Malpositions of the Occiput and Malpresentations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Diagnostic Impact of Limited, Screening Obstetric Ultrasound When Performed by Midwives in Rural Uganda
Journal of Perinatology (2014) 34, 508–512 © 2014 Nature America, Inc. All rights reserved 0743-8346/14 www.nature.com/jp ORIGINAL ARTICLE The diagnostic impact of limited, screening obstetric ultrasound when performed by midwives in rural Uganda JO Swanson1, MG Kawooya2, DL Swanson1, DS Hippe1, P Dungu-Matovu2 and R Nathan1 OBJECTIVE: To evaluate the diagnostic impact of limited obstetric ultrasound (US) in identifying high-risk pregnancies when used as a screening tool by midwives in rural Uganda. STUDY DESIGN: This was an institutional review board-approved prospective study of expecting mothers in rural Uganda who underwent clinical and US exams as part of their standard antenatal care visit in a local health center in the Isingiro district of Uganda. The midwives documented clinical impressions before performing a limited obstetric US on the same patient. The clinical findings were then compared with the subsequent US findings to determine the diagnostic impact. The midwives were US-naive before participating in the 6-week training course for limited obstetric US. RESULT: Midwife-performed screening obstetric US altered the clinical diagnosis in up to 12% clinical encounters. This diagnostic impact is less (6.7 to 7.4%) if the early third trimester diagnosis of malpresentation is excluded. The quality assurance review of midwives’ imaging demonstrated 100% sensitivity and specificity in the diagnosing gestational number, and 90% sensitivity and 96% specificity in the diagnosis of fetal presentation. CONCLUSION: Limited, screening obstetric US performed by midwives with focused, obstetric US training demonstrates the diagnostic impact for identifying conditions associated with high-risk pregnancies in 6.7 to 12% of patients screened. -

NUR 306- MIDWIWERY-II.Pdf
THE CATHOLIC UNIVERSITY OF EASTERN AFRICA P.O. Box 62157 A. M. E. C. E. A 00200 Nairobi - KENYA Telephone: 891601-6 Fax: 254-20-891084 MAIN EXAMINATION E-mail:[email protected] SEPTEMBER-DECEMBER 2020 TRIMESTER SCHOOL OF NURSING REGULAR PROGRAMME NUR/UNUR 306: MIDWIFERY II-LABOUR Date: DECEMBER2020 Duration: 3 Hours INSTRUCTIONS: i. All questions are compulsory ii. Indicate the answers in the answer booklet provided PART -I: MULTIPLE CHOICE QUESTIONS (MCQs) (20 MARKS): Q1.The following are two emergencies that can occur in third stage of labour: a) Cord prolapsed, foetal distress. b) Ruptured uterus ,foetal distress. c) Uterine inversion, cord pulled off. d) Cord round the neck, foetal distress. Q2 A woman in preterm labor at 30 weeks of gestation receives two 12-mg doses of betamethasone intramuscularly. The purpose of this pharmacologic treatment is to: a). Stimulate fetal surfactant production. b). Reduce maternal and fetal tachycardia associated with ritodrine administration. c). Suppress uterine contractions. d). Maintain adequate maternal respiratory effort and ventilation during magnesium sulfate therapy. Q3. Episiotomy should only be considered in case of : a) Breech, vacuum delivery, scarring from genital cutting, fetal distress. b) Primigravida, disturbed woman, genital cutting, obstructed labor. c) Obstructed labor, hypertonic contractions, multigravida, forceps delivery. Cuea/ACD/EXM/APRIL 2020/SCHOOL OF NURSING Page 1 ISO 9001:2015 Certified by the Kenya Bureau of Standards d) Primigravida, hypotonic contractions, fetal distress, genital cutting. Q4.A multiporous woman in labour tells the midwife “I feel like opening the bowels”.How should the midwife respond? a) Allow the woman to use the bedpan. -

Sexual Abuse of Elders Kearsley Home 1. Margaret Eckard
Sexual Abuse of Elders •Kathleen Brown •Associate Professor •University of Pennsylvania •School of Nursing Kearsley Home Retirement home for elderly women Located in West Philadelphia Gothic stone home over 200 years old 60 residents, ages 60-94 Security force on grounds Small in-patient unit; Highly trained staff 1. Margaret Eckard Popular, bubbly 92 year old resident One of longest residents at Kearsley January 23, 1983: missed at breakfast Nurse went to investigate; door ajar Body lying on floor next to rumpled bed Clad in nightgown; curled in fetal position Signs of rigor mortis starting to appear 1 Examination MD concerned over bruises on face; smears of blood around nose and mouth Streaks of blood in vagina and anus Decided not sufficiently disturbing to make an issue; decided natural death due to her age Funeral held 2. Katherine A. Maxwell 85 year old resident February 12, 1983: 21 inch snow storm Katherine failed to show for breakfast Door ajar; body lying on bed Pajamas spotted with blood Storm kept Dr. Webster from the Home Katherine Maxwell Body taken to hospital; no autopsy Blood believed to have occurred by natural causes at her death 2 3. Elizabeth Monroe Celebrated her 86th birthday with a party Next morning, failed to appear at breakfast Nurse found door ajar and her body in bed Face discolored; vaginal bleeding Dr. Webster away; substitute MD Sent body to undertaker Dr. Webster’s Concern Webster called the undertaker; suspicious over the 3 deaths ME’s office were not concerned over the 3 elderly victims’ deaths Webster insistent and ME accepted it for investigation but embalming made it difficult Ruled natural cause death 4. -

Delivery Mode for Prolonged, Obstructed Labour Resulting in Obstetric Fistula: a Etrr Ospective Review of 4396 Women in East and Central Africa
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by eCommons@AKU eCommons@AKU Obstetrics and Gynaecology, East Africa Medical College, East Africa 12-17-2019 Delivery mode for prolonged, obstructed labour resulting in obstetric fistula: a etrr ospective review of 4396 women in East and Central Africa C. J. Ngongo T. J. Raassen L. Lombard J van Roosmalen S. Weyers See next page for additional authors Follow this and additional works at: https://ecommons.aku.edu/eastafrica_fhs_mc_obstet_gynaecol Part of the Obstetrics and Gynecology Commons Authors C. J. Ngongo, T. J. Raassen, L. Lombard, J van Roosmalen, S. Weyers, and Marleen Temmerman DOI: 10.1111/1471-0528.16047 www.bjog.org Delivery mode for prolonged, obstructed labour resulting in obstetric fistula: a retrospective review of 4396 women in East and Central Africa CJ Ngongo,a TJIP Raassen,b L Lombard,c J van Roosmalen,d,e S Weyers,f M Temmermang,h a RTI International, Seattle, WA, USA b Nairobi, Kenya c Cape Town, South Africa d Athena Institute VU University Amsterdam, Amsterdam, The Netherlands e Leiden University Medical Centre, Leiden, The Netherlands f Department of Obstetrics and Gynaecology, Ghent University Hospital, Ghent, Belgium g Centre of Excellence in Women and Child Health, Aga Khan University, Nairobi, Kenya h Faculty of Medicine and Health Science, Ghent University, Ghent, Belgium Correspondence: CJ Ngongo, RTI International, 119 S Main Street, Suite 220, Seattle, WA 98104, USA. Email: [email protected] Accepted 3 December 2019. Objective To evaluate the mode of delivery and stillbirth rates increase occurred at the expense of assisted vaginal delivery over time among women with obstetric fistula. -

Rail Trespasser Fatalities Federal Railroad Administration Demographic and Behavioral Profiles
U.S. Department of Transportation Rail Trespasser Fatalities Federal Railroad Administration Demographic and Behavioral Profiles June 2013 NOTICE This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The U.S. Government assumes no liability for its contents or use thereof. Any opinions, findings and conclusions, or recommendations expressed in this material do not necessarily reflect the views or policies of the U.S. Government, nor does mention of trade names, commercial products or organizations imply endorsement by the U.S. Government. The U.S. Government assumes no liability for the content or use of the material contained in this document. NOTICE The U.S. Government does not endorse products or manufacturers. Trade or manufacturers’ names appear herein solely because they are considered essential to the objective of this report. NOTE: This report was prepared by North American Management (NAM) at the direction of the Federal Railroad Administration (FRA) for the purpose of more accurately identifying the types of persons who trespass on railroad rights-of-way, and ultimately reducing the number of trespassing casualties, which contribute significantly to the total annual railroad-related deaths and injuries in the United States. This report is an extension of a March 2008 report produced by Cadle Creek Consulting titled, “Rail Trespasser Fatalities, Developing Demographic Profiles” (2008 Report). The entire 2008 Report can be found at http://www.fra.dot.gov/eLib/Details/L02669. The current report was generated as part of FRA’s continuing efforts to reduce trespassing on railroad rights-of-way and associated fatalities and injuries. -

Breech Presentation at Delivery: a Marker for Congenital Anomaly?
Journal of Perinatology (2014) 34, 11–15 & 2014 Nature America, Inc. All rights reserved 0743-8346/14 www.nature.com/jp ORIGINAL ARTICLE Breech presentation at delivery: a marker for congenital anomaly? D Mostello1, JJ Chang2, F Bai2, J Wang3, C Guild4, K Stamps2 and TL Leet2,{ OBJECTIVE: To determine whether congenital anomalies are associated with breech presentation at the time of birth. STUDY DESIGN: A population-based, retrospective cohort study was conducted among 460 147 women with singleton live births using the Missouri Birth Defects Registry, which includes all defects diagnosed during the first year of life. Maternal and obstetric characteristics and outcomes between breech and cephalic presentation groups were compared using w2-square statistic and Student’s t-test. Multivariable binary logistic regression analysis was used to estimate adjusted odds ratios (aORs) and 95% confidence intervals (CIs). RESULT: At least one congenital anomaly was more likely present among infants breech at birth (11.7%) than in those with cephalic presentation (5.1%), whether full-term (9.4 vs 4.6%) or preterm (20.1 vs 11.6%). The relationship between breech presentation and congenital anomaly was stronger among full-term births (aOR 2.09, CI 1.96, 2.23, term vs 1.40, CI 1.26, 1.55, preterm), but not in all categories of anomalies. CONCLUSION: Breech presentation at delivery is a marker for the presence of congenital anomaly. Infants delivered breech deserve special scrutiny for the presence of malformation. Journal of Perinatology (2014) 34, 11–15; -

A Guide to Obstetrical Coding Production of This Document Is Made Possible by Financial Contributions from Health Canada and Provincial and Territorial Governments
ICD-10-CA | CCI A Guide to Obstetrical Coding Production of this document is made possible by financial contributions from Health Canada and provincial and territorial governments. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Unless otherwise indicated, this product uses data provided by Canada’s provinces and territories. All rights reserved. The contents of this publication may be reproduced unaltered, in whole or in part and by any means, solely for non-commercial purposes, provided that the Canadian Institute for Health Information is properly and fully acknowledged as the copyright owner. Any reproduction or use of this publication or its contents for any commercial purpose requires the prior written authorization of the Canadian Institute for Health Information. Reproduction or use that suggests endorsement by, or affiliation with, the Canadian Institute for Health Information is prohibited. For permission or information, please contact CIHI: Canadian Institute for Health Information 495 Richmond Road, Suite 600 Ottawa, Ontario K2A 4H6 Phone: 613-241-7860 Fax: 613-241-8120 www.cihi.ca [email protected] © 2018 Canadian Institute for Health Information Cette publication est aussi disponible en français sous le titre Guide de codification des données en obstétrique. Table of contents About CIHI ................................................................................................................................. 6 Chapter 1: Introduction .............................................................................................................. -

Twin Pregnancy with Triploidy and Co-Existing Live Twin Progressing to Viability: Case Study and Literature Review
Obstetrics & Gynecology International Journal Case Report Open Access Twin pregnancy with triploidy and co-existing live twin progressing to viability: Case study and literature review Abstract Volume 9 Issue 4 - 2018 Background: Twin pregnancies consisting of a triploid fetus with molar change and a 1,2 1,2 1,2 healthy coexisting fetus is an extremely rare phenomenon. Triploidy rarely advances to the Cingiloglu P, Yeung T, Sekar R second trimester, most resulting in a miscarriage, termination or stillbirth. Only five cases 1Royal Brisbane and Women’s Hospital, Women’s and Newborn of a triploid fetus and a healthy co-twin have been reported in literature. We present the first Services, Australia documented case of a live delivery of both triploid fetus and coexisting viable twin. 2University of Queensland, Australia Case presentation: A 23-year old woman, gravida 2, para 1 was admitted at 26+4 weeks Correspondence: Pinar Cingiloglu, Women’s and Newborn gestation with DCDA twins and a shortened cervix. Sonography revealed polyhydramnios, Services, Royal Brisbane and Women’s Hospital, Bowen Bridge an abnormal cystic placenta, and small aortic valve for the presenting twin. Emergency Road&, Butterfield St, Herston Queensland Australia, Tel +61 caesarean section was performed at 28 weeks gestation for cord prolapse. Twin A was born (07) 3646 8111, Email [email protected] a live infant with ambiguous genitalia, syndactyly, epicanthic folds and cerebral cysts. Twin B was born a healthy live male. Histopathology revealed features consistent with Received: June 13, 2018 | Published: July 13, 2018 partial hydatidiform mole, and cytogenetics revealed a diandric triploidy in twin A. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
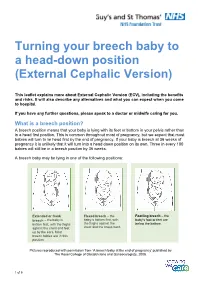
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Breech and Posterior Positions 19 Breech and Posterior Positions
Chapter 19 - Breech and posterior positions 19 Breech and posterior positions Western medical information t is expected that a baby will settle into a head down position within the pelvis around the 34th to 36th week of a pregnancy. The best position I for the baby to be in is termed a ‘well-flexed anterior position’, where the chin of the baby is tucked down towards its chest, its occiput has an anterior presentation into the pelvic outlet, and its spine is aligned outwards towards the mother’s abdomen. An anterior position can be either Left Occipital Anterior (LOA) or Right Occipital Anterior (ROA). In LOA the back of the baby’s head (the occiput) is lying to the left and slightly anterior within the mother’s pelvis. This means that the baby’s back will also be aligned at this angle with its spine facing outwards towards the mother’s abdomen. In ROA the occiput is to the right within the pelvis and the baby’s spine is angled towards the mother’s abdomen. Both are considered satisfactory positions for the baby to be in, although LOA is seen as the optimal position of the two. Left occipital anterior (LOA) Right occipital enterior (ROA) 128 Breech and posterior positions - Chapter 19 Unfortunately not all babies will actually be in the anterior position, and there may be either malposition or malpresentation of the foetus. Malposition In malposition, the baby’s head is the presenting part into the pelvic outlet, but it is not in the best position: either the occiput will be presenting as posterior, or the baby will have its head deflexed (in which case the head is hyperflexed instead of having the chin nicely tucked in). -

Chapter 9 Risk Factors
Chapter 9 Risk factors 9.1 Introduction The previous chapters have all focused on adverse pregnancy and birth outcomes as risk factors for foetal loss and neonatal death. The present chapter takes the discussion and analysis one layer further to the underlying risk factors for the selected adverse pregnancy and birth outcomes themselves. These risk factors are more remote in the causal chain and include maternal factors, complications of the placenta, cord, and membranes, and birth complications. These have been referred to earlier, in Chapter 3, in the operationalisation of the conceptual model (Figure 3.6). Besides their direct effect on pregnancy/birth outcome, they are believed to affect foetal loss (i.e. spontaneous abortion and stillbirth), both directly and indirectly, and neonatal death indirectly through the intermediate outcomes (i.e. adverse pregnancy and birth outcomes). As became clear in Chapter 3, many different causes and risk factors underlie the adverse pregnancy and birth outcomes, but what appear to be main risk factors? Are these risk factors also important in regions in transition and, more specifically, in Kerala? Moreover, does the relative importance of these risk factors change during the epidemiologic transition? A region’s position within the transition could very well be reflected by its specific combination of underlying risk factors. Factors such as infections and malnutrition are likely to be important during the early of the transition, while others such as diabetes and advanced maternal age may become more significant during later stages. This could lead to a redefinition of the concepts of endogenous and exogenous mortality (see Chapter 2). -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning.