Ambulatory Care Sensitive Conditions in Portugal Page I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
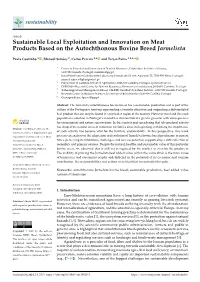
Sustainable Local Exploitation and Innovation on Meat Products Based on the Autochthonous Bovine Breed Jarmelista
sustainability Article Sustainable Local Exploitation and Innovation on Meat Products Based on the Autochthonous Bovine Breed Jarmelista Paula Coutinho 1 , Manuel Simões 2, Carlos Pereira 3,4 and Teresa Paiva 1,5,6,* 1 Center of Potential and Innovation of Natural Resources, Polytechnic Institute of Guarda, 6300-559 Guarda, Portugal; [email protected] 2 InnovPlantProtect Collaborative Laboratory, Estrada de Gil Vaz, Apartado 72, 7350-999 Elvas, Portugal; [email protected] 3 Polytechnic of Coimbra-School of Agriculture, 3045-601 Coimbra, Portugal; [email protected] 4 CERNAS—Research Centre for Natural Resources, Environment and Society, 3045-601 Coimbra, Portugal 5 Technological and Management School, CI&DEI, Guarda Polytechnic Institute, 6300-559 Guarda, Portugal 6 Research Center in Business Sciences, University of Beira Interior, 6200-609 Covilhã, Portugal * Correspondence: [email protected] Abstract: The Jarmelista autochthonous bovine breed has a sustainable production and is part of the culture of the Portuguese territory, representing a touristic attraction and originating a differentiated beef product that can only be found in a particular region of the country. However rural and livestock population evolution in Portugal’s inland has demonstrated a great regression with consequences for environment and nature conservation. In this context and considering that silvopastoral activity has shaped the natural areas of mountain territories since its beginning, rethinking the importance Citation: Coutinho, P.; Simões, M.; of such activity has become vital for the territory sustainability. In this perspective, this work Pereira, C.; Paiva, T. Sustainable Local Exploitation and Innovation on Meat presents an analysis of the adaptation and evolution of Jarmelista bovine breed production to current Products Based on the times, perceiving its limitations, challenges, and success potential, supported by a data collection of Autochthonous Bovine Breed secondary and primary sources. -

Millenium 83
CIÊNCIAS AGRÁRIAS, ALIMENTARES E VETERINÁRIAS AGRICULTURAL SCIENCES, FOOD AND VETERINARY CIENCIAS AGRÍCOLAS, ALIMENTOS Y VETERINARIA millenium 83 Millenium, 2(11), 83-90. en MORTALIDADE DE VITELOS FILHOS DE VACAS ALENTEJANAS E MERTOLENGAS NO DISTRITO DE PORTALEGRE MORTALITY OF CALVES BORN FROM ALENTEJANA AND MERTOLENGA COWS IN PORTALEGRE DISTRICT MORTALIDAD DE BECERROS NASCIDOS DE VACAS ALENTEJANAS Y MERTOLENGAS EN EL DISTRITO DE PORTALEGRE Rute Santos1,2 Luísa Pereira1 Miguel Minas1 Lina Costa1 Maria da Graça Carvalho1 Maria do Carmo Caetano3 José Neves4 1 Polytechnic Institute of Portalegre, Agrarian School of Elvas, Elvas, Portugal 2 VALORIZA - Research Centre for Enfogenous Resources Valorization, Portalegre, Portugal 3 General Directorate for Food and Veterinary, Regional Directorate for the Alentejo Region, Évora, Portugal 4 General Directorate for Food and Veterinary, Lisbon, Portugal Rute Santos - [email protected] | Luísa Pereira - [email protected] | Miguel Minas - [email protected] | Lina Costa - [email protected] | Maria da Graça Carvalho - [email protected] | Maria do Carmo Caetano - [email protected] | José Neves - [email protected] Corresponding Author RECEIVED: 12th October, 2019 Rute Santos ACCEPTED: 21th January, 2020 Escola Superior Agrária de Elvas Av. 14 de Janeiro, nº 21 7350-092 Portalegre [email protected] Santos, R., Pereira, L., Minas, M., Costa, L., Carvalho, M. G., Caetano, M. C., & Neves, J. (2020). Mortality of calves born from alentejana and mertolenga cows in Portalegre district. Millenium, 2(11), 83-90. 84 DOI: https://doi.org/10.29352/mill0211.09.00261 m11 RESUMO Introdução: Para além do seu impacto económico, a mortalidade dos vitelos é um indicador importante do bem-estar 7animal nas explorações de bovinos de carne. -

Weapons of the Weak in Portugal During the Early 20Th Century: the Example of the Central Alentejo1
Weapons of the Weak in Portugal during the Early 20th Century: The Example of the Central Alentejo1 Jesús-Ángel Redondo Cardeñoso2 Abstract This article explores James C. Scott’s concept of weapons of the weak, taking advantage of the possibilities of applying it to the social history of rural Portugal. Using the example of the Central Alentejo region during the early twentieth century, I analyze the characteristics of the most common types of daily resistance practiced by the lower classes in the region (such as stealing acorns and olives or poaching and livestock trespassing), specifically focusing on their social aspects as an act of resistance. To do this, I use newspaper reports and archive material from the district authorities as well as documentation on the cases tried at the Arraiolos District Court during the ten-year period between 1908 and 1918. Keywords Weapons of the Weak, Produce Theft, Poaching, Livestock Trespassing, Alentejo. Resumo No seguinte texto aprofundaremos no estudo do conceito armas dos fracos (weapons of the weak) de James C. Scott, para aproveitar as potenciais possibilidades da sua aplicação na história social rural portuguesa. Por meio do exemplo do Alentejo Central nos inícios do século XX, analisaremos as caraterísticas das práticas de resistência quotidiana mais comuns executadas pelas classes populares da região (furto de bolotas e azeitonas, caça furtiva e invasão de gados), e especificamente mostraremos o seu carater social e de resistência. Para isso, utilizaremos documentação jornalística e arquivística da administração distrital, assim como as causas judiciais do Tribunal de Comarca de Arraiolos durante a década de 1908 até 1918. -

Clustering Craftwork Activities: an Approach to Promote Regional Development in a Peripheral Region of Portugal
© Investigaciones Regionales. 19 – Páginas 97 a 116 Sección ARTÍCULOS Clustering craftwork activities: An approach to promote regional development in a peripheral region of Portugal Maria Manuela Natário *, Ascensão Braga **, Constantino Rei *** ABSTRACT: Portugal’s globalization and integration had positive repercussions at the economic and social development level, but simultaneously it evidenced regional asymmetries, demanding new explanatory models to lessen existent dis- parities. Recent paradigms value the endogenous characteristics of the territory that appear decisive of the country’s development, including the idea that regions and local agents should identify new kinds of production organization and relation- ships, thus enhancing clusters. Given that, in the Beira Interior Norte, craftwork activities assume a relative economic and social importance, the purpose of the present paper is to verify whether this sector acquires the cluster classification in the region and continuously characterized this classification while potential cluster promote and develop economic and social factors. JEL Classification: R11, R12. Keywords: regional development, clusters, craftwork activities. Clustering actividades artesanales: Un enfoque para promover el desarrollo regional en una región periférica de Portugal RESUMEN: La globalización y la integración de Portugal ha tenido repercusiones positivas en el nivel del desarrollo económico y social pero también han evidencia- do las asimetrías regionales, exigiendo nuevos modelos explicativos para disminuir las disparidades existentes. Los paradigmas recientes valoran las características endógenas del territorio como factores decisivos de su desarrollo. Las regiones y sus agentes locales deben identificar nuevas tipologías de organización y de rela- ción de la producción, de entre las que se destacan los clústers. Teniendo en cuenta * Instituto Politécnico da Guarda, Escola Superior de Tecnologia e Gestão. -

ESPON CPS 14 Scientific Report Annex XI Alentejo
Cross-border Public Services (CPS) Targeted Analysis Final Report Scientific Report – Annex XI Case study report – Alentejo-Extremadura- Andaluzia Version 14/01/2019 This targeted analysis is conducted within the framework of the ESPON 2020 Cooperation Programme, partly financed by the European Regional Development Fund. The ESPON EGTC is the Single Beneficiary of the ESPON 2020 Cooperation Programme. The Single Operation within the programme is implemented by the ESPON EGTC and co-financed by the European Regional Development Fund, the EU Member States and the Partner States, Iceland, Liechtenstein, Norway and Switzerland. This delivery does not necessarily reflect the opinions of members of the ESPON 2020 Monitoring Committee. Authors Costa, Nuno (IGOT-ULisboa) Marques da Costa, Eduarda (IGOT-ULisboa) Advisory Group ESPON EGTC Nicolas, Rossignol Acknowledgements J. Paulo Garrinhas by photo courtesy (June 2018) Photo cover page WORKSHOP 2 – Spatial Planning and Social Innovation in the territory CCDR Alentejo, Évora, 25/06/2018. Information on ESPON and its projects can be found on www.espon.eu. The web site provides the possibility to download and examine the most recent documents produced by finalised and ongoing ESPON projects. This delivery exists only in an electronic version. © ESPON, 2018 Printing, reproduction or quotation is authorised provided the source is acknowledged and a copy is forwarded to the ESPON EGTC in Luxembourg. Contact: [email protected] Cross-border Public Services (CPS) Final Report Scientific Report – Annex XI -
Wild 2020 – Annual Report
WILD 2020 ANNUAL REPORT i Contents Message from the board and team leader 3 Rewilding Portugal 4 What is rewilding? 5 Greater Côa Valley 6 Visiting the Greater Côa Valley 8 Wild Côa Network 10 When nature is part of entrepreneurship 12 Wildlife return 15 Increasing roe deer numbers 16 Reducing threats to wildlife 17 Coexistence corridors for the Iberian wolf 18 Livestock guarding dogs 19 Griffon vultures marked with GPS transmitters in the Côa Valley to study feeding habits 20 Communication 22 New documentary 23 Partnership with Guarda 2027 – European Capital of Culture 24 Media partnerships 25 Working closely with local communities 26 New environmental education program – Lupi EcoClubs 27 “Altano Rewilding” wine 28 Financials 2020 29 Who supports us 30 Supporting Rewilding Portugal’s work 32 2 JUAN CARLOS MUÑOZ REWILDING/ EUROPE JOÃO COSME Message from the board and team leader 2020 was a year that will go down in history. An proximity with the livestock breeders, in which unforgettable year due to the effects of the global solutions are found together and on a case-by- pandemic on social dynamics, changes in cul- case basis, with the ultimate goal of improving tural habits and the impact it had on our work. coexistence with this emblematic species. Rewilding Portugal had to adapt so that we could This work and many other actions that we keep the momentum we had gained in 2019, are developing were well documented in the when the organization was first established. first documentary produced within the scope It was immediately noticeable that the of the organization’s projects, “Rewilding, a new decrease in human activity on a global scale path for nature in Portugal”. -
Rally Guide Ii
RALLY GUIDE II BAJA PORTALEGRE 500 RALLY GUIDE II ÍNDEX Introduction & BAJA PORTALEGRE 500 Welcome 1 INTRODUCTION & WELCOME History 2 Dear friends, The Event 3 Past Winners 7 The Baja Portalegre 500 is back promising new emotions and great competition. Being the last event of the FIA Cross Country World Cup, as well as the last Organisation 10 round of the national off-road championship for cars and bikes, it will be decisive to define the national and Entities 11 international titles, which reinforces its international projection. AUTO Event 14 Downtown Portalegre will host, once again, the starting ceremony at the Tarro Garden, where we hope to host a great celebration to signal the start of the largest and oldest Portuguese off-road event. MOTO/ QUAD/SSV The layout is similar to that of previous years, with the traditional 5 km of the Prologue, which signals the start of the competition. Cars, Bikes, Quads Event 20 and SSV will face a further 85 km on SS2. The Mini Baja is also back, this time held in line, on a special stage, offering the younger ones Press 25 more competitiveness. We are, once more, grateful for the support of our sponsors – BP, Municipality Information & of Portalegre and Municipality of Ponte de Sor – as well as for the collaboration of the Municipalities of Abrantes, Alter do Chão, Crato, Tips 26 Fronteira, Gavião, Monforte, Nisa and Sousel, and the Community Councils of Chança, Comenda, Cunheira, Tolosa and Monte da Pedra, without which the Event would not be possible. The Region 30 We also count on the collaboration of the National Guard (GNR), the Fire Brigade of Portalegre District, as well as the support of Fonte Viva, Ibermedia, Environmental SNB, Fencaça, Portuguese Hunters Federation, RTP, and Rádio Portalegre. -

Loriga Is an Ancient, Beautiful and Historic Small Portuguese Town, Located in the Serra Da Estrela Mountains. Known As Lobriga
- 1 - Loriga is an ancient, beautiful and historic small portuguese town, located in the Serra da Estrela mountains. Known as Lobriga by the Lusitanians and Lorica by the Romans, it is more than 2600 years old. Notable people from Loriga include Viriathus ( known as Viriato in Portuguese ), a famous Lusitanian leader and portuguese national hero. Loriga as enormous touristics potentialities and they are the only ski resort and ski trails existing in Portugal ( Loriga is the Lusian Capital and the capital of the snow in Portugal ). Loriga is a small town in Portugal located in Guarda District. Loriga is 20 km away from the village of Seia, 40 km away from Viseu, 80 km away from Guarda and 320 km from Lisbon. It is nestled in the Serra da Estrela mountain range. It is known as the "Portuguese Switzerland" due to its landscape: a small town surrounded by mountains. Known to be settled by the Lusitanians, the town is more than 2600 years old and was part of the Roman province of Lusitania. It was known as Lobriga by the Lusitanians and Lorica by the Romans. Loriga became a textile manufacturing center in the begin-19th century. While that industry has since dissipated, today the town attracts a sizable tourist trade due to its picturesque scenery and vicinity to the Serra da Estrela Ski Resort, the only ski center in Portugal, totally inside the town limits. - 2 - Coordinates: 40°19'13.69?N 7°39'58.15?W? / ?40.3204694°N 7.6661528°W? / 40.3204694; -7.6661528 Loriga Civil Parish (Vila) The valley parish of Loriga in the shadow of the Serra -

National Report of Portugal
PORTUGAL Convention on the Conservation of Migratory Species of Wild Animals Format for reports of Parties on implementation of the Convention on the Conservation of Migratory Species of Wild Animals (revision of January 2002) Reporting format agreed by the Standing Committee at its 23 rd meeting (Bonn, December 2001) for voluntary use by Parties, on a trial basis, for reports submitted to COP7. Refer to separate instructions on completing the report. The questions below combine elements of Resolution 4.1 (Party Reports) adopted by the Fourth Meeting of the Conference of the Parties (Nairobi, June 1994) and Resolution 6.4 (Strategic Plan for the Convention on Migratory Species 2000-2005), adopted by the Sixth Meeting of the Conference of the Parties (Cape Town, November 1999), as well as commitments arising from other operational Resolutions and Recommendations of the Conference of the Parties. Which agency has been primarily responsible for the preparation of this report? INSTITUTO DA CONSERVAÇÃO DA NATUREZA, Ministry of Cities, Land Planning and Environment List any other agencies that have provided input: Department of Oceanography – University of Azores; Department of Biology, Marine Biology and Oceanography - University of Madeira; Madeira Natural Park; Whale Museum – Madeira I(a). General Information Please complete any unfilled boxes and amend and/or update as appropriate the information provided in the table below: Reports submitted: 1999 Period covered by this report: 2000 - 2001 Date of entry into force of the Convention in Portugal: 1 November 1983 Territory to which the Convention applies: Portugal and the Autonomous Regions of Madeira and of the Azores Reservations (against species listings): None Designated Focal Point: Appointment to the Scientific Council: Dr. -

Annual Report
WILD 2020 ANNUAL REPORT i Contents Message from the board and team leader 3 Rewilding Portugal 4 What is rewilding? 5 Greater Côa Valley 6 Visiting the Greater Côa Valley 8 Wild Côa Network 10 When nature is part of entrepreneurship 12 Wildlife return 15 Increasing roe deer numbers 16 Reducing threats to wildlife 17 Coexistence corridors for the Iberian wolf 18 Livestock guarding dogs 19 Griffon vultures marked with GPS transmitters in the Côa Valley to study feeding habits 20 Communication 22 New documentary 23 Partnership with Guarda 2027 – European Capital of Culture 24 Media partnerships 25 Working closely with local communities 26 New environmental education program – Lupi EcoClubs 27 “Altano Rewilding” wine 28 Financials 2020 29 Who supports us 30 Supporting Rewilding Portugal’s work 32 2 JUAN CARLOS MUÑOZ REWILDING/ EUROPE JOÃO COSME Message from the board and team leader 2020 was a year that will go down in history. An proximity with the livestock breeders, in which unforgettable year due to the effects of the global solutions are found together and on a case-by- pandemic on social dynamics, changes in cul- case basis, with the ultimate goal of improving tural habits and the impact it had on our work. coexistence with this emblematic species. Rewilding Portugal had to adapt so that we could This work and many other actions that we keep the momentum we had gained in 2019, are developing were well documented in the when the organization was first established. first documentary produced within the scope It was immediately noticeable that the of the organization’s projects, “Rewilding, a new decrease in human activity on a global scale path for nature in Portugal”. -

The Late Roman Villae of Horta Da Torre and Monte De São Francisco and Their Rural Context (North Alentejo, Portalegre District, Portugal)
THE LATE ROMAN VILLAE OF HORTA DA TORRE AND MONTE DE SÃO FRANCISCO AND THEIR RURAL CONTEXT (NORTH ALENTEJO, PORTALEGRE DISTRICT, PORTUGAL) Jesús García Sánchez Instituto de Arqueología, Mérida. CSIC-Junta de Extremadura André Carneiro Universidade de Évora Rogier A.A. Kalkers Sapienza Università di Roma Tesse D. Stek Royal Netherlands Institute in Rome RESUMEN / ABSTRACT Resumen: La investigación en las villae ilustra la con- Abstract: The development of large, Roman-style solidación del control administrativo y económico de villae have been seen as powerful illustrations of the territorios marginales y al mismo tiempo, presenta in- consolidation of Roman administrative and economic teresantes contextos para comprender el colapso del control, even in supposed backwater territories in far- control romano sobre el territorio y la aparición de flung areas of the Roman Empire. Their demise, realidades sociales alternativas. Desde 2018 hemos co- moreover, sheds light on the collapse of Roman con- menzado un nuevo de proyecto de investigación sobre trol and the appearance of new social realities. In this el desarrollo del Alto Alentejo desde la conquista ro- paper, we approach these research questions from the mana hasta el bajo imperio, en este caso presentamos point of view of a new landscape archaeology project algunas preguntas de investigación y resultados preli- launched in 2018, researching North Alentejo (Portu- minares relacionados con las villae de este último pe- gal) from the Roman conquest to the Late Roman Em- riodo. Nuestro trabajo comprende el uso de métodos pire. Our research, still work in progress, deploys no-invasivos como prospección artefactual, reconstruc- non-destructive methods such as archaeological sur- ción fotogramétrica del paisaje, prospección geofísica vey, landscape photogrammetric reconstruction, mediante georradar y también diversas campañas de ground penetrating radar (GPR) surveys and several excavación. -

Heritage Sites of Astronomy and Archaeoastronomy in the Context of the UNESCO World Heritage Convention
Heritage Sites of Astronomy and Archaeoastronomy in the context of the UNESCO World Heritage Convention Thematic Study, vol. 2 Clive Ruggles and Michel Cotte with contributions by Margaret Austin, Juan Belmonte, Nicolas Bourgeois, Amanda Chadburn, Danielle Fauque, Iván Ghezzi, Ian Glass, John Hearnshaw, Alison Loveridge, Cipriano Marín, Mikhail Marov, Harriet Nash, Malcolm Smith, Luís Tirapicos, Richard Wainscoat and Günther Wuchterl Edited by Clive Ruggles Published by Ocarina Books Ltd 27 Central Avenue, Bognor Regis, West Sussex, PO21 5HT, United Kingdom and International Council on Monuments and Sites Office: International Secretariat of ICOMOS, 49–51 rue de la Fédération, F–75015 Paris, France in conjunction with the International Astronomical Union IAU–UAI Secretariat, 98-bis Blvd Arago, F–75014 Paris, France Supported by Instituto de Investigaciones Arqueológicas (www.idarq.org), Peru MCC–Heritage, France Royal Astronomical Society, United Kingdom ISBN 978–0–9540867–6–3 (e-book) ISBN 978–2–918086–19–2 (e-book) © ICOMOS and the individual authors, 2017 All rights reserved A preliminary version of this publication was presented at a side-event during the 39th session of the UNESCO World Heritage Committee (39COM) in Bonn, Germany, in July 2015 Front cover photographs: Star-timing device at Al Fath, Oman. © Harriet Nash Pic du Midi Observatory, France. © Claude Etchelecou Chankillo, Peru. © Iván Ghezzi Starlight over the church of the Good Shepherd, Tekapo, New Zealand. © Fraser Gunn Table of contents Preface ......................................................................................................................................