Chapter 2 Aircraft Accident and Serious Incident Investigations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PROFILE of KYUSHU 2021 New Perspectives
Measure development of Kyushu Industrial Strategy for Kyushu-Okinawa Regional Growth―Kyushu-Okinawa Earth Strategy II The Kyushu-Okinawa Regional Council for Industrial Competitiveness promotes initiatives in four strategic areas that leverage Kyushu and Okinawa’s strengths to achieve the sustainable development of Kyushu, a gateway to Asia trying its best to work on solving new issues. The Council developed this strategy in 2014 under a public-private partnership. As of 2021, 21 projects are underway on Stage 2,incorporating PROFILE OF KYUSHU 2021 new perspectives. Strategic Areas 21 projects promoted under the Kyushu-Okinawa Earth Strategy II Project on Realizing Kyushu Hydrogen Energy Society Project on Promoting Industrial Base Formation for Clean Medical, Healthcare, Geothermal and Hot Spring Heat Energy Energy & and Cosmetics Project on Establishing Base Formation for Marine Environment Health Renewable Energy Industry Clean Project on Promoting Asia’s Advanced Base Formation for Northern Kyushu Automotive Industry Earth Project on Establishing Base for Organic Photonics and Electronics Industry Agriculture, Forestry, Sightseeing Project on Promoting Industrial Base Formation for Fisheries, and Food Kyushu and Asia Environmental Energy Industry Agriculture Tourism Project on Promoting Healthcare Industry Medical, Healthcare, Project on Creating Innovative Medical Products and Cosmetics Project on Promoting Biotechnology Industry Project on Promoting Karatsu Cosmetics Initiative Four strategic areas Four Russia Cross-cutting Initiatives -

Ai2014-5 Aircraft Serious Incident Investigation Report
AI2014-5 AIRCRAFT SERIOUS INCIDENT INVESTIGATION REPORT HOKKAIDO AIR SYSTEM CO., LTD. J A 0 3 H C November 27, 2014 The objective of the investigation conducted by the Japan Transport Safety Board in accordance with the Act for Establishment of the Japan Transport Safety Board (and with Annex 13 to the Convention on International Civil Aviation) is to prevent future accidents and incidents. It is not the purpose of the investigation to apportion blame or liability. Norihiro Goto Chairman, Japan Transport Safety Board Note: This report is a translation of the Japanese original investigation report. The text in Japanese shall prevail in the interpretation of the report. AIRCRAFT SERIOUS INCIDENT INVESTIGATION REPORT HOKKAIDO AIR SYSTEM CO., LTD. SAAB 340B, JA03HC EMERGENCY OPERATION TO AVOID COLLISION WITH THE TERRAIN ABOVE OKUSHIRI AIRPORT AROUND 11:38 JST, JUNE 4, 2011 November 7, 2014 Adopted by the Japan Transport Safety Board Chairman Norihiro Goto Member Shinsuke Endoh Member Toshiyuki Ishikawa Member Sadao Tamura Member Yuki Shuto Member Keiji Tanaka SYNOPSIS Summary of the Incident On June 4 (Saturday), 2011, a SAAB 340B, registered JA03HC, operated by Hokkaido Air System Co., Ltd., took off from Hakodate Airport as a scheduled Flight 2891. During the approach to Runway 31 of Okushiri Airport, the aircraft executed a go-around and once started climbing, but it soon reversed to descend. Consequently, at around 11:38 Japan Standard Time, its flight crew became aware of the situation and executed an emergency operation to avoid crash to the ground. The aircraft flew back to Hakodate Airport, following some holdings over Okushiri Airport. -

Public Spa Second Home Breakfast
Kamejimagawa Hot Spring Natural Hot Spring Shirasagi-no-Yu You can use our hotels as dormy inn EXPRESS Hakodate-Goryokaku SN Shinkawa-no-Yu dormy inn Tokyo Hatchobori Natural Hot Spring Kaga-no-Yusen dormy inn Kanazawa N SA B Natural Hot Spring Kirizakura-no-Yu dormy inn Kagoshima Business hotel with a spa You can use our hotels as 【TEL】+81(0)138-35-5489 【TEL】+81(0)3-5541-6700 N SA B 【TEL】+81(0)76-263-9888 N SA B dormy inn Himeji 【TEL】+81(0)99-216-5489 N S A B 【Address】29-26 Hon-cho, Hakodate City, Hokkaido 【Address】2-20-4 Shinkawa, Chuo-ku, Tokyo 【Address】2-25 Horikawa Shinmachi, Kanazawa City, Ishikawa 【TEL】+81(0)79-286-5489 【Address】17-30 Nishisengoku-cho, Kagoshima City, Kagoshima “your home” all over Japan 【 】 About 3 minutes walk from Streetcar Goryokaku Koen-mae Station. About 2 minutes walk from JR Hatchobori Station. Approx. 4 minutes About 2 minutes walk from JR Kanazawa Station. Approx. 5 km from Address 160-2 Toyozawa-cho, Himeji City, Hyogo About 2 minutes’ walk from Tram “Takamibaba” Stop Kinki Area Hokkaido Area Kyushu Area Kanto Area walk from Tokyo Metro Hibiya Line Hatchobori Station. Kanazawa-nishi Interchange of Hokuriku Expressway. 3 minutes walk from JR Sanyo Main Line/Shinkansen Himeji Station. (from JR Kagoshima-Chuo Station east exit). Chubu Area Natural Hot Spring Tenboku-no-Yu N SA B Natural Hot Spring Iwakisakura-no-Yu N SA B Suehiro-no-Yu dormy inn Akihabara SP SA M dormyinn EXPRESS Nagoya SP SA B dormy inn EXPRESS Matsue B dormy inn PREMIUM SEOUL Garosugil *Designated days only dormy inn Wakkanai dormy inn Hirosaki 【TEL】+81(0)3-5295-0012 【TEL】+81(0)52-586-6211 【TEL】+81(0)852-59-5489 【TEL】+82(0)2-518-5489 SP B 【TEL】+81(0)162-24-5489 【TEL】+81(0)172-37-5489 【Address】4-12-5 Sotokanda, Chiyoda-ku, Tokyo 【Address】1-11-8 Meieki Minami, Nakamura-ku, Nagoya City, Aichi 【Address】498-1 Asahi-machi, Matsue City, Shimane 【Address】119,Dosan-daero,Gangnam-gu,Seoul,135-887 South Korea 【 】2-7-13 Chuo Wakkanai City, Hokkaido 【Address】71-1 Hon-cho, Hirosaki City, Aomori Address About 1 minute walk from Tokyo Metro Ginza Line Suehiro-cho Station. -

Omagari Station Akita Station
Current as of January 1, 2021 Compiled by Sendai Brewery Regional Taxation Bureau Akita Results of the Japan Sake Awards - National New Sake Competition … https://www.nrib.go.jp/data/kan/ https://www.nta.go.jp/about/ SAKE Results of the Tohoku Sake Awards …… organization/sendai/release/kampyokai/index.htm MAP http://www.osake.or.jp/ Akita Brewers Association website …… Legend Shinkansen JR Line 454 Private Railway Kosaka 103 Expressway Major National Highway Town Happo City Boundary Shinkansen Station Town Fujisato 104 Gono Line JR and Private Railway Stations Higashi-Odate 103 Town Station Kazuno Odate Station 282 City Noshiro 101 Towada- Takanosu 7 Odate City Futatsui Ou Main Line Minami Station Higashi- Station City Noshiro Port Station Noshiro 103 7 Station Kanisawa IC 285 Hanawa Line 105 Kazuno-Hanawa Ou Main Line Station Odate-Noshiro Airport 282 7 Mitane Town Kitaakita City Ogata Hachirogata Town 101 Village Kamikoani Aniai Station 285 Village 341 Oga City Gojome Akita Nairiku Jūkan Railway 285 Town Oga Oga Line 101 Ikawa Station 105 Katagami Town City Oiwake Station Funakawa Port 7 Senboku City Akita City 13 Tazawako Akita Port Station n Name of City, Town, and Village No. Brewery Name Brand Name Brewery Tour Phone Number Akita Station se n a 13 k Akita City ① Akita Shurui Seizoh Co.,Ltd. TAKASHIMIZU ○Reservation 018-864-7331 n hi Araya Station S ② ARAMASA SHUZO CO.,LTD. ARAMASA × 018-823-6407 ita 46 k A AKITAJOZO CO.,LTD. YUKINOBIJIN 018-832-2818 Kakunodate ③ × ④ Akita Shuzo Co.,Ltd. Suirakuten ○Reservation 018-828-1311 Daisen Station Akita Shurui Seizoh Co.,Ltd. -

Effects of Constructing a New Airport on Ishigaki Island
Island Sustainability II 181 Effects of constructing a new airport on Ishigaki Island Y. Maeno1, H. Gotoh1, M. Takezawa1 & T. Satoh2 1Nihon University, Japan 2Nihon Harbor Consultants Ltd., Japan Abstract Okinawa Prefecture marked the 40th anniversary of its reversion to Japanese sovereignty from US control in 2012. Such isolated islands are almost under the environment separated by the mainland and the sea, so that they have the economic differences from the mainland and some policies for being active isolated islands are taken. It is necessary to promote economical measures in order to increase the prosperity of isolated islands through initiatives involving tourism, fisheries, manufacturing, etc. In this study, Ishigaki Island was considered as an example of such an isolated island. Ishigaki Island is located to the west of the main islands of Okinawa and the second-largest island of the Yaeyama Island group. Ishigaki Island falls under the jurisdiction of Okinawa Prefecture, Japan’s southernmost prefecture, which is situated approximately half-way between Kyushu and Taiwan. Both islands belong to the Ryukyu Archipelago, which consists of more than 100 islands extending over an area of 1,000 km from Kyushu (the southwesternmost of Japan’s four main islands) to Taiwan in the south. Located between China and mainland Japan, Ishigaki Island has been culturally influenced by both countries. Much of the island and the surrounding ocean are protected as part of Iriomote-Ishigaki National Park. Ishigaki Airport, built in 1943, is the largest airport in the Yaeyama Island group. The runway and air security facilities were improved in accordance with passenger demand for larger aircraft, and the airport became a tentative jet airport in May 1979. -

Towada-Hachimantai National Park Guide Book
Towada-Hachimantai National Park Guide Book 十和田八幡平国立公園 Feel the landscapes of Northern Tohoku that change from season to season in the vast nature 四季それぞれに美しい北東北を自然の中で体感 In Japan, each of the four seasons has its own colour that allows visitors to truly feel its atmosphere. Especially in Tohoku, where winter is crucially rigorous, people wait for the arrival of spring, sing the joys of summer, and appreciate the rich harvests of autumn. There are many things in Tohoku that bring joy to people throughout the year. Towada-Hachimantai National Park is located in the mountainous area of Northern Japan, and lies upon the three prefectures of Northern Tohoku. It is composed of “Towada-Hakkoda Area” , on the northern side that consists of Lake Towada, Oirase Gorge and Hakkoda Mountains and “Hachimantai Area” , on the southern side that consists of Mt. Hachimantai, Mt. Akita-Komagatake and Mt. Iwate. Both areas are very rich in natural resources, such as forests, lakes and marshes, and a wide variety of fauna and flora. There are also many onsen spots where you can immerse your body and soul. 01 Shin-Hakodate-Hokuto Hakodate Airport Oma To Tomakomai Aomori Contents ● Tohoku Shinkansen about 3hr 10 min. Tokyo Station Shin-Aomori Station Towada-Hakkoda Area Shin-Aomori Station Airplane about 1hr 20 min. Haneda Airport Misawa Airport Airplane about 1hr 15 min. Haneda Airport Aomori Airport Tohoku Shinkansen about 1hr 30 min. Sendai Station Shin-Aomori Station Hokkaido / Tohoku Shinkansen about 1hr Shin-Hakodate-Hokuto Station Shin-Aomori Station Highway Bus about 4hr 50 min. Sendai Station Aomori Station Joy of Spring Iwate 04 春の歓喜 Tohoku Shinkansen about 2hr 20 min. -

Invincible Investment Corporation
Invincible Investment Corporation Asset Management Report Fiscal Period ended June 30, 2019 (January 1, 2019 to June 30, 2019) Content Greetings from Naoki Fukuda, Executive Director of Invincible Investment Corporation and President & CEO of Consonant Investment Management Co., Ltd. Increase in Asset Size and Initiatives for Asset recycling Properties Acquired in July 2019 Asset Management Report Audited Financial Statements for the 32th Fiscal Period (from January 1, 2019 to June 30, 2019) Domestic Portfolio Map (As of August 31, 2019) Financial Conditions Overview of Unitholders/Investment Greetings from Naoki Fukuda, Executive Director of Invincible Investment Corporation and President & CEO of Consonant Investment Management Co., Ltd. We would like to take this opportunity to express our sincere gratitude to all unitholders of Invincible Investment Corporation (“INV”) for your continued support. We hereby provide you with a report on INV’s asset management and financial results for the 32nd fiscal period (covering the period from January 1, 2019 to June 30, 2019; the “Reporting Period”). During the Reporting Period, INV changed the investment structure for two overseas hotels to a direct ownership structure of the underlying assets from investments in anonymous associations on May 9, 2019. The change in ownership structure was made to adapt to an amended Act on Special Measures Concerning Taxation executed on April 1, 2019 and completely resolves the tax issue regarding conduit requirements. In June 2019, INV sold two residential assets for extremely favorable terms as a continuation of its asset recycling program. The total sale price was JPY 39.9 billion, resulting in a gain of JPY 11.1 billion. -

Ai2009-1 Aircraft Serious Incident Investigation Report
AI2009-1 AIRCRAFT SERIOUS INCIDENT INVESTIGATION REPORT JAPAN AIRLINES INTERNATIONAL CO., LTD. J A 8 9 0 4 JAPAN AIRLINES INTERNATIONAL CO., LTD. J A 8 0 2 0 January 23, 2009 Japan Transport Safety Board The investigation for this report was conducted by Japan Transport Safety Board, JTSB, about the aircraft serious incident of JAPAN AIRLINES INTERNATIONAL , B747-400D registration JA8904 and JAPAN AIRLINES INTERNATIONAL, MD-90-30 registration JA8020 in accordance with Japan Transport Safety Board Establishment Law and Annex 13 to the Convention on International Civil Aviation for the purpose of determining causes of the aircraft serious incident and contributing to the prevention of accidents/incidents and not for the purpose of blaming responsibility of the serious incident. This English version of this report has been published and translated by JTSB to make its reading easier for English speaking people who are not familiar with Japanese. Although efforts are made to translate as accurately as possible, only the Japanese version is authentic. If there is any difference in the meaning of the texts between the Japanese and English versions, the text in the Japanese version prevails. Norihiro Goto, Chairman, Japan Transport Safety Board AIRCRAFT SERIOUS INCIDENT INVESTIGATION REPORT 1. JAPAN AIRLINES INTERNATIONAL CO., LTD. BOEING 747-400D JA8904 2. JAPAN AIRLINES INTERNATIONAL CO., LTD. DOUGLAS MD-90-30 JA8020 AT ABOUT 10:33 JST FEBRUARY 16, 2008 ON THE RUNWAY 01R OF NEW CHITOSE AIRPORT December 10, 2008 Adopted by the Japan Transport Safety Board (Aircraft Sub-committee) Chairman Norihiro Goto Member Yukio Kusuki Member Shinsuke Endo Member Noboru Toyooka Member Yuki Shuto Member Akiko Matsuo - 1 - 1 PROCESS AND PROGRESS OF AIRCRAFT SERIOUS INCIDENT INVESTIGATION 1.1 Summary of the Serious Incident The event covered by this report falls under the category of “an aborted take-off on an engaged runway” as stipulated in Clause 1, Article 166-4 of the Civil Aeronautics Regulations of Japan, and is classified as an Aircraft Serious Incident. -
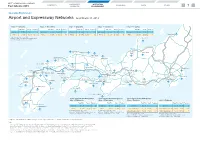
7. Airport and Expressway Networks (PDF, 352KB)
WEST JAPAN RAILWAY COMPANY CORPORATE OPERATING CONTENTS BUSINESS DATA OTHER Fact Sheets 2019 OVERVIEW ENVIRONMENT 7 Operating Environment Airport and Expressway Networks As of March 31, 2019 Tokyo — Fukuoka Tokyo — Hiroshima Tokyo — Okayama Tokyo — Kanazawa Tokyo — Toyama Travel Time Fare (¥) Frequency Travel Time Fare (¥) Frequency Travel Time Fare (¥) Frequency Travel Time Fare (¥) Frequency Travel Time Fare (¥) Frequency Shinkansen 4h 46m 22,950 31 Shinkansen 3h 44m 19,080 46 Shinkansen 3h 09m 17,340 60 Shinkansen 2h 28m 14,120 24 Shinkansen 2h 08m 12,730 24 Niigata Airport Airlines 3h 00m 41,390 54 (19) Airlines 3h 30m 34,890 18 Airlines 3h 10m 33,990 10 Airlines 2h 50m 24,890 10 Airlines 2h 30m 24,890 4 Travel Time and Fare: JAL or ANA Noto Airport Frequency: All airlines. Numbers in parentheses are frequency excluding those of JAL or ANA. Kanazawa Izumo Airport Komatsu Toyama Airport Yonago Airport Airport Tottori Airport Yonago Hagi Iwami Airport Izumo Tajima Airport Gotsu Hamada Tsuruga Yamaguchi Ube Airport Yamaguchi HiroshimaHiroshima Hiroshima Airport Okayama Airport Maibara Kitakyushu Ibaraki Airport Onomichi Hakata KomakiKomaki AirportAirport Okayama KobeKobe ItamiItami AirportAirport Fukuoka Airport Kitakyushu Airport KKurashikiurashiki SSuitauita Iwakuni Kintaikyo NagoyaNagoya Sasebo Tosu Airport Sakaide Shin-OsakaShin-Osaka Tokyo Saga Airport Imabari Kobe Airport Narita Airport Matsuyama Airport Takamatsu Airport Naruto KansaiKansai AirportAirport Haneda Airport Oita Airport Kansai Nagasaki International Airport Chubu International -

Kyushu China Taipei
Sapporo 北京 Japan Seoul South Korea Hiroshima Busan Oita Tokyo Nagoya Fukuoka Osaka Saga Nagasaki Kumamoto Kagoshima Miyazaki Shanghai Kyushu China Taipei Hong Kong Macao Hanoi Taiwan Thailand Vietnam Philippines Bangkok Manila Ho chi minh Malaysia Kuala Lumpur Singapore Singapore Shimonoseki Mojiko Moji Kokura Hakata Takeo Saga Tosu Haiki Onsen Shin Tosu Hita Yufuin Beppu Sasebo Kurume Oita Chikugo Funagoya Chugoku Expressway Huis Ten Bosch Arita Shin Omuta Miyaji Saiki Shin Tamana Aso Kumamoto Higo Ozu Nagasaki Nobeoka Shin Shimonoseki Misumi Yatsushiro Shin Yatsushiro Hitoyoshi Shin Minamata Izumi Yoshimatsu Shimonoseki IC Miyazaki Kirishima Onsen Minami Miyazaki Sendai Kirishima Jingu Aoshima Mojiko IC Hayato Kitago Kagoshima Obi Moji Port Kagoshima Chuo Nichinan Kyushu Expressway Nango Makurazaki Ibusuki Kokura Kitakyushu (Kokura) Shinmonji Port Fukuoka Kokura Higashi IC Kitakyushu Airport Kitakyushu Suou Nada Sea Airport Hakata Port International Terminal Fukuoka IC Hakata Port Hakata Nakatsu Fukuoka Airport Fukuoka Airport Buzen IC Hakata Yobuko Tenjin Usa Beppu Expressway Nakatsu IC Dazaifu IC Oita Airport Nishi Karatsu Oita Airport Kosoku Kiyama Karatsu Saga Tosu JCT Oita Hiji IC Oita AirportRoad Karatsu IC Tosu IC Hirado Imafuku IC Matsuura Shin Tosu Hita IC Oita Expressway Yamashirokubara IC Taniguchi IC Nagasaki Expressway Kurume IC Gulf of Beppu Saga Yamato IC Hita Beppu IC Kurume Hita Yufuin Imari Kurume Saga Yufuin IC Beppu Saza IC Imari Oita Saga Beppu Takeo Onsen Yufuin Oita Sasebo Chikugo Funagoya Amagase Oita IC Nishi-Kyushu -

Hokkaido Map Scenic Spots in the Kamikawa Area
Cape Soya Wakkanai Rebun Island Wakkanai Airport Scenic spots in the Kafuka Oshidomari Kamikawa area Mt. Rishiri Hokkaido Map ▲ Rishiri Nakagawa/Aerial photo of Teshio River Saku Otoineppu/The place that Hokkaido was named Rishiri Island Toyotomi Onsen (Mizukiri Contest (Stone-skipping Contest)) in July Airport Toyotomi Nakagawa Otoineppu Etorofu Island 40 Bifuka/Farm inn tonttu Horokanai/Santozan Mountain Range Shibetsu/Suffolk Land Kenbuchi/Nano in July Wassamu/A street lined with white birch in winter Bifuka Yagishiri Chiebun Sunflower fields● ●Nayoro Onsen Teuri Okhotsk Island Island Haboro Nayoro Mombetsu Lake Shumarinai Shimokawa Monbetsu ●Icebreaker Airport "Garinko-go" ●Takinoue Park Shiretoko Peninsula Kamiyubetsu World Sheep Museum● Shibetsu Tulip Park ● Takinoue Lake Saroma Nayoro/Sunflower fields Shimokawa/Forest in winter Asahikawa/Kamuikotan Library of picture books● Mt. Rausu Kenbuchi ▲ Engaru Lake Notoro Wassamu Horokanai Mt. Teshio Abashiri Utoro Onsen Rausu ▲ Maruseppu Lake Abashiri Rumoi Takasu Pippu ●Maruseppu Abashiri-Kohan Onsen Kunashiri Island Onsen Shiretoko-Shari Mashike Aibetsu Memanbetsu ●Tohma Limestone cave Airport Kitami Snow Crystal Museum● Tohma Kamikawa ● Shikotan Island Asahiyama Zoo 39 ▲ Asahikawa Asahikawa Mt. Shari ▲ 237 Airport Sounkyo Onsen Mt. Shokanbetsu 39 Onneyu Onsen Higashikagura Kawayu Onsen ▲ Asahidake Onsen Lake Kussharo Higashikawa Mt. Asahidake Tenninkyo Onsen Habomai Islands Takikawa Ashibetsu Biei Takasu/Palette Hills in May Pippu/The top of Pippu Ski Area in Jan. Aibetsu/Kinokonosato park golf course in May Shirogane Onsen ▲ Lake Mashu Shintotsukawa Kamifurano Mt. Tomuraushi Lake Akan Mashu Nakashibetsu Airport 12 Akan Mashu Cape Shakotan Nakafurano ▲ Akanko Onsen Mt. Tokachi Nukabira Onsen ▲ Onsen Mt. Oakan Bibai Furano Nemuro Cape Kamui Nemuro Peninsula Ishikari Bay 44 Otaru Iwamizawa 38 Ashoro Minamifurano Yoichi Sapporo ▲ Hoshino Resorts Shiranuka Yubari Mt. -

Aichi Prefecture
Coordinates: 35°10′48.68″N 136°54′48.63″E Aichi Prefecture 愛 知 県 Aichi Prefecture ( Aichi-ken) is a prefecture of Aichi Prefecture Japan located in the Chūbu region.[1] The region of Aichi is 愛知県 also known as the Tōkai region. The capital is Nagoya. It is the focus of the Chūkyō metropolitan area.[2] Prefecture Japanese transcription(s) • Japanese 愛知県 Contents • Rōmaji Aichi-ken History Etymology Geography Cities Towns and villages Flag Symbol Mergers Economy International relations Sister Autonomous Administrative division Demographics Population by age (2001) Transport Rail People movers and tramways Road Airports Ports Education Universities Senior high schools Coordinates: 35°10′48.68″N Sports 136°54′48.63″E Baseball Soccer Country Japan Basketball Region Chūbu (Tōkai) Volleyball Island Honshu Rugby Futsal Capital Nagoya Football Government Tourism • Governor Hideaki Ōmura (since Festival and events February 2011) Notes Area References • Total 5,153.81 km2 External links (1,989.90 sq mi) Area rank 28th Population (May 1, 2016) History • Total 7,498,485 • Rank 4th • Density 1,454.94/km2 Originally, the region was divided into the two provinces of (3,768.3/sq mi) Owari and Mikawa.[3] After the Meiji Restoration, Owari and ISO 3166 JP-23 Mikawa were united into a single entity. In 187 1, after the code abolition of the han system, Owari, with the exception of Districts 7 the Chita Peninsula, was established as Nagoya Prefecture, Municipalities 54 while Mikawa combined with the Chita Peninsula and Flower Kakitsubata formed Nukata Prefecture. Nagoya Prefecture was renamed (Iris laevigata) to Aichi Prefecture in April 187 2, and was united with Tree Hananoki Nukata Prefecture on November 27 of the same year.