Study Design and Baseline Profiles of Participants In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
USGS Open File Report 2007-1365
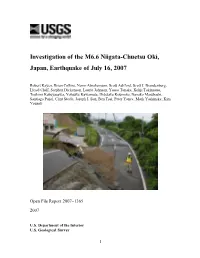
Investigation of the M6.6 Niigata-Chuetsu Oki, Japan, Earthquake of July 16, 2007 Robert Kayen, Brian Collins, Norm Abrahamson, Scott Ashford, Scott J. Brandenberg, Lloyd Cluff, Stephen Dickenson, Laurie Johnson, Yasuo Tanaka, Kohji Tokimatsu, Toshimi Kabeyasawa, Yohsuke Kawamata, Hidetaka Koumoto, Nanako Marubashi, Santiago Pujol, Clint Steele, Joseph I. Sun, Ben Tsai, Peter Yanev, Mark Yashinsky, Kim Yousok Open File Report 2007–1365 2007 U.S. Department of the Interior U.S. Geological Survey 1 U.S. Department of the Interior Dirk Kempthorne, Secretary U.S. Geological Survey Mark D. Myers, Director U.S. Geological Survey, Reston, Virginia 2007 For product and ordering information: World Wide Web: http://www.usgs.gov/pubprod Telephone: 1-888-ASK-USGS For more information on the USGS—the Federal source for science about the Earth, its natural and living resources, natural hazards, and the environment: World Wide Web: http://www.usgs.gov Telephone: 1-888-ASK-USGS Suggested citation: Kayen, R., Collins, B.D., Abrahamson, N., Ashford, S., Brandenberg, S.J., Cluff, L., Dickenson, S., Johnson, L., Kabeyasawa, T., Kawamata, Y., Koumoto, H., Marubashi, N., Pujol, S., Steele, C., Sun, J., Tanaka, Y., Tokimatsu, K., Tsai, B., Yanev, P., Yashinsky , M., and Yousok, K., 2007. Investigation of the M6.6 Niigata-Chuetsu Oki, Japan, Earthquake of July 16, 2007: U.S. Geological Survey, Open File Report 2007-1365, 230pg; [available on the World Wide Web at URL http://pubs.usgs.gov/of/2007/1365/]. Any use of trade, product, or firm names is for descriptive purposes only and does not imply endorsement by the U.S. -

Press Release
Press Release Press Release (This is provisional translation. Please refer to the original text written in Japanese.) October 22, 2020 Policy Planning Division for Environmental Health and Food Safety, Food Inspection and Safety Division, Pharmaceutical Safety and Environmental Health Bureau To Press and those who may concern, Cancellation of Instruction to restrict distribution based on the Act on Special Measures Concerning Nuclear Emergency Preparedness, direction of Director-General of the Nuclear Emergency Response Headquarters Today, based on the results of inspections conducted until yesterday, the Nuclear Emergency Response Headquarters has cancelled its Instruction of restriction of distribution for Governors of Ibaraki and Niigata as follows: (1)Bamboo shoot produced in Hokota-shi, Ibaraki prefecture. (2)Bear meat obtained after capturing in Tokamachi-shi and Joetsu-shi which are controlled under the policy for shipment and inspection set by Niigata prefecture. 1. With regard to Ibaraki prefecture, the restriction of distribution of Bamboo shoot produced in Hokota-shi is cancelled today. (1) The Instruction of the Nuclear Emergency Response Headquarters is attached as attachment 1. (2) The application of Ibaraki is attached as attachment 2. 2. With regard to Niigata prefecture, the restriction of distribution of Bear meat obtained after capturing in Tokamachi-shi and Joetsu-shi which are controlled under the management policy set by Niigata is cancelled today. (1) The Instruction of the Nuclear Emergency Response Headquarters is attached as attachment 3. (2) The application of Niigata is attached as attachment 4. 3. The list of Instructions on the restriction of distribution and/or consumption of food concerned in accordance with the Act on Special Measures Concerning Nuclear Emergency Preparedness is attached as reference. -
The Japanese School System
英語 2018 Edition The Japanese School System Going to High School Ⅰ The Structure of Japanese Schools 1 The Japanese Education System Age Graduate School 24 (2 or 5 years) Age 22 Age University (4 yrs.) Technical College (2 20 College (1-4 yrs.) yrs.) Specialized Age Vocational Special Late- High School (3 yrs.) 18 High School (5 Training Secondary Full-time (3 yrs.), Part-time or yrs.) High Education Correspondence High School (3-4 School (1-3 School (3 yrs.) yrs.) yrs.) Age Lower 15 Secondary Education Junior High School (3 yrs.) School (3 yrs.) Age Elementary School (6 yrs.) 12 Age 6 Preschool / Kindergarten (1) The 6・3・3・4 System The Japanese education system consists of a 6・3・3・4 system: 6 years of elementary school, 3 years of junior high school, 3 years of high school, and 4 years of university (or 2 years of college). (2) Compulsory Education Under the compulsory education system, all children are required to attend and graduate both elementary and junior high school. Although the compulsory education requirement applies only to Japanese nationals, non-Japanese children between the ages of 6-15 living in Japan are able to attend elementary and junior high school at the same cost as a Japanese child regardless of their nationality. Additionally, in 1994, Japan ratified the “Convention on the Rights of the Child” adopted by the UN General Assembly in 1989. This convention mandates that the right of all children to an education must be recognized. While Japan does not mandate that the guardians of non-Japanese children force their children to receive an education, children are guaranteed their right to one. -

Japanese Folk Tale
The Yanagita Kunio Guide to the Japanese Folk Tale Copublished with Asian Folklore Studies YANAGITA KUNIO (1875 -1962) The Yanagita Kunio Guide to the Japanese Folk Tale Translated and Edited by FANNY HAGIN MAYER INDIANA UNIVERSITY PRESS Bloomington This volume is a translation of Nihon mukashibanashi meii, compiled under the supervision of Yanagita Kunio and edited by Nihon Hoso Kyokai. Tokyo: Nihon Hoso Shuppan Kyokai, 1948. This book has been produced from camera-ready copy provided by ASIAN FOLKLORE STUDIES, Nanzan University, Nagoya, japan. © All rights reserved No part of this book may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying and recording, or by any information storage and retrieval system, without permission in writing from the publisher. The Association of American University Presses' Resolution on Permissions constitutes the only exception to this prohibition. Manufactured in the United States of America Library of Congress Cataloging-in-Publication Data Nihon mukashibanashi meii. English. The Yanagita Kunio guide to the japanese folk tale. "Translation of Nihon mukashibanashi meii, compiled under the supervision of Yanagita Kunio and edited by Nihon Hoso Kyokai." T.p. verso. "This book has been produced from camera-ready copy provided by Asian Folklore Studies, Nanzan University, Nagoya,japan."-T.p. verso. Bibliography: p. Includes index. 1. Tales-japan-History and criticism. I. Yanagita, Kunio, 1875-1962. II. Mayer, Fanny Hagin, 1899- III. Nihon Hoso Kyokai. IV. Title. GR340.N52213 1986 398.2'0952 85-45291 ISBN 0-253-36812-X 2 3 4 5 90 89 88 87 86 Contents Preface vii Translator's Notes xiv Acknowledgements xvii About Folk Tales by Yanagita Kunio xix PART ONE Folk Tales in Complete Form Chapter 1. -

Tourism As a Key for Regional Revitalization?: a Quantitative Evaluation of Tourism Zone Development in Japan
sustainability Article Tourism as a Key for Regional Revitalization?: A Quantitative Evaluation of Tourism Zone Development in Japan Hyunjung Kim 1 and Eun Jung Kim 2,* 1 Institute of Construction and Environmental Engineering, Seoul National University, Seoul 08826, Korea; [email protected] 2 Department of Urban Planning, Keimyung University, Daegu 42601, Korea * Correspondence: [email protected]; Tel.: +82-53-580-5247 Abstract: Since the dawn of the 21st century, Japan has switched its national industry strategy from traditional industries—manufacturing and trading—toward tourism. Regional revitalization is a particularly important issue in Japan, and by uniting regions as an integrated tourism zone, the government expects an increase in visits to tourism zones. This study quantitatively evaluates whether the regions that contain a tourism zone experience a significant increase in visitors by using a quasi-experimental pretest–posttest control group design. Additionally, it examines the effects of subsidies through regression modeling. The results indicated that the tourism zones that were comprised of a narrow region in the same prefectures experienced a significant increase in visitors. The subsidy on information transmission, measures for the secondary traffic, and space formation had a significant positive impact on the increase in visitors to these tourism zones. Implications on tourism policies, urban and regional development, and community development can be obtained through this study. Keywords: tourism zone development; regional revitalization; tourism nation; Japanese tourism Citation: Kim, H.; Kim, E.J. Tourism policy; tourism policy evaluation; pretest and posttest control group design as a Key for Regional Revitalization?: A Quantitative Evaluation of Tourism Zone Development in Japan. -

A Mediator Between Young People and Local Companies to Save Our Town
A Mediator Between Young People and Local Companies to Save Our Town 3103 Mimi Iwata Introduction A decline in population is one of the biggest problems in Japan, especially in the countryside. Minamiuonuma city, located in the southern part of Niigata prefecture, is greatly influenced by this phenomenon. It is inevitable for Minamiuonuma city to overcome this problem. In Minamiuonuma city, the number of young people is so few. The city hall has been carrying out some new policies that encourage young generation to come back, but they have not resulted well yet. So we need something new to address this problem. Problems The problem in Minamiuonuma city is the lack of young human resources. It leads to the decline in its industry and citizens will have difficulty living in, eventually. It will be difficult to improve the city’s overall industry. According to the survey of the Ministry of Internal Affairs and Communications (2017), the population of Minamiuonuma city decreased by 11.0% from 2000 to 2015. Seirou-machi, located in Niigata city, increased by 5.0%. Seirou-machi has the highest rate of increase in the population in Niigata prefecture. The population of 15 to 34 year-olds dexreased by 13% in Minamiuonuma city and has not so changed in Seirou-machi. It can be said that there is a big gap between Minamiuonuma city and Seirou-machi even if these two cities are located in the same prefecture. So we have to diminish the gap and solve the lack of young people. Solutions To solve this situation, I suggest introducing a UTA system, which stands for Uonuma Tactic Association. -

Preliminary Observations on the Niigata Ken Chuetsu, Japan, Earthquake of October 23, 2004
EERI Special Earthquake Report — January 2005 Learning from Earthquakes Preliminary Observations on the Niigata Ken Chuetsu, Japan, Earthquake of October 23, 2004 EERI organized a field investigation significant earthquake to affect Japan more than 100,000 people into tem- team led by Charles Scawthorn of since the 1995 Kobe earthquake. porary shelters, and as many as Kyoto University, which included Forty people were killed, almost 10,000 will be displaced from their Scott Ashford, University of Califor- 3,000 were injured, and numerous upland homes for several years, if nia San Diego; Jean-Pierre Bardet, landslides destroyed entire upland not permanently. Total damages are University of Southern California; villages. Landslides were of all types; estimated by Japanese authorities Charles Huyck, ImageCat Inc.; Rob- some dammed streams, creating at US$40 billion, making this the ert Kayen, U.S. Geological Survey; new lakes likely to overtop their new second most costly disaster in his- Scott Kieffer, Colorado School of embankments at any moment and tory, after the 1995 Kobe earth- Mines; Yohsuke Kawamata, Univer- cause flash floods and mudslides. quake. sity of California San Diego; and Landslides and permanent ground Rob Olshansky, University of Illinois, deformations damaged roads, rail The epicenter was in northwestern Urbana/Champaign and Visiting lines and other lifelines, resulting in Honshu, about 80 km south of Professor, Kyoto University. Paul major economic disruption. The nu- Niigata City (population 500,000), Somerville, URS Corporation, and merous landslides resulted, in part, well-known as the place liquefac- Jim Mori, Kyoto University, covered from heavy rain associated with tion was first systematically stud- the seismological aspects, but were Typhoon Tokage. -

Press Release
Press Release (Press Release (This is provisional translation. Please refer to the original text written in Japanese.) May 21, 2018 Policy Planning Division for Environmental Health and Food Safety, Food Inspection and Safety Division, Pharmaceutical Safety and Environmental Health Bureau To Press and those who may concern, Restriction of distribution based on the Act on Special Measures Concerning Nuclear Emergency Preparedness, direction of Director-General of the Nuclear Emergency Response Headquarters Today, based on the results of inspections conducted until yesterday, the Nuclear Emergency Response Headquarters has issued the Instruction of restriction of distribution of wild Koshiabura produced in Minamiuonuma-shi and Yuzawa-machi for Governor of Niigata. 1. With regard to Niigata prefecture, the restriction of distribution of wild Koshiabura produced in Minamiuonuma-shi and Yuzawa-machi is instructed today. (1) The Instruction of the Nuclear Emergency Response Headquarters is attached as attachment 1. (2) The application of Niigata is attached as attachment 2. 2. The list of Instructions on the restriction of distribution and/or consumption of food concerned in accordance with the Act on Special Measures Concerning Nuclear Emergency Preparedness is attached as reference. Reference: omitted Attachment 2: omitted (Attachment 1) Instruction 21 May, 2018 From Director-General of the Nuclear Emergency Response Headquarters To Governor of Niigata Prefecture, The Instruction to the Prefecture on 9 June, 2017, based on the Article 20.2 of the Act on Special Measures Concerning Nuclear Emergency Preparedness (Act No. 156, 1999) shall be changed as follows. 1. Restrictive requirements shall apply to heads of relevant municipalities and food business operators concerned not to distribute any bear meat obtained after capturing in Niigata prefecture (excluding Sado-shi and Awashimaura-mura) for the time being. -

Recent Damaging Earthquakes in Japan, 2003-2008
Missouri University of Science and Technology Scholars' Mine International Conference on Case Histories in (2008) - Sixth International Conference on Case Geotechnical Engineering Histories in Geotechnical Engineering 16 Aug 2008, 8:45am - 12:30pm Recent Damaging Earthquakes in Japan, 2003-2008 Robert Kayen U.S. Geological Survey, Menlo Park, CA Follow this and additional works at: https://scholarsmine.mst.edu/icchge Part of the Geotechnical Engineering Commons Recommended Citation Kayen, Robert, "Recent Damaging Earthquakes in Japan, 2003-2008" (2008). International Conference on Case Histories in Geotechnical Engineering. 21. https://scholarsmine.mst.edu/icchge/6icchge/session03/21 This Article - Conference proceedings is brought to you for free and open access by Scholars' Mine. It has been accepted for inclusion in International Conference on Case Histories in Geotechnical Engineering by an authorized administrator of Scholars' Mine. This work is protected by U. S. Copyright Law. Unauthorized use including reproduction for redistribution requires the permission of the copyright holder. For more information, please contact [email protected]. RECENT DAMAGING EARTHQUAKES IN JAPAN, 2003-2008 Robert Kayen, Ph.D. P.E. U.S. Geological Survey 345 Middlefield Road Menlo Park, CA 94025 USA ABSTRACT During the last six years, from 2003-2008, Japan has been struck by three significant and damaging earthquakes: The most recent M6.6 Niigata Chuetsu Oki earthquake of July 16, 2007 off the coast of Kashiwazaki City, Japan; The M6.6 Niigata Chuetsu earthquake of October 23, 2004, located in Niigata Prefecture in the central Uonuma Hills; and the M8.0 Tokachi Oki Earthquake of September 26, 2003 effecting southeastern Hokkaido Prefecture. -

Guide to Health Care & Hospitals 2017
Guide To Health Care & Hospitals 2017 医 療 案 内 General Information Page 1 1. National Health Insurance (NHI) 2. Things to Remember When You Visit Hospitals 3. Typical Visit to Hospitals 4. Medical Services Scheme in Uonuma Region Guide to Hospitals and Clinics 4 1. Yukiguni Yamato Hospital 4 2. Uonuma Kikan Hospital 10 3. Koide Hospital 14 4. Minami Uonuma City Hospital 15 5. Moegi Clinic 17 6. Other Clinics & Dentists 18 Maps to Hospitals and Clinics 19 1. Koide 2. Muikamachi 3. Sakura Clinic How to Seek Emergency Care 22 Additional Information 24 1. Compulsory Health Examination 2. Physical Health Support 3. Mental Health Support 4. Emergencies 5. Automated External Defibrillator (AED) 6. Multilingual Medical Questionnaire Sheet <Multilingual Medical Questionnaire> 25 <Language Assistance Sheet> 26 This guide is designed for use by students of the International University of Japan. < General Information > 1. National Health Insurance (NHI) The National Health Insurance (NHI) system in Japan is a “tax” system which reduces individuals’ medical cost and is called “Kokumin Kenko Hoken” in Japanese. All international students at IUJ must join this system. It is administered by the Minami Uonuma City Office. Please follow the procedure for NHI sign-up when you register your address with the City Office and be issued a health insurance card. 1.1. National Health Insurance Fee You have to pay the NHI fee after joining the NHI. It is a tax. The fee is discounted for students and will be approximately ¥18,000 for one year which is about 70% of the normal fee. -

Niigata Brewers Association
Tax Free Shop Kanto-Shinetsu Regional Taxation Bureau Tax Free Shop Brewery available for English website shop consumption tax telephone consumption tax tour English Brochure Location No. Breweries Mainbrand & liquor tax number As of December, 2017 ※ Please refer to SAKE Brewery when you visit it, because a reservation may be necessary. Niigata Brewers Association http://www.niigata-sake.or.jp/ ❶ Taiyo Sake Brewery Co., Ltd. TAIYOZAKARI 0254-53-3145 Yuzawa Shirataki Sake Brewery Jyozen Mizunogotoshi 025-784-3443 Murakami ❷ Miyao Sake Brewing CO., LTD. SHIMEHARITSURU 0254-52-5181 Uonumashuzou Kabushikikaisha TENJINBAYASHI 025-752-3017 Tokamachi ❸ Ichishima Sake Brewery Inc. ICHISHIMA 0254-22-2350 Matsunoishuzoujyou Corporation MATSUNOI 025-768-2047 KANEMASU SAKE CO., LTD 0254-22-3131 Naebashuzo Corporation NAEBASAN 025-765-2011 ❹ Brewery & Distillery KANEMASU Tsunan Shibata Tsunanjozo Corporation KIRINOTOH 025-765-5252 ❺ Kikusui Sake CO., LTD. KIKUSUI 0254-24-5111 KATOSHUZOU CO., LTD. KIYOMASA 025-548-3765 ❻ Fujinoishuzou Corporation FUJINOI 0254-41-3165 Kubiki Sake Brewery Co., Ltd. Koshijino Kobai 025-536-2329 Echigozakurashuzo Joetsu 0250-62-2033 ❼ Corporation ECHIGOZAKURA Koyamashuzouten Limited Partnership ECHIGOJIMAN 025-534-2022 Koshitsukanoshuzou Jouetsushuzou Corporation KOSHINOWAKATAKE 025-528-4011 Agano 0250-62-2011 ❽ Corporation KOSHINOAJIWAI Hakuryushuzou Sake- 0250-62-2222 Awashima ❾ brewing CO., LTD. HAKURYU Echigoshuzojo Corporation KOSHINOHAPPO 025-387-2008 ❿ Awashimaura Kita-ku ⓫ Echigodenemon Corporation DENEMON 025-388-5020 ⓬ DHC shuzo Co., Ltd. KOSHINOBAIRI 025-387-2025 ⓭ Imayo Tsukasa Corporation IMAYO TSUKASA 025-244-3010 Chuo-ku KOSHINOHANASHUZOU Murakami Niigata 025-241-2277 ⓮ Corporation KOSHINOHANA Sado Island Konan-ku ⓯ Ishimoto Sake Brewery CO., LTD. KOSHI NO KANBAI 025-276-2028 ●❷ ⓰ Shiokawa Sake Brewery Co., Ltd. -

Recent Damaging Earthquakes in Japan, 2003-2008
Missouri University of Science and Technology Scholars' Mine International Conference on Case Histories in (2008) - Sixth International Conference on Case Geotechnical Engineering Histories in Geotechnical Engineering 16 Aug 2008, 8:45am - 12:30pm Recent Damaging Earthquakes in Japan, 2003-2008 Robert Kayen U.S. Geological Survey, Menlo Park, CA Follow this and additional works at: https://scholarsmine.mst.edu/icchge Part of the Geotechnical Engineering Commons Recommended Citation Kayen, Robert, "Recent Damaging Earthquakes in Japan, 2003-2008" (2008). International Conference on Case Histories in Geotechnical Engineering. 21. https://scholarsmine.mst.edu/icchge/6icchge/session03/21 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 4.0 License. This Article - Conference proceedings is brought to you for free and open access by Scholars' Mine. It has been accepted for inclusion in International Conference on Case Histories in Geotechnical Engineering by an authorized administrator of Scholars' Mine. This work is protected by U. S. Copyright Law. Unauthorized use including reproduction for redistribution requires the permission of the copyright holder. For more information, please contact [email protected]. RECENT DAMAGING EARTHQUAKES IN JAPAN, 2003-2008 Robert Kayen, Ph.D. P.E. U.S. Geological Survey 345 Middlefield Road Menlo Park, CA 94025 USA ABSTRACT During the last six years, from 2003-2008, Japan has been struck by three significant and damaging earthquakes: The most recent M6.6 Niigata Chuetsu Oki earthquake of July 16, 2007 off the coast of Kashiwazaki City, Japan; The M6.6 Niigata Chuetsu earthquake of October 23, 2004, located in Niigata Prefecture in the central Uonuma Hills; and the M8.0 Tokachi Oki Earthquake of September 26, 2003 effecting southeastern Hokkaido Prefecture.