Incidence and Prevalence of Malaria in Thrissur District, Kerala: a Time
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Local Governments-The Real Promotores of Women Empowerment
© 2019 IJRAR March 2019, Volume 6, Issue 1 www.ijrar.org (E-ISSN 2348-1269, P- ISSN 2349-5138) Local governments-The real promotores of women empowerment Dr. R. Ramya Assistant Professor of Economics Sri C. Achutha Menon Govt. College Thrissur 14 Abstract The empowerment of women gains a significant place in the developmental planning of every nation. There lays the significance of local governments who are the real promoters of women empowerment from the grass root level. How far the local governments are succeeded in helping women to empower socially, politically and economically is examined through an impact evaluation of schemes carried out in the Mattathur Panchayat in Thrissur district. Key Words: Women empowerment, local governments, pachayat, women component plan Introduction Empowerment, especially empowerment of women is very essential for the development of the family, society as well as nation. It is thus a process of enhancing the capacity of individuals or groups to make choices and to transform those choices into desired actions and outcomes. Empowerment in the real sense of the term increases the innate ability by way of acquiring knowledge, skill, power and experience. It helps individuals to think and act in an autonomous way. It involves developing confidence in their own capacities creating an enabling environment to use it productively to enhance the quality of their life. The main goal of women empowerment is to create a society with gender equality having equitable access to resources. Gender equality implies a society in which women and men enjoy the same opportunities, outcomes, rights and obligations in all spheres of life. -
List of Lacs with Local Body Segments (PDF
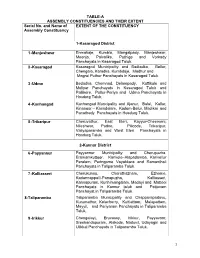
TABLE-A ASSEMBLY CONSTITUENCIES AND THEIR EXTENT Serial No. and Name of EXTENT OF THE CONSTITUENCY Assembly Constituency 1-Kasaragod District 1 -Manjeshwar Enmakaje, Kumbla, Mangalpady, Manjeshwar, Meenja, Paivalike, Puthige and Vorkady Panchayats in Kasaragod Taluk. 2 -Kasaragod Kasaragod Municipality and Badiadka, Bellur, Chengala, Karadka, Kumbdaje, Madhur and Mogral Puthur Panchayats in Kasaragod Taluk. 3 -Udma Bedadka, Chemnad, Delampady, Kuttikole and Muliyar Panchayats in Kasaragod Taluk and Pallikere, Pullur-Periya and Udma Panchayats in Hosdurg Taluk. 4 -Kanhangad Kanhangad Muncipality and Ajanur, Balal, Kallar, Kinanoor – Karindalam, Kodom-Belur, Madikai and Panathady Panchayats in Hosdurg Taluk. 5 -Trikaripur Cheruvathur, East Eleri, Kayyur-Cheemeni, Nileshwar, Padne, Pilicode, Trikaripur, Valiyaparamba and West Eleri Panchayats in Hosdurg Taluk. 2-Kannur District 6 -Payyannur Payyannur Municipality and Cherupuzha, Eramamkuttoor, Kankole–Alapadamba, Karivellur Peralam, Peringome Vayakkara and Ramanthali Panchayats in Taliparamba Taluk. 7 -Kalliasseri Cherukunnu, Cheruthazham, Ezhome, Kadannappalli-Panapuzha, Kalliasseri, Kannapuram, Kunhimangalam, Madayi and Mattool Panchayats in Kannur taluk and Pattuvam Panchayat in Taliparamba Taluk. 8-Taliparamba Taliparamba Municipality and Chapparapadavu, Kurumathur, Kolacherry, Kuttiattoor, Malapattam, Mayyil, and Pariyaram Panchayats in Taliparamba Taluk. 9 -Irikkur Chengalayi, Eruvassy, Irikkur, Payyavoor, Sreekandapuram, Alakode, Naduvil, Udayagiri and Ulikkal Panchayats in Taliparamba -
Newsletter Govt
04APR 2018 Newsletter Govt. Of Kerala Saras Mela 2018 kickstarted with a bang Organised by Kudumbashree Mission Saras Mela 2018, the national food and cultural expo, which would offer the best of traditional ethnic food and artistry was kickstarted at the ground near Market, Pattambi, Palakkad on 29 March 2018. Dr. K.T Jaleel, Minister, Local Self Government Department, Gov- ernment of Kerala inaugurated the programme. He also inaugurated the food stalls set up at the Mela. Saras Fair is not only a platform for the micro entre- preneurs to find market for their rural products, but also, this national festival is a platform which arrange the get together of the diverse yet secular culture of K our country. Minister said. Shri.Muhammad Muhsin, MLA, Pattambi presid- ed over the function. Shri. S.Harikishore, Executive Director, Kudumbashree presented the report. Shri. U Paloli Muhammed Kutty, Former Minister, LSGD was felicitated during the function. More than 4000 Kudumbashree women took part in D the procession organised prior to the inaugural func- tion. Micro entrepreneurs from 25 states across the country including Kerala are taking part in the pro- U gramme. Around 250 stalls are opened, out of which Kheer etc are the few of the foods offered by the dif- 100 stalls are of other states. The 70,000 sqft big pavil- ferent states. 45 tables and 315 chairs are set up at the ion and food court is the main attraction of the Mela. food court for serving the food. Gothra A sale of Rs 1 lakh was recorded on the inaugural day M The programme strictly follow the green protocol itself. -

Accused Persons Arrested in Thrissur Rural District from 29.11.2020To05.12.2020
Accused Persons arrested in Thrissur Rural district from 29.11.2020to05.12.2020 Name of Name of the Name of the Place at Date & Arresting Court at Sl. Name of the Age & Cr. No & Sec Police father of Address of Accused which Time of Officer, which No. Accused Sex of Law Station Accused Arrested Arrest Rank & accused Designation produced 1 2 3 4 5 6 7 8 9 10 11 29-11-2020 1050/2020 CHERPU UNNIKRISH MOHANDA 50, URAKATH HOUSE PERINCHER BAILED BY 1 APPU at 21:35 U/s 118(e) of (Thrissur NAN S Male , PERINCHERY RY POLICE Hrs KP Act Rural) SI OF POLICE 1281/2020 U/s 269, 270 IPC & 118(e) of KP Act & ANANDAKR MATHILAK POOVALIPARAMB 29-11-2020 Sec. 4(2)(f) ISHNAN SHAMSUDE 56, AM BAILED BY 2 ABDU IL HOUSE, AMANDOOR at 20:30 r/w 5 of ISHO EN Male (Thrissur POLICE PORIBAZAR Hrs Kerala MATHILAKA Rural) Epidemic M PS Diseases Ordinance 2020 THEKKOTTU 991/2020 U/s HOUSE, PARAMBI 29-11-2020 ALOOR SUKUMARA 35, PARAMBI 4(2)(e)(j)r/w SREEJITH.AK BAILED BY 3 ARUN ROAD DESAM, at 20:50 (Thrissur N Male ROAD 3(a) of KEDO SI OF POLICE POLICE THAZHEKKAD Hrs Rural) 2020 VILLAGE THEKKOTU 991/2020 U/s HOUSE,THAZHEK 29-11-2020 ALOOR 38, PARAMBI 4(2)(e)(j)r/w SREEJITH.AK BAILED BY 4 SAJI MOHANAN AD at 20:50 (Thrissur Male ROAD 3(a) of KEDO SI OF POLICE POLICE DESHAM,THAZHE Hrs Rural) 2020 KAD VILLAGE 1280/2020 U/s 269, 270 IPC & 118(e) RAMANKULATH of KP Act & MATHILAK HOUSE, EMMAD 29-11-2020 Sec. -

Accused Persons Arrested in Thrissur Rural District from 27.08.2017 to 02.09.2017
Accused Persons arrested in Thrissur Rural district from 27.08.2017 to 02.09.2017 Name of Name of the Name of the Place at Date & Arresting Court at Sl. Name of the Age & Cr. No & Sec Police father of Address of Accused which Time of Officer, which No. Accused Sex of Law Station Accused Arrested Arrest Rank & accused Designation produced 1 2 3 4 5 6 7 8 9 10 11 THEKOOT HOUSE CR.750/17 OLLURKKARA 27.08.201 A.S. 20/17 U/S 15 (C ) ATHIRAPPILL JFCM 1 VIBIN RAVI DESAM ATHIRAPPILLY 7 AT 13.00 SAJEEVAN MALE R/W 63 OF Y CHALAKUDY OLLURKKARA HRS SI OF POLICE ABKARI ACT VILLAGE M.K MAKKANDATHIL CR.531/17 27.08.201 PRABHAKARA JFCM 44/17 HOUSE, U/S 15 (C 0 ERUMAPETT 2 SURESH KURU VELLARAKKAD 7 AT 21.40 N WADAKKAN MALE VELLARAKKAD, R/W 63 OF Y HRS ADDL SI OF CHERY VELLATHERY ABKARI ACT POLICE M.K CR.531/17 KARAPPAMVEETTIL 27.08.201 PRABHAKARA JFCM 41/17 U/S 15 (C 0 ERUMAPETT 3 KABEER KAHADER HOUSE, AADHOOR, VELLARAKKAD 7 AT 21.40 N WADAKKAN MALE R/W 63 OF Y CHERANELLUR HRS ADDL SI OF CHERY ABKARI ACT POLICE ILAYEDATH CR.731/17 27.08.201 JFCM 21/17 HOUSE,EDAKULAM U/S 15 (C ) AJESH 4 SARATH SUDHI EDAKULAM 7 AT 21.31 KATTOOR IRINJALAKUD MALE DESAM,MANAVALA R/W 63 OF SI OF POLICE HRS A SSERY ABKARI ACT IDATHATTIL CR.731/17 27.08.201 JFCM 23/17 HOUSE,EDAKULAM U/S 15 (C ) AJESH 5 CHANAL CHANDRAN EDAKULAM 7 AT 21.31 KATTOOR IRINJALAKUD MALE DESAM,CHELOOR,M R/W 63 OF SI OF POLICE HRS A ANAVALASSERY ABKARI ACT MANGALAMPILLY CR.1578/17 27.08.201 JFCM MUHAMME 26/17 HOUSE EMMAD U/S 143 147 KODUNGALL JINESH 6 NISHAD KUNJAYANI 7 AT 14.45 KODUNGALL D MALE KOOLIMUTTAM -

TRICHUR BRANCH Ist Floor, Sakthan Arcade, TUDA Bldg, Near Sakthan Bus Stand, Trichur1
TRICHUR BRANCH Ist Floor, Sakthan Arcade, TUDA Bldg, Near Sakthan Bus Stand, Trichur1. Phone: 0487 2420330,2421590-e-mail:[email protected] Ref:TCR:665:880423:2019 06.08.2019 To Mr.Vibin K V, Mrs. Subhashini , S/o Vijayan Kamattathil, W/o Vijayan Kamattathil, Kamattathil House, Kamatttathil, Narayana Nagar, Narayana Nagar, Thhazhekad, Thazhekad, Kalletumkara P O, Kalletumkara P O, Thrissur District, Thrissur District, Kerala 680 683. Kerala 680 683 Dear Sir/Madam, Sub: Sale notice for sale of immovable property E-Auction Sale Notice for Sale of Immovable Assets under the Securitisation and Reconstruction of Financial Assets and Enforcement of Security Interest Act 2002 read with provision to Rule 8 (6) of Security Interest (Enforcement) Rules, 2002. Notice is hereby given to the public in general and in particular to the Borrower/s and Guarantor/s, that the below described immovable property mortgaged / charged to Secured Creditor, the physical possession of which has been taken by the Authorised Officer of Union Bank of India, Trichur Branch, Secured Creditor, will be sold on “AS IS WHERE IS”, “ AS IS WHAT IS”, “WHATEVER THERE IS” on 17.09.2019, for recovery of Rs. 41,65,524/- together with further interests & costs due to the Union Bank of India, Trichur, Secured Creditor from Mr.Vibin K V, S/o Vijayan Kamattathil, Kamattathil House, Narayana Nagar, Thazhekad, Kalletumkara P O, Thrissur District, Kerala 680 683 and Mrs. Subhashini , W/o Vijayan Kamattathil, Kamatttathil, Narayana Nagar, Thazhekad, Kalletumkara P O, Thrissur District, Kerala 680 683(borrowers). The reserve price will be Rs.29,00,000/- and earnest money deposit (EMD) will be Rs.2,90,000/- DESCRIPTION OF PROPERTY WITH KNOWN ENCURMBRANCES, IF ANY 3.64Ares of land and all improvements in Syno 1436/4 part of Mattathur Village in Chalakudy Taluk, Thrissur District obtained by Sale Deed No 1675/16 dated 09.09.2016 of SRO Kodaly in the name of Mr. -

Brief Industrial Profile of Thrissur District
1 Government of India Ministry of MSME Brief Industrial Profile of Thrissur District Carried out by MSME-Development Institute (Ministry of MSME, Govt. of India,), Thrissur Phone-0487-2360536, 2360638 Fax: 0487-2360216 e-mail: [email protected] Web-www.msmedithrissur.gov.in 2 Contents S. No. Topic Page No. 1. General Characteristics of the District 1 1.1 Location & Geographical Area 1 1.2 Topography 1 1.3 Availability of Minerals. 2 1.4 Forest 2 1.5 Administrative set up 3 2. District at a glance 3,4,5 2.1 Existing Status of Industrial Area in Thrissur District. 5 3. Industrial Scenario Of Thrissur District. 6 3.1 Industry at a Glance 6 3.2 Year Wise Trend Of Units Registered 7 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In The 8 District 3.4 Large Scale Industries / Public Sector undertakings 9 3.5 Major Exportable Item 9 3.6 Growth Trend 9 3.7 Vendorisation / Ancillarisation of the Industry 10 3.8 Medium Scale Enterprises 10 3.8.1 List of the units in Thrissur & near by Area 10 3.8.2 Major Exportable Item 10 3.9 Service Enterprises 10 3.9.1 Coaching Industry 10 3.9.2 Potentials areas for service industry 10 3.10 Potential for new MSMEs 10 4. Existing Clusters of Micro & Small Enterprise 10,11 4.1 Detail Of Major Clusters 11 4.1.1 Manufacturing Sector 11 4.1.2 Service Sector 11 4.2 Details of Identified cluster 11 4.2.1 -do- 11 4.2.2 -do- 11 4.2.3 -do- 12 4.2.4 -do- 12 4.2. -

Signature Not Verified
File No.DDP-TSR/4201/2020-E2 “ഭരണഭാഷ – മാതഭാഷഷ തശ്ശൂർ പഞ്ചായത്ത് ഡ蕆പ്യൂട്ടി 蕆യറക്ട앁ഡ絆 唾ാരയാഞ്ചയയ അയ്യനന്താൾ പി.ഒ, പിൻ- 680 003 നഫാൺ നമർ :0487 2360616 ഇ-ഡമയിൽ : [email protected] WEbsite: Https://dop.lsgkErala.gov.in/ നമർ. DDP-TSR/14201/2020-E2. തിയ്യതി : 29/06/2021 നനാട്ടീസ് വിഷയയ:- പഞ്ചായത്ത് വ啁പ്പ് - ജീവനകാരയയ - 2020 ഡപാ酁സ്ഥഞ്ചയ മാറയ - തശ്ശൂർ ജില്ലയിഡഞ്ച അനപക്ഷ唾셁ഡ絆 പ ട്ടി唾 അന്തിമമാകി bസി饍ീ唾രി啁നത് - സയബനിധിച്. ചന: - 1) ജി.ഒ.(പി) 3/2017/ഉഭപവ, തിയ്യതി. 25/02/2017. 2) ബഹ. പഞ്ചായത്ത് 蕆യറക്ട앁ഡ絆 21/12/2020 ഡഞ്ച PAN/14725/2020-E1(DP) നമർ നനാട്ടീസ്. 3) ഈ ഓഫീസിഡഞ്ച 26/02/2021 തിയ്യതിയിഡഞ്ച ഇനത നമർ നനാട്ടീസ്. ചന (1) b唾ാരയ സർകാർ പറഡപ്പപവിധിച സ്ഥഞ്ചയമാറ മാനദണ്ൾക് അനുതമായി പഞ്ചായത്ത് വ啁പ്പിഡഞ്ച വിവപ തസ്തി唾唾ലിഡഞ്ച 2021 ഡഞ്ച ഡപാ酁 സ്ഥഞ്ചയ മാറത്തിനത അനപക്ഷ ക്ഷണിച്ചുഡ唾ാണ്ട് ചന(2) b唾ാരയ ബഹ. പഞ്ചായത്ത് 蕆യറക്ടർ നനാട്ടീസ് bസി饍ീ唾രി啁唾യണ്ടായി. ആയ酁 b唾ാരയ ഡപാ酁 സ്ഥഞ്ചയ മാറത്തിനായി ഞ്ചഭിധിച അനപക്ഷ唾ൾ നകാ蕆ീ唾രിധിച് ജില്ലാ തഞ്ചത്തിൽ സ്ഥഞ്ചയ മാറയ ന絆നത്തണ്ട വിവപ തസ്തി唾唾ലിൽ സ്ഥഞ്ചയമാറയ ഞ്ചഭി啁നതിന് അനപക്ഷ സമർപ്പിധിച ജീവനകാ셁ഡ絆 唾ര絆് പട്ടി唾 ചന (3) b唾ാരയ bസി饍ീ唾രിധിച് ജീവനകാരിൽ നിനയ ആനക്ഷപ്ൾ സൾീ唾രി啁唾യണ്ടായി. അb唾ാരയ ഈ ഓഫീസിൽ ഞ്ചഭിധിച അനക്ഷപ്ങയ അഭിായ്ങയ പരിനാാപിധിച് ആയവ പരിഗണിധിചതിൻഡറ അ絆ിസ്ഥാനത്തിൽ ജില്ലയിൽ ഡപാ酁 സ്ഥഞ്ചയ മാറത്തിനത അനപക്ഷ唾셁ഡ絆 ചന (3) b唾ാരളത ഡപാ酁 സ്ഥഞ്ചയമാറ 唾ര絆് പട്ടി唾 പന:കമീ唾രിധിച് അന്തിമമാകി bസി饍ി唾രി啁ന. -

House Details Chalakudy Damage Type Complete Loss of Buildings
House Details_Chalakudy_Damage Type_Complete loss Of Buildings Ward House Sub Sl No Localbody Type Localbody Name Taluk Name Village Name Owner Name Owner Address Damage Type No No No 1 Grama Panchayat Alur 1 17 Chalakudy Kallettumkara sajeevan kocheri house,panjappilly,p.o kallettunkara Complete loss of Buildings Chakkedath(H) vellanchira po vellanchira, 2 Grama Panchayat Alur 9 187 Chalakudy Aloor Jaison chakko Complete loss of Buildings alur, Thrissur 680697 ILLIKKAL,THURUTHIPARAMBU 3 Grama Panchayat Alur 9 384 Chalakudy Aloor Rosy Antony VELLANCHIRA,ANNALLUR P Complete loss of Buildings O,Annallur,Thrissur,Kerala,680731 Nambiaruveettil House,Annallur P 4 Grama Panchayat Alur 10 132 Chalakudy Aloor N K VWLAYUDHAN O,Thiruthiparambu,Annallur,Thrissur,Kerala Complete loss of Buildings ,680731 5 Grama Panchayat Alur 10 22 A Chalakudy Aloor LALITHA Complete loss of Buildings Nayathodan House,Thiruthiparambu,Near 6 Grama Panchayat Alur 10 89 Chalakudy Aloor Kochamma Thiruthiparambu Church,Annalloor,po Complete loss of Buildings Vellanchira,Thrissur,Kerala,680697 7 Grama Panchayat Alur 11 157 Chalakudy Aloor Leela Koodoly house Karoor P O PIN 680697 Complete loss of Buildings Thooyath Vallakkunu Kallettumkara 8 Grama Panchayat Alur 23 441 Chalakudy Kallettumkara Sunil T.G Complete loss of Buildings Thrissur 680683 KATTEMKULAM KALLETTUMKARA P.O 9 Grama Panchayat Alur 23 621 Chalakudy Kallettumkara MINI SIVAN Complete loss of Buildings THRISSUR PIN:680683 10 Grama Panchayat Annamanada 1 71 Chalakudy Alathur Xavier T. T Themaliparambil house, -

Fairs and Festivals of Kerala-Statements, Part VII B (Ii
CENSUS OF INDIA 1961 VOLUME VII KERALA PART VII B (ii) FAIRS AND FESTIVALS OF KERALA-STATEMENTS M. K. DEVASSY~ B. A., B. L. OF TbE INDIAN ADMINISTRATIVE SERVICE Superintendent ql Census Operations, KeTola and the Union Territory of Laccadive, Minicoy and Amindivi Islands PUBLISHED BY THE MANAGER OF PUBLICATIONS. DELHI-8 PRINTED AT THB C. M. S. PRESS. KOTfAYAM 1968 PRICE: Delux.e Rs. 20.00 or 46 sh. 8 d. or $ 7.20 cents Ordinary Rs.8.75 or 20 sh. 5 d. or $ 3.15 cents PREFACE It is one of the unique features of the 1961 Cell3us that a comprehensive survey was conducted about the fairs and festivals of the country. Apart from the fact that it is the first systematic attempt as far as Kerala is concerned, its particular value lay in presenting a record of these rapidly vanishing cultural heritage. The Census report on fairs and festivals consists of two publications, Part VII B (i), Fairs and Festivals of Kerala containing the descriptive portion and Part VII B (ii), Fairs and Festivals of Kerala-Statements giving the tables relating to the fairs and festivals. The first part has already been published in 1966. It is the second part that is presented in this book. This publication is entirely a compilation of the statements furnished by various agencies like the Departments of Health Services, Police, Local Bodies, Revenue and the Devaswom Boards of Travancore and Cochin. This is something like a directory of fairs and festivals in the State arranged according to di'>tricts and taluks, which might excite the curiosity of the scholars who are interested in investigating the religiou, centres and festivals. -

Supply of Kadali Banana to Guruvayur Temple
Supply of Kadali Banana to Guruvayur Temple Kudumbashree District Mission of Thrissur had been supplying the Kadali Banana to the Devasom of Guruvayur, Kadali banana being the favorite offering to the deity of Guruvayur Temple. The bananas cultivated by the Kudumbashree women of Thrissur district in purely organic way are taken for poojas and are given away to the people as prasadam and are also used in preparing ‘panchamrutham’ (a sweet desert) as well. The JLGs in the district thereby got a permanent market for their cultivation. A total of 750 women from 150 Joint Liability Groups had been supplying 1.5 million of Kadali Banana to Guruvayur Temple every year. Kudumbashree District Mission of Thrissur had signed a Memorandum of Understanding (MoU) with the Guruvayur Devaswom regarding the same. The project had been a great success. The wise act of the District Mission had helped to find out a permanent market for the banana cultivated by JLGs in the district. Let’s see how the project works! Guruvayur Temple Guruvayur Sri Krishna Temple is a Hindu temple dedicated to the Hindu god Guruvayurappan (a four-armed affiliation of the Hindus god Vishnu), Kerala and is one of the most important places of worship which is located in the town of Guruvayur in Thrissur District in Kerala. It is believed by the followers that, Kadali Banana along with Yellow silk and lotus bud is the favorite offering of the deity. Kadali Banana Kadali is a small and sweet fruited variety of banana. The variety is mainly grown for offerings in temple. -

Farm Guide 2018
FARM GUIDE 2018 Printed & Published by V. SUMA PRINCIPAL INFORMATION OFFICER FARM INFORMATION BUREAU Kowdiar P.O., Thiruvananthapuram - 695 003 Fax. 0471 - 2318186 e-mail : [email protected]/ [email protected] Compiled and Edited by B. Neena Asst. Director (Technical Asst. IT Division), Dept. of Agriculture Dr. Suja Mary Koshy Editor, Farm News, Dept. of Animal Husbandry Dr. Geetha Ram Information Officer, Dept. of Animal Husbandry Dr. P. Selvakumar Campaign Officer, Dept. of Animal Husbandry Anitha C.S. Agricultural Officer, Dept. of Agriculture Vishnu S.P. Agricultural Officer, Dept. of Agriculture Publication Officer Elizabeth George Asst. Director, Dairy Development Dept. Design & Layout Deepak Mouthatil Articles for Kerala Karshakan: [email protected] 0471- 2314358 Press Release: [email protected] 0471- 2317314 Farm News & General Communication: [email protected] 0471- 2318186 Website: www.fibkerala.gov.in Im¿jnI hnI-k\ I¿jIt£a hIp∏v ktµiw tIcfsaßpw lcnX{]Xo£IfpW¿Øn ]pXph¿jw ho≠pw kamKXamhpIbmWv. Im¿jnItIcfØn\v A`nam\apb¿Øp∂ t\´ßƒ ssIhcn®psIm≠v kwÿm\k¿°mcpw Im¿jnIhnIk\ I¿jIt£a hIp∏pw kZv`cWØns‚ ]mXbn¬ apt∂dpIbmWv. A[nImcta‰v c≠ph¿jw ]q¿Ønbm°p∂ Cu thfbn¬ tZiobXeØn¬Øs∂ {it≤bamb \nch[n I¿jIt£a Im¿jnI˛]cnÿnXnkulrZ ]≤XnIƒ s]mXpP\ ]¶mfnØ tØmsS \n¿hln°m≥Ign™p F∂Xn¬ Gsd NmcnXm¿Yyhpw A`nam\hpap≠v. tIcfØns‚ {][m\ Im¿jnIhnfIfmb s\√pw sXßpw C∂v kwÿm\k¿°m¿ ]≤XnIfneqsS Xncn®phchns‚ ]mXbnemWv. CXns‚ `mKambn k¿°m¿ {]Jym]n® s\¬h¿jmNcWØn\v anI® {]XnIcWhpw ]n¥pWbpamWv e`n®Xv. CXns\ ]n¥pS¿∂v 1193 Nnßw H∂papX¬ 1194 Nnßw H∂phsc tIch¿jambn BNcn®v IrjnhIp∏v hnhn[]≤XnIƒ \S∏nem°pIbmWv.