Ocular Disease Management 18Th18th Eeditiondition
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Antiseptics and Disinfectants for the Treatment Of
Verstraelen et al. BMC Infectious Diseases 2012, 12:148 http://www.biomedcentral.com/1471-2334/12/148 RESEARCH ARTICLE Open Access Antiseptics and disinfectants for the treatment of bacterial vaginosis: A systematic review Hans Verstraelen1*, Rita Verhelst2, Kristien Roelens1 and Marleen Temmerman1,2 Abstract Background: The study objective was to assess the available data on efficacy and tolerability of antiseptics and disinfectants in treating bacterial vaginosis (BV). Methods: A systematic search was conducted by consulting PubMed (1966-2010), CINAHL (1982-2010), IPA (1970- 2010), and the Cochrane CENTRAL databases. Clinical trials were searched for by the generic names of all antiseptics and disinfectants listed in the Anatomical Therapeutic Chemical (ATC) Classification System under the code D08A. Clinical trials were considered eligible if the efficacy of antiseptics and disinfectants in the treatment of BV was assessed in comparison to placebo or standard antibiotic treatment with metronidazole or clindamycin and if diagnosis of BV relied on standard criteria such as Amsel’s and Nugent’s criteria. Results: A total of 262 articles were found, of which 15 reports on clinical trials were assessed. Of these, four randomised controlled trials (RCTs) were withheld from analysis. Reasons for exclusion were primarily the lack of standard criteria to diagnose BV or to assess cure, and control treatment not involving placebo or standard antibiotic treatment. Risk of bias for the included studies was assessed with the Cochrane Collaboration’s tool for assessing risk of bias. Three studies showed non-inferiority of chlorhexidine and polyhexamethylene biguanide compared to metronidazole or clindamycin. One RCT found that a single vaginal douche with hydrogen peroxide was slightly, though significantly less effective than a single oral dose of metronidazole. -

Intraoperative Optical Coherence Tomography Imaging in Corneal Surgery: a Literature Review and Proposal of Novel Applications
Hindawi Journal of Ophthalmology Volume 2020, Article ID 1497089, 10 pages https://doi.org/10.1155/2020/1497089 Research Article Intraoperative Optical Coherence Tomography Imaging in Corneal Surgery: A Literature Review and Proposal of Novel Applications Hiroshi Eguchi ,1 Fumika Hotta,1 Shunji Kusaka,1 and Yoshikazu Shimomura2 1Department of Ophthalmology, Kindai University, Faculty of Medicine, 377-2 Ohnohigashi, Osakasayama, Osaka 589-8511, Japan 2Department of Ophthalmology, Fuchu Eye Center, 1-10-17 Hiko-cho, Izumi, Osaka 594-0076, Japan Correspondence should be addressed to Hiroshi Eguchi; [email protected] Received 26 June 2020; Revised 12 August 2020; Accepted 21 August 2020; Published 11 September 2020 Academic Editor: Sang Beom Han Copyright © 2020 Hiroshi Eguchi et al. &is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Intraoperative optical coherence tomography (iOCT) is widely used in ophthalmic surgeries for cross-sectional imaging of ocular tissues. &e greatest advantage of iOCTis its adjunct diagnostic efficacy, which facilitates to decision-making during surgery. Since the development of microscopic-integrated iOCT (MIOCT), it has been widely used mainly for vitreoretinal and anterior segment surgeries. In corneal transplantation, MIOCT allows surgeons to visualise structure underneath the turbid and distorted cornea, which are impossible to visualise with a usual microscope. Real-time visualisation of hard-to-see area reduces the operation time and leads to favorable surgical outcomes. &e use of MIOCT is advantageous for a variety of corneal surgical procedures. Here, we have reviewed articles focusing on the utility of iOCT and MIOCTin penetrating keratoplasty, deep anterior lamellar keratoplasty, Descemet stripping automated endothelial keratoplasty, and Descemet membrane endothelial keratoplasty. -

Pupillary Disorders LAURA J
13 Pupillary Disorders LAURA J. BALCER Pupillary disorders usually fall into one of three major cat- cortex generally do not affect pupillary size or reactivity. egories: (1) abnormally shaped pupils, (2) abnormal pupillary Efferent parasympathetic fibers, arising from the Edinger– reaction to light, or (3) unequally sized pupils (anisocoria). Westphal nucleus, exit the midbrain within the third nerve Occasionally pupillary abnormalities are isolated findings, (efferent arc). Within the subarachnoid portion of the third but in many cases they are manifestations of more serious nerve, pupillary fibers tend to run on the external surface, intracranial pathology. making them more vulnerable to compression or infiltration The pupillary examination is discussed in detail in and less susceptible to vascular insult. Within the anterior Chapter 2. Pupillary neuroanatomy and physiology are cavernous sinus, the third nerve divides into two portions. reviewed here, and then the various pupillary disorders, The pupillary fibers follow the inferior division into the orbit, grouped roughly into one of the three listed categories, are where they then synapse at the ciliary ganglion, which lies discussed. in the posterior part of the orbit between the optic nerve and lateral rectus muscle (Fig. 13.3). The ciliary ganglion issues postganglionic cholinergic short ciliary nerves, which Neuroanatomy and Physiology initially travel to the globe with the nerve to the inferior oblique muscle, then between the sclera and choroid, to The major functions of the pupil are to vary the quantity of innervate the ciliary body and iris sphincter muscle. Fibers light reaching the retina, to minimize the spherical aberra- to the ciliary body outnumber those to the iris sphincter tions of the peripheral cornea and lens, and to increase the muscle by 30 : 1. -

Living on Sunlight Publishing Copyright © 2004 All Rights Reserved
Compiled and Edited by Vina Parmar, MBA 2nd Edition Canticle of the Sun ÂcÜt|áx àÉ lÉâ? b _ÉÜw ÉâÜ ZÉw? yÉÜ tÄÄ lÉâÜ vÜxtàâÜxá? xáÑxv|tÄÄç ÉâÜ wxtÜ UÜÉà{xÜ fâÇ? j{É |á à{x wtç à{ÜÉâz{ ã{ÉÅ lÉâ z|äx âá Ä|z{àA Yt|Ü |á {x? |Ç áÑÄxÇwÉâÜ Ütw|tÇà? by lÉâ? `Éáà [|z{? {x uxtÜá à{x Ä|~xÇxáá‹Ê íft|Çà YÜtÇv|á Submitted by Stijn Cuypers This book is available as an e-book and as a hard copy. To order a copy, send an email to [email protected] 1st Edition November 2004 2nd Edition, December 2004 Living on Sunlight Publishing Copyright © 2004 All Rights Reserved 2 Table of Contents 1. Introduction, by Vina Parmar, MBA, Editor.......………………………...……….……...…4 2. Sun Gazing Benefits and Process, by Hira Ratan Manek: Living on Sunlight: Benefits and Background….………....................................6 About HRM ……………………………….……….…………………………..…….7 Sun Gazing: Process, History, Practice …………..……………………………10 3. How to Sun Gaze A Synopsis: Sun Gazing Instructions, by Sunny Jamshedji ……………………....16 Sun Charged Water ……………………………………………………………....17 Sun Bathing ………………………………………………………………………..17 What? Sun Gazing Essay and Poem by John Logan ……………………………18 4. Frequently Asked Questions Q & A Part I: from HRM’s original website …………………………………………..21 Q & A Part II: from www.lifemysteries.com website ................................................23 5. HRM’s Live Lectures and Interviews To hear HRM Live Online, Free ………..……………………………………..…41 Transcript # 1, Oct 2, 2004…………………………..……………………….…..42 Transcript # 2, Dec 1, 2002 ….. …………………………………………….…...51 HRM’s Interview with Jasmuheen ……………………………………………....58 6. Articles Published NASA …………………………………………………………………………........61 Living on Light ………………………………………….………………………….62 World Watch…………………………………………….………………………….64 Times of India……………………………………………………………………...65 Scientific Research Studies, Endocrinologist’s Report ……………………….68 7. -

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Ocular Photography - External (L34393)
Local Coverage Determination (LCD): Ocular Photography - External (L34393) Links in PDF documents are not guaranteed to work. To follow a web link, please use the MCD Website. Contractor Information Contractor Name Contract Type Contract Number Jurisdiction State(s) CGS Administrators, LLC MAC - Part A 15101 - MAC A J - 15 Kentucky CGS Administrators, LLC MAC - Part B 15102 - MAC B J - 15 Kentucky CGS Administrators, LLC MAC - Part A 15201 - MAC A J - 15 Ohio CGS Administrators, LLC MAC - Part B 15202 - MAC B J - 15 Ohio Back to Top LCD Information Document Information LCD ID Original Effective Date L34393 For services performed on or after 10/01/2015 Original ICD-9 LCD ID Revision Effective Date L31880 For services performed on or after 10/01/2018 Revision Ending Date LCD Title N/A Ocular Photography - External Retirement Date Proposed LCD in Comment Period N/A N/A Notice Period Start Date Source Proposed LCD N/A N/A Notice Period End Date AMA CPT / ADA CDT / AHA NUBC Copyright Statement N/A CPT only copyright 2002-2018 American Medical Association. All Rights Reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS/DFARS Apply to Government Use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for data contained or not contained herein. The Code on Dental Procedures and Nomenclature (Code) is published in Current Dental Terminology (CDT). -

Optum Essential Health Benefits Enhanced Formulary PDL January
PENICILLINS ketorolac tromethamineQL GENERIC mefenamic acid amoxicillin/clavulanate potassium nabumetone amoxicillin/clavulanate potassium ER naproxen January 2016 ampicillin naproxen sodium ampicillin sodium naproxen sodium CR ESSENTIAL HEALTH BENEFITS ampicillin-sulbactam naproxen sodium ER ENHANCED PREFERRED DRUG LIST nafcillin sodium naproxen DR The Optum Preferred Drug List is a guide identifying oxacillin sodium oxaprozin preferred brand-name medicines within select penicillin G potassium piroxicam therapeutic categories. The Preferred Drug List may piperacillin sodium/ tazobactam sulindac not include all drugs covered by your prescription sodium tolmetin sodium drug benefit. Generic medicines are available within many of the therapeutic categories listed, in addition piperacillin sodium/tazobactam Fenoprofen Calcium sodium to categories not listed, and should be considered Meclofenamate Sodium piperacillin/tazobactam as the first line of prescribing. Tolmetin Sodium Amoxicillin/Clavulanate Potassium LOW COST GENERIC PREFERRED For benefit coverage or restrictions please check indomethacin your benefit plan document(s). This listing is revised Augmentin meloxicam periodically as new drugs and new prescribing LOW COST GENERIC naproxen kit information becomes available. It is recommended amoxicillin that you bring this list of medications when you or a dicloxacillin sodium CARDIOVASCULAR covered family member sees a physician or other penicillin v potassium ACE-INHIBITORS healthcare provider. GENERIC QUINOLONES captopril ANTI-INFECTIVES -

Pattern of Vitreo-Retinal Diseases at the National Referral Hospital in Bhutan: a Retrospective, Hospital-Based Study Bhim B
Rai et al. BMC Ophthalmology (2020) 20:51 https://doi.org/10.1186/s12886-020-01335-x RESEARCH ARTICLE Open Access Pattern of vitreo-retinal diseases at the national referral hospital in Bhutan: a retrospective, hospital-based study Bhim B. Rai1,2* , Michael G. Morley3, Paul S. Bernstein4 and Ted Maddess1 Abstract Background: Knowing the pattern and presentation of the diseases is critical for management strategies. To inform eye-care policy we quantified the pattern of vitreo-retinal (VR) diseases presenting at the national referral hospital in Bhutan. Methods: We reviewed all new patients over three years from the retinal clinic of the Jigme Dorji Wangchuck National Referral Hospital. Demographic data, presenting complaints and duration, treatment history, associated systemic diseases, diagnostic procedures performed, and final diagnoses were quantified. Comparisons of the expected and observed frequency of gender used Chi-squared tests. We applied a sampling with replacement based bootstrap analysis (10,000 cycles) to estimate the population means and the standard errors of the means and standard error of the 10th, 25th, 50th, 75th and 90th percentiles of the ages of the males and females within 20-year cohorts. We then applied t-tests employing the estimated means and standard errors. The 2913 subjects insured that the bootstrap estimates were statistically conservative. Results: The 2913 new cases were aged 47.2 ± 21.8 years. 1544 (53.0%) were males. Housewives (953, 32.7%) and farmers (648, 22.2%) were the commonest occupations. Poor vision (41.9%), screening for diabetic and hypertensive retinopathy (13.1%), referral (9.7%), sudden vision loss (9.3%), and trauma (8.0%) were the commonest presenting symptoms. -
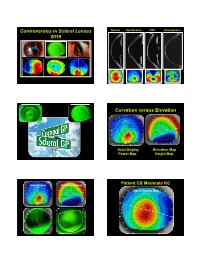
Controversies in Scleral Lenses 2019 Curvature Versus Elevation
Controversies in Scleral Lenses Normal Keratoconus PMD Keratoglobus 2019 Curvature versus Elevation Axial Display Elevation Map Power Map Height Map Axial Display Elevation Display Patient CB Moderate KC Axial Display Map +180um +180 +379 +379um Elevation Display -110 - 276 Elevation Map 655 Above the 290 microns Micron Sphere Height -276um Differential Depression Below the -110um Sphere N = 87 Patients 127 CL Fits Less than 350um Greater than 350um Patients with 350um or less of corneal elevation difference (along the greatest meridian of change) have an 88.2% chance of success with a corneal GP lens. The Re-Birth of Scleral Lenses Glass Scleral Lenses 1887 Molding Glass Scleral Lenses Average 8.5 High DK Scleral Materials Traditional Corneal / Scleral • Menicon Z Dk = 163 Shape • B & L, Boston XO2 DK = 141 • Contamac, Optimum Extreme DK = 125 • B & L, Boston XO DK = 100 • Paragon HDS 100 DK = 100 • Contamac, Optimum Extra DK = 100 • Lagado, Tyro -97 DK = 97 Scleral Shape Cone Angle Circa 1948 Klaus Pfortner New Understandings Argentina Scleral Lens Fitting Objectives Anatomy of a Scleral Lens 1. Central Vault Zone (250 to 400 microns) 2. Peripheral Lift Zone 4 3 2 1 2 3 4 3. Limbal Lift Zone 4. Scleral Landing Zone Ocular Surface Disease Scleral Lens Indications Scleral Irregular Astigmatism Lens • Keratoconus Indications • Pellucid Marginal Degeneration • Post Corneal Trauma • Post keratoplasty • Post K-Pro • Post Refractive Surgery RK, PRK and LASIK • Post HSV and HZV • Athletes • GP stability (rocking) issues Corneal Irregularity -

Olivia Steinberg ICO Primary Care/Ocular Disease Resident American Academy of Optometry Residents Day Submission
Olivia Steinberg ICO Primary Care/Ocular Disease Resident American Academy of Optometry Residents Day Submission The use of oral doxycycline and vitamin C in the management of acute corneal hydrops: a case comparison Abstract- We compare two patients presenting to clinic with an uncommon complication of keratoconus, acute corneal hydrops. Management of the patients differs. One heals quickly, while the other has a delayed course to resolution. I. Case A a. Demographics: 40 yo AAM b. Case History i. CC: red eye, tearing, decreased VA x 1 day OS ii. POHx: (+) keratoconus OU iii. PMHx: depression, anxiety, asthma iv. Meds: Albuterol, Ziprasidone v. Scleral CL wearer for approximately 6 months OU vi. Denies any pain OS, denies previous occurrence OU, no complaints OD c. Pertinent Findings i. VA cc (CL’s)- 20/25 OD, 20/200 PH 20/60+2 OS ii. Slit Lamp 1. Inferior corneal thinning and Fleisher ring OD, central scarring OD, 2+ diffuse microcystic edema OS, Descemet’s break OS (photos and anterior segment OCT) 2. 2+ diffuse injection OS 3. D&Q A/C OU iii. Intraocular Pressures: deferred OD due to CL, 9mmHg OS (tonopen) iv. Fundus Exam- unremarkable OU II. Case B a. Demographics: 39 yo AAM b. Case History i. CC: painful, red eye, tearing, decreased VA x 1 day OS ii. POHx: unremarkable iii. PMHx: hypertension iv. Meds: unknown HTN medication v. Wears Soflens toric CL’s OU; reports previous doctor had difficulty achieving proper fit OU; denies diagnosis of keratoconus OU vi. Denies any injury OS, denies previous occurrence OU, no complaints OD c. -

Frequency of Common Factors Leading to Leukocoria in Pediatric Age Group at Tertiary Care Eye Hospital: an Observational Study
Biostatistics and Biometrics Open Access Journal ISSN: 2573-2633 Research Article Biostat Biometrics Open Acc J Faisal’s Issue - January 2018 Copyright © All rights are reserved by Muhammad Faisal Fahim DOI: 10.19080/BBOAJ.2018.04.555636 Frequency of Common Factors Leading to Leukocoria in Pediatric Age Group at Tertiary Care Eye Hospital: An Observational Study Rizwana Dargahi1, Abdul Haleem1, Darikta Dargahi S1 and Muhammad Faisal Fahim2* 1Department of Ophthalmology, Shaheed Mohtarma Benazir Bhutto Medical University, Pakistan 2Department of Research & Development, Al-Ibrahim Eye Hospital, Pakistan Submission: November 27, 2017; Published: January 19, 2018 *Corresponding author: Muhammad Faisal Fahim, M.Sc. (Statistics), Statistician, Department of Research & Development, Al-Ibrahim Eye Hospital, Isra postgraduate Institute of Ophthalmology, Karachi, Pakistan, Tel: ; Email: Abstract Objective: To know the frequency of common factors leading to leukocoria in pediatric age group at a tertiary care eye hospital. Materials & methods: This was across sectional observational study carried out at Pediatric department, Al-Ibrahim eye hospital Karachi from February to July 2016. All patients younger than 10 years who presented with leukocoria were included. The excluding criteria were previous history of trauma and ocular surgery. Systemic as well as ocular examination and relevant investigations was done to know cause of was used to analyzed data. leukocoria. B. Scan was done in all the cases. If needed X-ray chest, CT scan & MRI orbit was done for confirming diagnosis. SPSS version 20.0 Results: In our country congenital cataract is the most common cause of leukocoria which comprises about 77.3% (133/172) which is treatable. 2nd common cause was persistent fetal vasculature comprises 8.1% (14/172). -

Reseptregisteret 2013–2017 the Norwegian Prescription Database
LEGEMIDDELSTATISTIKK 2018:2 Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Christian Berg Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Utgitt av Folkehelseinstituttet/Published by Norwegian Institute of Public Health Område for Helsedata og digitalisering Avdeling for Legemiddelstatistikk Juni 2018 Tittel/Title: Legemiddelstatistikk 2018:2 Reseptregisteret 2013–2017 / The Norwegian Prescription Database 2013–2017 Forfattere/Authors: Christian Berg, redaktør/editor Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Acknowledgement: Julie D. W. Johansen (English text) Bestilling/Order: Rapporten kan lastes ned som pdf på Folkehelseinstituttets nettsider: www.fhi.no The report can be downloaded from www.fhi.no Grafisk design omslag: Fete Typer Ombrekking: Houston911 Kontaktinformasjon/Contact information: Folkehelseinstituttet/Norwegian Institute of Public Health Postboks 222 Skøyen N-0213 Oslo Tel: +47 21 07 70 00 ISSN: 1890-9647 ISBN: 978-82-8082-926-9 Sitering/Citation: Berg, C (red), Reseptregisteret 2013–2017 [The Norwegian Prescription Database 2013–2017] Legemiddelstatistikk 2018:2, Oslo, Norge: Folkehelseinstituttet, 2018. Tidligere utgaver / Previous editions: 2008: Reseptregisteret 2004–2007 / The Norwegian Prescription Database 2004–2007 2009: Legemiddelstatistikk 2009:2: Reseptregisteret 2004–2008 / The Norwegian Prescription Database 2004–2008 2010: Legemiddelstatistikk 2010:2: Reseptregisteret 2005–2009. Tema: Vanedannende legemidler / The Norwegian Prescription Database 2005–2009.