.15 TopicalÐoc ular 36 ventricular) 14 3.16 Footpad 37 3.3 Intradermal 16 3.17 Uncommonroutes 38 3.4 Intramuscular 16 4Special considerations for wildanimals 38 3.5 Intranasal 18 References 39 Correspo ndenceandre q uestsfo rreprintst o:ProfessorD.B.Morton,DepartmentofBiomedicalSciences & BiomedicalEthic s, TheMed icalScho ol,UniversityofBirm ingham,Ed gbaston,Birm inghamB152TT, UK Accepted 14July 2000 # LaboratoryAnimals Ltd. -

Asthma Agents
APPROVED PA Criteria Initial Approval Date: July 10, 2019 Revised Date: January 20, 2021 CRITERIA FOR PRIOR AUTHORIZATION Asthma Agents BILLING CODE TYPE For drug coverage and provider type information, see the KMAP Reference Codes webpage. MANUAL GUIDELINES Prior authorization will be required for all current and future dose forms available. All medication-specific criteria, including drug-specific indication, age, and dose for each agent is defined in Table 1 below. Benralizumab (Fasenra®) Dupilumab (Dupixent®) Mepolizumab (Nucala®) Omalizumab (Xolair®) Reslizumab (Cinqair®) GENERAL CRITERIA FOR INITIAL PRIOR AUTHORIZATION: (must meet all of the following) • Must be approved for the indication, age, and not exceed dosing limits listed in Table 1. • Must be prescribed by or in consultation with a pulmonologist, allergist, or immunologist.1,2 • For all agents listed, the preferred PDL drug, which treats the PA indication, is required unless the patient meets the non-preferred PDL PA criteria. • Must have experienced ≥ 2 exacerbations within the last 12 months despite meeting all of the following (exacerbation is defined as requiring the use of oral/systemic corticosteroids, urgent care/hospital admission, or intubation: o Patient adherence to two long-term controller medications, including a high-dose inhaled corticosteroid 1,2 (ICS) and a long-acting beta2-agonist (LABA) listed in Table 2. ▪ Combination ICS/LABA and ICS/LABA/LAMA products meet the requirement of two controller medications. o Patient must have had an adequate trial (at least 90 consecutive days) of a leukotriene modifier or a long-acting muscarinic antagonist (LAMA) as a third long-term controller medication listed in Table 2. -

Upper and Lower Limb Blocks in Children
Upper and lower limb blocks in children Adrian Bosenberg Correspondence Email: [email protected] INTRODUCTION insulated needles are the next best option Regional anaesthesia is commonly used as an although successful blocks can be achieved with 6 rinciples of clinical anaesthesia adjunct to general anaesthesia and plays a key non-insulated needles. P role in the multimodal approach to perioperative Nerve stimulator 1,2 pain management in children. Peripheral nerve Many peripheral nerve stimulators are available. SUMMARY blockade has increased with the development of Familiarise yourself with a particular device and age-appropriate equipment, safer, long-acting This article outlines regional stick with it. Read the manufacturer’s instructions anaesthetic techniques and local anaesthetic agents, increasing experience and understand how the nerve stimulator works methods used to identify and and low complication rates. before you use it.7 block individual nerves to provide analgesia for surgical The safety of peripheral nerve blocks in children The following basic principles should be followed procedures of the upper has been established in large-scale prospective to locate a peripheral nerve or plexus accurately: and lower limbs. Expertly studies, although caudal epidural remains the performed, peripheral nerve most popular and frequently used block in • Muscle relaxants must be withheld until after blocks can provide long lasting 3-5 completion of the block. anaesthesia and analgesia infants and small children. The experience of for surgery or after injury to the operator, pathology, the site and extent of • Attach the Negative electrode to the Needle the upper or lower limbs in surgery, the child’s body habitus and the presence and the Positive electrode to the Patient using children. -

Inadequate Assessment of Adherence To€Maintenance Medication Leads
ORIGINAL ARTICLE ASTHMA Inadequate assessment of adherence to maintenance medication leads to loss of power and increased costs in trials of severe asthma therapy: results from a systematic literature review and modelling study Matshediso C. Mokoka1, Melissa J. McDonnell2, Elaine MacHale1, Breda Cushen1, Fiona Boland3, Sarah Cormican2, Christina Doherty4, Frank Doyle 5, Richard W. Costello6 and Garrett Greene1 @ERSpublications Trials of add-on therapy for severe asthma do not include adequate assessment of adherence to maintenance therapy. As a result, they suffer from a significant loss of statistical power, leading to greatly increased sample sizes and associated costs. http://ow.ly/ZCyH30nSFHc Cite this article as: Mokoka MC, McDonnell MJ, MacHale E, et al. Inadequate assessment of adherence to maintenance medication leads to loss of power and increased costs in trials of severe asthma therapy: results from a systematic literature review and modelling study. Eur Respir J 2019; 53: 1802161 [https://doi. org/10.1183/13993003.02161-2018]. ABSTRACT Adherence to inhaled maintenance therapy in severe asthma is rarely adequately assessed, and its influence on trial outcomes is unknown. We systematically determined how adherence to maintenance therapy is assessed in clinical trials of “add-on” therapy for severe asthma. We model the improvement in trial power that could be achieved by accurately assessing adherence. A systematic search of six major databases identified randomised trials of add-on therapy for severe asthma. The relationship between measuring adherence and study outcomes was assessed. An estimate of potential improvements in statistical power and sample size was derived using digitally recorded adherence trial data. -
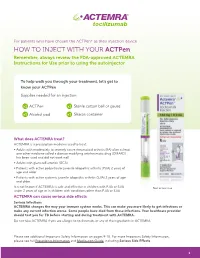
HOW to INJECT with YOUR Actpen Remember, Always Review the FDA-Approved ACTEMRA Instructions for Use Prior to Using the Autoinjector
For patients who have chosen the ACTPen® as their injection device HOW TO INJECT WITH YOUR ACTPen Remember, always review the FDA-approved ACTEMRA Instructions for Use prior to using the autoinjector To help walk you through your treatment, let’s get to know your ACTPen Supplies needed for an injection: x1 ACTPen x1 Sterile cotton ball or gauze x1 Alcohol pad x1 Sharps container What does ACTEMRA treat? ACTEMRA is a prescription medicine used to treat: • Adults with moderately to severely active rheumatoid arthritis (RA) after at least one other medicine called a disease modifying antirheumatic drug (DMARD) has been used and did not work well • Adults with giant cell arteritis (GCA) • Patients with active polyarticular juvenile idiopathic arthritis (PJIA) 2 years of age and older • Patients with active systemic juvenile idiopathic arthritis (SJIA) 2 years of age and older It is not known if ACTEMRA is safe and effective in children with PJIA or SJIA Not actual size. under 2 years of age or in children with conditions other than PJIA or SJIA. ACTEMRA can cause serious side effects Serious Infections ACTEMRA changes the way your immune system works. This can make you more likely to get infections or make any current infection worse. Some people have died from these infections. Your healthcare provider should test you for TB before starting and during treatment with ACTEMRA. Do not take ACTEMRA if you are allergic to tocilizumab, or any of the ingredients in ACTEMRA. Please see additional Important Safety Information on pages 9-10. For more Important Safety Information, please see full Prescribing Information and Medication Guide, including Serious Side Effects. -

Injectable Supramolecular Polymer–Nanoparticle Hydrogels Enhance Human Mesenchymal Stem Cell Delivery
Received: 13 July 2019 Revised: 25 September 2019 Accepted: 1 October 2019 DOI: 10.1002/btm2.10147 RESEARCH REPORT Injectable supramolecular polymer–nanoparticle hydrogels enhance human mesenchymal stem cell delivery Abigail K. Grosskopf1 | Gillie A. Roth2 | Anton A. A. Smith3 | Emily C. Gale4 | Hector Lopez Hernandez3 | Eric A. Appel3 1Department of Chemical Engineering, Stanford University, Stanford, California Abstract 2Department of Bioengineering, Stanford Stem cell therapies have emerged as promising treatments for injuries and diseases in University, Stanford, California regenerative medicine. Yet, delivering stem cells therapeutically can be complicated 3Department of Materials Science & Engineering, Stanford University, Stanford, by invasive administration techniques, heterogeneity in the injection media, and/or California poor cell retention at the injection site. Despite these issues, traditional administra- 4 Department of Biochemistry, Stanford tion protocols using bolus injections in a saline solution or surgical implants of cell- University, Stanford, California laden hydrogels have highlighted the promise of cell administration as a treatment Correspondence strategy. To address these limitations, we have designed an injectable polymer– Eric A. Appel, Department of Materials Science & Engineering, Stanford University, nanoparticle (PNP) hydrogel platform exploiting multivalent, noncovalent interactions Stanford, CA 94305. between modified biopolymers and biodegradable nanoparticles for encapsulation Email: [email protected] -

WO 2016/176089 Al 3 November 2016 (03.11.2016) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2016/176089 Al 3 November 2016 (03.11.2016) P O P C T (51) International Patent Classification: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, A01N 43/00 (2006.01) A61K 31/33 (2006.01) DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, (21) International Application Number: KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, PCT/US2016/028383 MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, (22) International Filing Date: PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, SC, 20 April 2016 (20.04.2016) SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every (26) Publication Language: English kind of regional protection available): ARIPO (BW, GH, (30) Priority Data: GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, 62/154,426 29 April 2015 (29.04.2015) US TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, (71) Applicant: KARDIATONOS, INC. [US/US]; 4909 DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, Lapeer Road, Metamora, Michigan 48455 (US).