Work-Related Lung Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Occupational Airborne Particulates
Environmental Burden of Disease Series, No. 7 Occupational airborne particulates Assessing the environmental burden of disease at national and local levels Tim Driscoll Kyle Steenland Deborah Imel Nelson James Leigh Series Editors Annette Prüss-Üstün, Diarmid Campbell-Lendrum, Carlos Corvalán, Alistair Woodward World Health Organization Protection of the Human Environment Geneva 2004 WHO Library Cataloguing-in-Publication Data Occupational airborne particulates : assessing the environmental burden of disease at national and local levels / Tim Driscoll … [et al.]. (Environmental burden of disease series / series editors: Annette Prüss-Ustun ... [et al.] ; no. 7) 1.Dust - adverse effects 2.Occupational exposure 3.Asthma - chemically induced 4.Pulmonary disease, Chronic obstructive - chemically induced 5.Pneumoconiosis - etiology 6.Cost of illness 7.Epidemiologic studies 8.Risk assessment - methods 9.Manuals I.Driscoll, Tim. II.Prüss-Üstün, Annette. III.Series. ISBN 92 4 159186 2 (NLM classification: WA 450) ISSN 1728-1652 Suggested Citation Tim Driscoll, et al. Occupational airborne particulates: assessing the environmental burden of disease at national and local levels. Geneva, World Health Organization, 2004. (Environmental Burden of Disease Series, No. 7). © World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). -

Dust Exposure and Byssinosis Among Cotton Textile Workers in Dar Es Salaam, Tanzania
MOJ Public Health Research Article Open Access Dust exposure and byssinosis among cotton textile workers in Dar es salaam, Tanzania Abstract Volume 9 Issue 6 - 2020 Background: Cotton dust exposure increases the risk of developing lung diseases including Luco P Mwelange, Simon Mamuya, Gloria Byssinosis. The prevalence of byssinosis is more in developing countries compare to developed countries. For the past forty years there are little information known about the Sakwari, Witness John Axwesso Department of Environmental and Occupational Health, prevalence of byssinosis and its associated risk factors among textile workers in Tanzania. Muhimbili University of Health and Allied Sciences, Tanzania Objective: The study aimed to assess dust exposure and associated risk factors among textile workers, in Dar es Salaam, Tanzania. Correspondence: Luco P Mwelange, Muhimbili University of Health and Allied Sciences, Tanzania, Tel+255655049524, Material and methods: The study design was descriptive cross sectional study conducted Email from March to August 2019. Stratified sampling technique was used to obtain 325 participants (exposed 164 and control 161) respectively. A modified British Medical Received: October 29, 2020 | Published: November 30, 2020 Research Council (BMRC) questionnaire and Side Kick Casella Pump were used for data collection. Data were analyzed using Statistical Package for Social Science software 23 versions. Chi square test and Binary logistic regression were performed to check for association. A 95% confidence Interval with a significance expressed in P˂0.05 was used. Results: Prevalence of byssinosis in the exposed group was 18.9% and 6.2% in the control group. Respiratory symptoms such as Coughing more days in three consecutive months (P˂0.001), wheezing (P˂0.02), dyspnoea I (P˂0.03), dyspnoea II (P˂0.007), and dyspnoea III (P˂0.002), were higher among exposed group compare to control group and the differences were statistically significant. -

PICTORIAL REVIEW Thoracic Involvement in Connective
JBR–BTR, 2015, 98: 3-19. PICTORIAL REVIEW THORACIC INVOLVEMENT IN CONNECTIVE TISSUE DISEASES: RADIO- LOGICAL PATTERNS AND FOLLOW-UP G. Serra1, A.-L. Brun1, P. Ialongo2, M.-L. Chabi1, P.A. Grenier1 Connective tissue diseases (CTDs) are a heterogeneous group of idiopathic inflammatory diseases involving various organs. A thoracic involvement is frequent, and chest-CT represents the imaging technique of reference in its assess- ment. Pulmonary abnormalities related to CTDs are various; although several disease-specific aspects have been described, the two most clinically relevant complications are represented by interstitial lung disease and pulmonary arterial hypertension. The early identification of a thoracic involvement, with the adoption of specific therapies, can significantly change patient’s prognosis. The aim of this article is to review the most common typical and atypical CT features of thoracic involvement occurring in CT, especially focusing on interstitial lung disease. Key-word: Connective tissue, diseases – Lung, interstitial disease – Hypertension, pulmonary. Connective tissue diseases (CTDs) at the time of diagnosis of CTD, or chronic inflammation in the alveolar are a heterogeneous group of in- more commonly manifest later in the walls. The patients usually response flammatory diseases derived from course of the disease (5, 6). well to corticosteroid therapy and an immunologic deregulation affect- The most common histopatholog- have a good prognosis. However pa- ing various organs. A thoracic in- ic patterns of ILD seen in the setting tients with OP associated with CTD volvement (pulmonary, pleural or of CTDs are non specific interstitial seem to have a greater tendency to mediastinal) can be frequently pneumonia (NSIP), usual interstitial develop fibrosis and a higher mortal- found; its frequency and expression pneumonia (UIP), organizing pneu- ity than patients with cryptogenic depends on the type of disease, and monia (OP), diffuse alveolar damage OP (5, 6). -

Management of Malignant Pleural Effusions an Official ATS/STS/STR Clinical Practice Guideline David J
AMERICAN THORACIC SOCIETY DOCUMENTS Management of Malignant Pleural Effusions An Official ATS/STS/STR Clinical Practice Guideline David J. Feller-Kopman*, Chakravarthy B. Reddy*, Malcolm M. DeCamp, Rebecca L. Diekemper, Michael K. Gould, Travis Henry, Narayan P. Iyer, Y. C. Gary Lee, Sandra Z. Lewis, Nick A. Maskell, Najib M. Rahman, Daniel H. Sterman, Momen M. Wahidi, and Alex A. Balekian; on behalf of the American Thoracic Society, Society of Thoracic Surgeons, and Society of Thoracic Radiology THIS OFFICIAL CLINICAL PRACTICE GUIDELINE WAS APPROVED BY THE AMERICAN THORACIC SOCIETY OCTOBER 2018, THE SOCIETY OF THORACIC SURGEONS JUNE 2018, AND THE SOCIETY OF THORACIC RADIOLOGY JULY 2018 Background: This Guideline, a collaborative effort from the MPE; 3) using either an indwelling pleural catheter (IPC) or American Thoracic Society, Society of Thoracic Surgeons, and chemical pleurodesis in symptomatic patients with MPE and Society of Thoracic Radiology, aims to provide evidence-based suspected expandable lung; 4) performing large-volume recommendations to guide contemporary management of patients thoracentesis to assess symptomatic response and lung expansion; with a malignant pleural effusion (MPE). 5) using either talc poudrage or talc slurry for chemical pleurodesis; 6) using IPC instead of chemical pleurodesis in patients with Methods: A multidisciplinary panel developed seven questions nonexpandable lung or failed pleurodesis; and 7) treating using the PICO (Population, Intervention, Comparator, and IPC-associated infections with antibiotics and not removing the Outcomes) format. The GRADE (Grading of Recommendations, catheter. Assessment, Development and Evaluation) approach and the Evidence to Decision framework was applied to each question. Recommendations Conclusions: These recommendations, based on the best available were formulated, discussed, and approved by the entire panel. -

Pneumoconiosis
Prim Care Respir J 2013; 22(2): 249-252 PERSPECTIVE Pneumoconiosis *Paul Cullinan1, Peter Reid2 1 Consultant Physician, Royal Brompton and Harefield NHS Foundation Trust, London, UK 2 Consultant Physician, Western General Hospital, Edinburgh, UK Introduction Figure 1. Asbestosis; the HRCT scan shows the typical The pneumoconioses are parenchymal lung diseases that arise from picture of subpleural fibrosis (solid arrow); in addition inhalation of (usually) inorganic dusts at work. Some such dusts are there is diffuse, left-sided pleural thickening (broken biologically inert but visible on a chest X-ray or CT scan; thus, while arrow), characteristic too of heavy asbestos exposure they are radiologically alarming they do not give rise to either clinical disease or deficits in pulmonary function. Others – notably asbestos and crystalline silica – are fibrogenic so that the damage they cause is through the fibrosis induced by the inhaled dust rather than the dust itself. Classically these give rise to characteristic radiological patterns and restrictive deficits in lung function with reductions in diffusion capacity; importantly, they may progress long after exposure to the causative mineral has finished. In the UK and similar countries asbestosis is the commonest form of pneumoconiosis but in less developed parts of the world asbestosis is less frequent than silicosis; these two types are discussed in detail below. Other, rarer types of pneumoconiosis include stannosis (from tin fume), siderosis (iron), berylliosis (beryllium), hard metal disease (cobalt) and coal worker’s pneumoconiosis. Asbestosis Clinical scenario How is the diagnosis made? Asbestosis is the ‘pneumoconiosis’ that arises from exposure to A man of 78 reports gradually worsening breathlessness; he has asbestos in the workplace.1 The diagnosis is made when, on the no relevant medical history of note and has never been a regular background of heavy occupational exposure to any type of asbestos, smoker. -
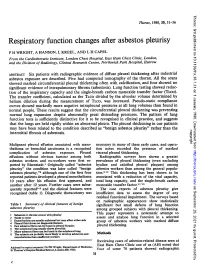
Respiratory Function Changes After Asbestos Pleurisy
Thorax: first published as 10.1136/thx.35.1.31 on 1 January 1980. Downloaded from Thorax, 1980, 35, 31-36 Respiratory function changes after asbestos pleurisy P H WRIGHT, A HANSON, L KREEL, AND L H CAPEL From the Cardiothoracic Institute, London Chest Hospital, East Ham Chest Clinic, London, and the Division of Radiology, Clinical Research Centre, Northwick Park Hospital, Harrow ABSTRACT Six patients with radiographic evidence of diffuse pleural thickening after industrial asbestos exposure are described. Five had computed tomography of the thorax. All the scans showed marked circumferential pleural thickening often with calcification, and four showed no significant evidence of intrapulmonary fibrosis (asbestosis). Lung function testing showed reduc- tion of the inspiratory capacity and the single-breath carbon monoxide transfer factor (TLco). The transfer coefficient, calculated as the TLCO divided by the alveolar volume determined by helium dilution during the measurement of TLco, was increased. Pseudo-static compliance curves showed markedly more negative intrapleural pressures at all lung volumes than found in normal people. These results suggest that the circumferential pleural thickening was preventing normal lung expansion despite abnormally great distending pressures. The pattern of lung function tests is sufficiently distinctive for it to be recognised in clinical practice, and suggests that the lungs are held rigidly within an abnormal pleura. The pleural thickening in our patients may have been related to the condition described as "benign asbestos pleurisy" rather than the copyright. interstitial fibrosis of asbestosis. Malignant pleural effusion associated with meso- necessary in many of these early cases, and opera- thelioma or bronchial carcinoma is a recognised tion notes recorded the presence of marked http://thorax.bmj.com/ complication of asbestos exposure. -

Occupational Lung Diseases
24 Occupational lung diseases Introduction i Occupational diseases are often thought to be Key points uniquely and specifically related to factors in the work environment; examples of such diseases are • Systematic under-reporting and the pneumoconioses. However, in addition to other difficulties in attributing causation both contribute to underappreciation of the factors (usually related to lifestyle), occupational burden of occupational respiratory exposures also contribute to the development or diseases. worsening of common respiratory diseases, such • Work-related exposures are estimated as chronic obstructive pulmonary disease (COPD), to account for about 15% of all adult asthma and lung cancer. asthma cases. • Boththe accumulation of toxic dust in the Information about the occurrence of occupational lungs and immunological sensitisation respiratory diseases and their contribution to to inhaled occupational agents can morbidity and mortality in the general population is cause interstitial lung disease. provided by different sources of varying quality. Some • Despite asbestos use being phased European countries do not register occupational out, mesothelioma rates are forecast diseases and in these countries, information about to continue rising owing to the long latency of the disease. the burden of such diseases is completely absent. • The emergence of novel occupational In others, registration is limited to cases where causes of respiratory disease in compensation is awarded, which have to fulfil specific recent years emphasises the need for administrative or legal criteria as well as strict continuing vigilance. medical criteria; this leads to biased information and underestimation of the real prevalence. Under- reporting of occupational disease is most likely to occur in older patients who are no longer at work but whose condition may well be due to their previous job. -

Pneumoconiosis in Coalminers
6I8 POSTGRADUATE MEDICAL JOURNAL December I949 Postgrad Med J: first published as 10.1136/pgmj.25.290.618 on 1 December 1949. Downloaded from IRVINE, L. G., SIMSON, F. W., and STRACHAN, A. S. (1930), NEW YORK STATE DEPARTMENT OF LABOUR (1949), Proc. Intern. Conf. on Silicosis in Johannesburg, I.L.O. Studies Monthly Review, 28, No. 4, April. and Reports, Series F. (Industrial Hygiene), No. I3, p. 259. PERRY, K. M. A. (1948), Proc. Ninth Intern. Cong. of Ind. Med., JONES, W. R. (I933), ,. of Hyg., 33, 307. London (in the press). KETTLE, E. H. (I932), Y. Path. and Bat., 35, 395. KETTLE, E. H. (I934), Ibid., 38, 20o. POLICARD, A. (1947), Proc. Conf. of the Institution of Mining KING, E. J. (I945), M.R.C. Special Report Series, No. 250, p. 73. Engineers and Institution of Mining and Metalurgy, London, KING, E. J. (I947) Occ. Med., 4, 26. P. 24. KING, E. J., WRI6HT, B. M., and RAY, S. C. (I949), Paper read ROGERS, E. (i944), Paper read to the British Tuberculosis Associa- to the Path. Soc., Great Britain, January, 1949. tion. McLAUGHLIN, A. I. G., ROGERS, E., and DUNHAM, K. C. (I949), Brit. 3Y. Ind. Med., 6, I84. SHAVER, C. G. (1948), Radiology, 50, 760. MINERS' PHTHISIS MEDICAL BUREAU OF SOUTH SHAVER, C. G., and RIDDELL, A. R. (I947), J. Id. Hyg. and AFRICA (1946), Report for the Three Years ending Jy 31, Tox., 29, 145. I944 (South African Government Printer). VORWALD, A. J., and CARR, J. W. (1938), Amer. J7. Path., 14,49. PNEUMOCONIOSIS IN COAL MINERS By J. -

Progressive Plasterer's Pneumoconiosis Complicated By
Kurosaki et al. BMC Pulmonary Medicine (2019) 19:6 https://doi.org/10.1186/s12890-018-0776-4 CASEREPORT Open Access Progressive plasterer’s pneumoconiosis complicated by fibrotic interstitial pneumonia: a case report Fumio Kurosaki1,2*, Tamiko Takemura3, Masashi Bando1, Tomonori Kuroki1,2, Toshio Numao2, Hiroshi Moriyama4 and Koichi Hagiwara1 Abstract Background: Although the prevalence of pneumoconiosis has been decreasing due to improvements in working conditions and regular health examinations, occupational hygiene measures are still being established. Plasterers encounter a number of hazardous materials that may be inhaled in the absence of sufficient protection. Case presentation: A 64-year-old man who plastered without any dust protection for more than 40 years was referred to our hospital with suspected interstitial pneumonia. Mixed dust pneumoconiosis and an unusual interstitial pneumonia (UIP) pattern with fibroblastic foci were diagnosed by video-assisted thoracoscopic surgery, and an elemental analysis detected elements included in plaster work materials. Despite the cessation of plaster work and administration of nintedanib, the patient developed advanced respiratory failure. Conclusion: Plasterers are at an increased risk of pneumoconiosis and may have a poor prognosis when complicated by the UIP pattern. Thorough dust protection and careful monitoring are needed. Keywords: Plasterer, Pneumoconiosis, Usual interstitial pneumonia, Elemental analysis Background unusual interstitial pneumonia (UIP) pattern, the cause of With energy transition from coal to oil and nuclear power, which was identified as plaster work by an elemental coal mines completely disappeared by the early first analysis. Therefore, plasterers need to take proper coun- decade of the 2000s in Japan. Furthermore, improvements termeasures for dust prevention and undergo regular in industrial hygiene and vocational education have examinations. -

Pathological Aspects of Asbestosis
POSTGRAD. MED. J. (1966), 42, 613. Postgrad Med J: first published as 10.1136/pgmj.42.492.613 on 1 October 1966. Downloaded from PATHOLOGICAL ASPECTS OF ASBESTOSIS D. O'B. HOURIHANE, M.D., M.C.Path., D.C.P.(Lond.), M.R.C.P.I. W. T. E. MCCAUGHEY, M.D., M.C.Path. School ofPathology, Trinity College, Dublin WIDESPREAD recognition of asbestosis dates from the work of Merewether and Price in 1930. They investigated 363 asbestos workers and concluded that there was a pneumoconiosis resulting from asbestos inhalation, that this condition shortened life, and that measures to diminish the atmospheric concentration of asbestos dust would reduce the incidence of the disease. In 1931 asbestosis was accepted as a compensatable disease in Great Britain and steps were taken to reduce the risk in the asbestos industry. 18 years later Wyers (1949) found that the age at death in this disorder had Protected by copyright. increased and that finger-clubbing had become more common. He suggested that these changes were due to a more chronic form of the disease resulting from improved dust control in the industry following the legislation of 1931. Currently however, the number of new cases of asbestosis in Great Britain is increasing, their frequency suggesting an incidence rate of at least five per thousand of those occupation- ally exposed (McVittie, 1965). Though earlier reports indicated that tuberculosis was common in asbestosis (Wyers, 1949; Gloyne, 1951; Bonser, Foulds and Stewart, 1955) it appears to be a rare I 0 n < ,. ' complication at the present time (Buchanan, 1965). -

08-0205: N.M. and DEPARTMENT of the NAVY, PUGET S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) N.M., Appellant ) ) and ) Docket No. 08-205 ) Issued: September 2, 2008 DEPARTMENT OF THE NAVY, PUGET ) SOUND NAVAL SHIPYARD, Bremerton, WA, ) Employer ) __________________________________________ ) Appearances: Oral Argument July 16, 2008 John Eiler Goodwin, Esq., for the appellant No appearance, for the Director DECISION AND ORDER Before: DAVID S. GERSON, Judge COLLEEN DUFFY KIKO, Judge JAMES A. HAYNES, Alternate Judge JURISDICTION On October 30, 2007 appellant filed a timely appeal from a November 17, 2006 decision of the Office of Workers’ Compensation Programs denying his occupational disease claim. Pursuant to 20 C.F.R. §§ 501.2(c) and 501.3, the Board has jurisdiction over the merits of the claim. ISSUE The issue is whether appellant has established that he sustained occupational asthma in the performance of duty due to accepted workplace exposures. On appeal, he, through his attorney, asserts that the Office did not provide Dr. William C. Stewart, the impartial medical examiner, with a complete, accurate statement of accepted facts. FACTUAL HISTORY On December 8, 2004 appellant, then a 57-year-old insulator, filed an occupational disease claim (Form CA-2) asserting that he sustained occupational asthma and increasing shortness of breath due to workplace exposures to fiberglass, silicates, welding smoke, polychlorobenzenes, rubber, dusts, gases, fumes and smoke from “burning out” submarines from 1991 through January -

National Occupational Research Agenda (Nora)
NATIONAL OCCUPATIONAL RESEARCH AGENDA (NORA) NATIONAL OCCUPATIONAL RESEARCH AGENDA FOR HEALTHCARE AND SOCIAL ASSISTANCE (HCSA) February 2019 Developed by the NORA HCSA Council 1 . For more information about the National Occupational Research Agenda (NORA), visit the web site: https://www.cdc.gov/niosh/nora/ For monthly updates on NORA, subscribe to NIOSH eNews at www.cdc.gov/niosh/eNews Disclaimer This is a product of the National Occupational Research Agenda (NORA) Healthcare and Social Assistance Sector Council. It does not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, or U.S. Department of Health and Human Services. 2 INTRODUCTION What is the National Occupational Research Agenda? The National Occupational Research Agenda (NORA) is a partnership program to stimulate innovative research and workplace interventions. In combination with other initiatives, the products of this program are expected to reduce the occurrence of injuries and illnesses at work. Unveiled in 1996, NORA has become a research framework for the Nation and the National Institute for Occupational Safety and Health (NIOSH). Diverse parties collaborate to identify the most critical issues in workplace safety and health and develop research objectives for addressing those needs. NORA enters its third decade in 2016 with an enhanced structure. The ten sectors formed for the second decade will continue to prioritize occupational safety and health research by major areas of the U.S. economy. In addition, there are seven cross-sectors organized according the major health and safety issues affecting the U.S. working population. While NIOSH is serving as the steward to move this effort forward, it is truly a national effort.