Preserving Kidney Function When You Have Diabetes Steps to Prevent Kidney Damage Or Halt Its Progress
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Acute Kidney Injury: Challenges and Opportunities
Acute kidney injury: Challenges and opportunities Abstract: Community-acquired acute kidney injury (CA-AKI) can be a devastating diagnosis for any patient and can increase mortality during hospitalization. There can be long-term consequences for those who survive the initial insult. This article discusses CA-AKI and its implications for APRNs. By Nhan L.A. Dinh, MSN, CNP, AGACNP-BC, CCRN cute kidney injury (AKI) is a heterogeneous risk of CKD, but if clinicians do not recognize the kidney disorder that increases in-hospital diagnosis, they cannot follow up or intervene. An AKI A morbidity and mortality. In 2016 data, the diagnosis also increases the chance of another AKI incidence of AKI was 20% for Medicare patients with episode, with a 30% risk of a recurrent AKI episode both chronic kidney disease (CKD) and diabetes.1 Us- within 1 year.1 ing Veterans Affairs (VA) 2016 data, AKI occurred in Mortality is increased with an AKI episode. Medi- more than 25% of hospitalized veterans over age 22, care data from 2016 shows an in-hospital mortality of but less than 50% of those with lab-documented AKI 8.2% but this increases to over 13% when includ- were coded as such.1 The chief concern here is a missed ing patients who were discharged to hospice.1 The in- opportunity for intervention. AKI increases long-term hospital mortality for patients without AKI was only Keywords: acute kidney injury (AKI), Acute Kidney Injury Network (AKIN), chronic kidney disease (CKD), community-acquired acute kidney injury (CA-AKI), hospital-acquired acute kidney injury (HA-AKI), Kidney Disease Improving Global Outcomes (KDIGO), SvetaZi / Shutterstock Nephrotoxic Injury Negated by Just-in-time Action (NINJA), sick day rules 48 The Nurse Practitioner • Vol. -

Kidney, Renal Tubule – Dilation
Kidney, Renal Tubule – Dilation Figure Legend: Figure 1 Kidney, Renal tubule - Dilation in a male B6C3F1 mouse from a chronic study. Dilated tubules are noted as tracts running through the cortex and outer medulla. Figure 2 Kidney, Renal tubule - Dilation in a male F344/N rat from a chronic study. Tubule dilation is present throughout the outer stripe of the outer medulla, extending into the cortex. Figure 3 Kidney, Renal tubule - Dilation in a male B6C3F1 mouse from a chronic study. Slight tubule dilation is associated with degeneration and necrosis. Figure 4 Kidney, Renal tubule - Dilation in a male F344/N rat from a chronic study. Tubule dilation is associated with chronic progressive nephropathy. Comment: Renal tubule dilation may occur anywhere along the nephron or collecting duct system. It may occur in focal areas or as tracts running along the entire length of kidney sections (Figure 1). 1 Kidney, Renal Tubule – Dilation Renal tubule dilation may occur from xenobiotic administration, secondary mechanisms, or an unknown pathogenesis (see Kidney – Nephropathy, Obstructive (Figure 2). Dilation may result from direct toxic injury to the tubule epithelium interfering with absorption and secretion (Figure 3). It may also occur secondary to renal ischemia or from prolonged diuresis related to drug administration. Secondary mechanisms of tubule dilation may result from lower urinary tract obstruction, the deposition of tubule crystals, interstitial inflammation and/or fibrosis, and chronic progressive nephropathy (Figure 4). A few dilated tubules may be regarded as normal histologic variation. Recommendation: Renal tubule dilation should be diagnosed and given a severity grade. The location of tubule dilation should be included in the diagnosis as a site modifier. -

Hypertensive Kidney Disease Hypertensive Kidney
JAMA PATIENT PAGE The Journal of the American Medical Association KIDNEY DISEASE Hypertensive Kidney Disease ypertension (high blood pressure) causes problems for many organs in the body, including the kidneys. Kidney problems Hcaused by high blood pressure (hypertensive kidney disease) occur often in persons who have undetected, untreated, or poorly controlled hypertension. Kidney problems are also called renal dysfunction or renal failure. Certain groups of people, including African Americans and Native Americans, are more at risk for having hypertensive kidney disease. High blood pressure is the second leading cause of kidney failure, surpassed only by diabetes. African Americans are 6 times more likely than whites to have chronic renal failure related to high blood pressure. The November 20, 2002, issue of JAMA includes an article about high blood pressure and its effect on the kidneys. WHY IS HIGH BLOOD PRESSURE DANGEROUS? FOR MORE INFORMATION High blood pressure makes the heart work harder and can also damage the small blood • American Heart Association vessels in the body. These vessels are in all organs of the body, including the kidneys, the 800/242-8721 heart, and the brain. Damage to the arteries (blood vessels that carry blood to organs) www.americanheart.org results in insufficient blood flow to those organs and organ damage. In the kidney, this • National Institute of Diabetes & organ damage is called nephrosclerosis. The kidneys lose their ability to filter blood, Digestive & Kidney Diseases allowing buildup of substances that can be toxic to the body. Eventually the kidneys fail, www.niddk.nih.gov/health/kidney and dialysis (filtration of blood by a special machine) or a kidney transplant becomes /pubs/highblood/highblood.htm necessary to preserve the person’s life. -
The Urinary Tract and How It Works
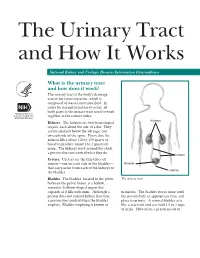
The Urinary Tract and How It Works National Kidney and Urologic Diseases Information Clearinghouse What is the urinary tract and how does it work? The urinary tract is the body’s drainage system for removing urine, which is composed of wastes and extra fluid. In order for normal urination to occur, all body parts in the urinary tract need to work together in the correct order. Kidneys Kidneys. The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine. Every day, the kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine. The kidneys work around the clock; a person does not control what they do. Ureters Ureters. Ureters are the thin tubes of muscle—one on each side of the bladder— Bladder that carry urine from each of the kidneys to Urethra the bladder. Bladder. The bladder, located in the pelvis The urinary tract between the pelvic bones, is a hollow, muscular, balloon-shaped organ that expands as it fills with urine. Although a urination. The bladder stores urine until person does not control kidney function, the person finds an appropriate time and a person does control when the bladder place to urinate. A normal bladder acts empties. Bladder emptying is known as like a reservoir and can hold 1.5 to 2 cups of urine. How often a person needs to urinate depends on how quickly the kidneys Why is the urinary tract produce the urine that fills the bladder. -

Claudins in the Renal Collecting Duct
International Journal of Molecular Sciences Review Claudins in the Renal Collecting Duct Janna Leiz 1,2 and Kai M. Schmidt-Ott 1,2,3,* 1 Department of Nephrology and Intensive Care Medicine, Charité-Universitätsmedizin Berlin, 12203 Berlin, Germany; [email protected] 2 Molecular and Translational Kidney Research, Max-Delbrück-Center for Molecular Medicine in the Helmholtz Association (MDC), 13125 Berlin, Germany 3 Berlin Institute of Health (BIH), 10178 Berlin, Germany * Correspondence: [email protected]; Tel.: +49-(0)30-450614671 Received: 22 October 2019; Accepted: 20 December 2019; Published: 28 December 2019 Abstract: The renal collecting duct fine-tunes urinary composition, and thereby, coordinates key physiological processes, such as volume/blood pressure regulation, electrolyte-free water reabsorption, and acid-base homeostasis. The collecting duct epithelium is comprised of a tight epithelial barrier resulting in a strict separation of intraluminal urine and the interstitium. Tight junctions are key players in enforcing this barrier and in regulating paracellular transport of solutes across the epithelium. The features of tight junctions across different epithelia are strongly determined by their molecular composition. Claudins are particularly important structural components of tight junctions because they confer barrier and transport properties. In the collecting duct, a specific set of claudins (Cldn-3, Cldn-4, Cldn-7, Cldn-8) is expressed, and each of these claudins has been implicated in mediating aspects of the specific properties of its tight junction. The functional disruption of individual claudins or of the overall barrier function results in defects of blood pressure and water homeostasis. In this concise review, we provide an overview of the current knowledge on the role of the collecting duct epithelial barrier and of claudins in collecting duct function and pathophysiology. -

Uremic Toxins Affect Erythropoiesis During the Course of Chronic
cells Review Uremic Toxins Affect Erythropoiesis during the Course of Chronic Kidney Disease: A Review Eya Hamza 1, Laurent Metzinger 1,* and Valérie Metzinger-Le Meuth 1,2 1 HEMATIM UR 4666, C.U.R.S, Université de Picardie Jules Verne, CEDEX 1, 80025 Amiens, France; [email protected] (E.H.); [email protected] (V.M.-L.M.) 2 INSERM UMRS 1148, Laboratory for Vascular Translational Science (LVTS), UFR SMBH, Université Sorbonne Paris Nord, CEDEX, 93017 Bobigny, France * Correspondence: [email protected]; Tel.: +33-2282-5356 Received: 17 July 2020; Accepted: 4 September 2020; Published: 6 September 2020 Abstract: Chronic kidney disease (CKD) is a global health problem characterized by progressive kidney failure due to uremic toxicity and the complications that arise from it. Anemia consecutive to CKD is one of its most common complications affecting nearly all patients with end-stage renal disease. Anemia is a potential cause of cardiovascular disease, faster deterioration of renal failure and mortality. Erythropoietin (produced by the kidney) and iron (provided from recycled senescent red cells) deficiencies are the main reasons that contribute to CKD-associated anemia. Indeed, accumulation of uremic toxins in blood impairs erythropoietin synthesis, compromising the growth and differentiation of red blood cells in the bone marrow, leading to a subsequent impairment of erythropoiesis. In this review, we mainly focus on the most representative uremic toxins and their effects on the molecular mechanisms underlying anemia of CKD that have been studied so far. Understanding molecular mechanisms leading to anemia due to uremic toxins could lead to the development of new treatments that will specifically target the pathophysiologic processes of anemia consecutive to CKD, such as the newly marketed erythropoiesis-stimulating agents. -

Pyelonephritis (Kidney Infection)
Pyelonephritis (Kidney Infection) Cathy E. Langston, DVM, DACVIM (Small Animal) BASIC INFORMATION urine collected from the bladder to be negative despite infection in the Description kidney. Abdominal x-rays and an ultrasound may be recommended. Bacterial infection of the kidney is termed pyelonephritis . Infection Although culture of a piece of kidney tissue obtained by biopsy may occur within kidney tissue or in the renal pelvis, the area of increases the chance of finding the infection, the invasiveness of the kidney where urine collects before being transported to the the procedure makes it too risky for general use (the biopsy would bladder. need to be taken from deeper within the kidney than the average Causes kidney biopsy). Contrast x-ray studies, such as an excretory uro- In most cases, a urinary tract infection starts in the bladder and gram (intravenous pyelogram), are sometimes helpful. An excre- the bacteria travel upstream to the kidney. Anything that decreases tory urogram involves taking a series of x-rays after a dye (that the free flow of urine, such as obstruction of the urethra (tube shows up white on x-rays) is given intravenously. Other tests may that carries urine from the bladder to the outside), bladder, ureter be recommended to rule out diseases that cause similar clinical (tube that carries urine from the kidney to the bladder), or kid- signs and other causes of kidney disease. ney, increases the risk that the infection will spread to the kid- ney. The presence of stones and growths in the bladder and kidney TREATMENT AND FOLLOW-UP also increases the risk. -
Urinalysis and Kidney Disease: What You Need to Know
URINALYSIS AND KIDNEY DISEASE What You Need To Know www.kidney.org About the Information in this Booklet Did you know that the National Kidney Foundation (NKF) offers guidelines and commentaries that help your healthcare provider make decisions about your medical treatment? The information in this booklet is based on those recommended guidelines. Stages of Kidney Disease There are five stages of kidney disease. They are shown in the table below. Your healthcare provider determines your stage of kidney disease based on the presence of kidney damage and your glomerular filtration rate (GFR), which is a measure of your kidney function. Your treatment is based on your stage of kidney disease. Speak to your healthcare provider if you have any questions about your stage of kidney disease or your treatment. STAGES OF KIDNEY DISEASE Glomerular Stage Description Filtration Rate (GFR)* Kidney damage (e.g., protein 1 90 or above in the urine) with normal GFR Kidney damage with mild 2 60 to 89 decrease in GFR 3 Moderate decrease in GFR 30 to 59 4 Severe reduction in GFR 15 to 29 5 Kidney failure Less than 15 *Your GFR number tells your healthcare provider how much kidney function you have. As chronic kidney disease progresses, your GFR number decreases. What is a urinalysis (also called a “urine test”)? A urinalysis is a simple test that looks at a small sample of your urine. It can help find conditions that may need treatment, including infections or kidney problems. It can also help find serious diseases in the early stages, like chronic kidney disease, diabetes, or liver disease. -

High Blood Pressure and Chronic Kidney Disease: for People
HIGH BLOOD PRESSURE AND CHRONIC KIDNEY DISEASE For People with CKD Stages 1–4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney Foundation's Kidney Disease Outcomes Quality Initiative (NKF-KDOQI™) has guidelines and commentaries that help your doctor and healthcare team make important decisions about your medical treatment? The information in this booklet is based on the NKF- KDOQI recommended guidelines and commentaries. What is your stage of kidney disease? There are five stages of kidney disease. They are shown in the table below. Your doctor determines your stage of kidney disease based on the presence of kidney damage and your glomerular filtration rate (GFR), which is a measure of your level of kidney function. Your treatment is based on your stage of kidney disease. Speak to your doctor if you have any questions about your stage of kidney disease or your treatment. STAGES of KidNEY DISEASE AGES of KidNEY DISEASE STAGES OF KIDNEY DISEASE Stage Description Glomerular Filtration Rate (GFR)* Kidney damage (e.g., protein 1 90 or above in the urine) with normal GFR Kidney damage with mild 2 60 to 89 decrease in GFR 3 Moderate decrease in GFR 30 to 59 4 Severe reduction in GFR 15 to 29 5 Kidney failure Less than 15 *Your GFR number tells your doctor how much kidney function you have. As chronic kidney disease progresses, your GFR number decreases. 2 NATIONAL KIDNEY FOUNDATION TABLE of ConTEntS Did you know? ...............................4 What is chronic kidney disease? ................5 What is high blood pressure? ...................6 How are high blood pressure and kidney disease related? ..............................6 How do I know if my blood pressure is too high? ..................................7 How is blood pressure measured? How often should it be checked? ...............8 I have high blood pressure but am not sure if I have CKD. -
Focal Segmental Glomerulosclerosis
some = Focal sections of = Segmental Focal Segmental kidney filters = Glomerulo FSGS Glomerulosclerosis = { are scarred Sclerosis How can research help? Research, which often requires patient participation, can lead to a better understanding of the causes, provide better diagnoses and more effective treatments, and ultimately help to find a cure. Be part of the discovery: By studying patients, researchers can more quickly unlock the mysteries of this disease. To get involved in research and stay informed, go to: Nephrotic Syndrome Study Network www.Nephrotic-Syndrome- NEPTUNE is a part of the NIH Rare Diseases Clinical Research Network (RDCRN). Funding and/or programmatic support for this project has been provided by U54 Studies.org DK083912 from the NIDDK and the NIH Office of Rare Diseases Research (ORDR), the NephCure Foundation and the University of Michigan. The views expressed in written materials of publications do not necessarily reflect the official policies of the or call 1-866-NephCure Department of Health and Human Services; nor does mention by trade names, commercial practices or organizations imply endorsement by the U.S. Government. What is Focal and Segmental Glomerulosclerosis? Symptoms, Diagnosis and Treatment Each person has Focal Segmental Glomerulosclerosis (FSGS) is a Your nephrologist may also recommend: two kidneys in rare disease that attacks the kidney’s filtering system • Diuretics and low salt diet help to control edema their lower back. (glomeruli) causing scarring of the filter. FSGS • A medication that blocks a hormone system called is one of the causes of a condition known as the renin angiotensin system (ACE inhibitor or ARB) Nephrotic Syndrome (NS). -

Chronic Kidney Disease (Ckd)
CHRONIC KIDNEY DISEASE ISSUE BRIEF prevent and control progressiveawareness obesity untreated end-stage renal disease kidney failure heart disease high blood pressure lifestyle changes stages complications family history damage to kidneys diabetes CKD few signs or symptoms PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) RISK FACTORS FOR CKD MAY INCLUDE ■ Heart Disease ■ Lupus ■ Diabetes ■ Family History of CKD ■ High Blood Pressure ■ Age ■ Obesity ■ High Cholesterol REDUCED INCREASED KIDNEY KIDNEY NORMAL KIDNEY RISK DAMAGE FUNCTION FAILURE Preventing CKD and its complications is possible by managing risk factors and treating the disease to slow its progression and reduce the risk of complications PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) What Is Chronic Kidney Disease? Fast Fact: Kidney diseases are the 9th leading cause of death in the United States. ■ Chronic kidney disease (CKD) is a condition in which a person has damaged kidneys or reduced kidney function for more than 3 months. During this time, the kidneys cannot properly filter waste out of the blood. If not detected and treated early, CKD can cause many health problems and even lead to kidney failure and early death. ■ CKD can start at any age, but the chances of developing it increase as people get older. It is most common among adults aged 70 years or older. ■ Once a person has CKD, it usually gets worse over time and lasts for the rest of the person’s life. Kidney failure—also called end-stage renal disease—is the final stage of CKD, when the kidneys stop working completely. How Big Is the CKD Problem and Who Is at Risk? Fast Fact: CDC estimates that more 6% than 20 million US adults aged 20 Unknown years or older have CKD—or more than 10% of the US adult population. -

Kidney Failure - Chronic in Dogs
Oak Knoll Animal Hospital 6315 Minnetonka Blvd, St. Louis Park, MN, 55416 Phone: 952-929-0074 Fax: 952-929-0110 Email: [email protected] Website: www.okah.net Kidney Failure - Chronic in Dogs What do my dog's kidneys do? The kidneys have many functions. They principally act to remove metabolic waste products from the blood stream, regulate the levels of certain essential nutrients such potassium and sodium, conserve water and produce urine. What does \"Chronic Renal Failure\" mean? Many people think that "chronic kidney failure" or "chronic renal failure" means that the kidneys have stopped working and are not making urine. Fortunately, this is not the case. By definition, chronic renal failure (CRF) is the inability of the kidneys to efficiently filter the blood of its physiological waste products, not the inability to produce urine. Ironically, most dogs in kidney failure produce large quantities of urine, but the body's toxic wastes are not being effectively eliminated. When do most cases of chronic kidney failure occur? Since kidney tissue cannot regenerate if destroyed, the kidneys have a large amount of spare capacity to perform their various functions. At least 2/3 of the kidneys must be dysfunctional before any clinical signs are seen. "Destruction has been occurring for months to years (chronic) before failure has become evident." In many cases, this means that the destruction has been occurring for months to years (chronic) before failure has become evident. In dogs, chronic kidney failure is associated with aging, and in simple terms can be considered to be "wearing out" of the kidney tissues.