Current Data and Strategy in Glioblastoma Multiforme
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PHYSICS and SOCIETY
PHYSICS and SOCIETY THE NEWSLETTER OF THE FORUM ON PHYSICS AND SOCIETY, PUBLISHED BY THE AMERICAN PHYSICAL SOCIETY, 335 EAST 45th ST., NEW YORK, NY 10017 PRINTED BY PENNY-SAVER, MANSFIELD, PA. 16933 Volume 10, Number 3, July, 1981 TABLE OF CONTENTS Synopsis of the April, 1981 Executive Committee Meeting........................................... 2 Report of the Forum Councillor, Mike Casper........................................................... 3 Committee on Opportunities in Physics, Earl Callen................................................... 3 Possible POPA Studies, George SeideL................................................................... 4 Report on Livermore Arms Control Conference, Charles Schwartz................................ 4 The Defense of the United States, review by John Dowling.......................................... 6 Arms Control Kit, John Dowling............................................................................ 7 PHYSICS AND SOCIETY is a quarterly newsletter of the Forum on Physics and Society. a division of the American Physical Society. The newsletter is distributed free to members of the Forum and also to physics libraries upon request. It presents news of the Forum and of the American Physical Society and provides a medium for Forum members to exchange ideas. PHYSICS AND SOCIETY also presents articles and letters on the scientific and economic health of the physics com munity; on the relations of physics and the physics community to government and to society, and the social responsiblities of scientists. Contributions should be sent to the Editor: John Dowling, Physics Department, Mansfield State College, Mansfield, PA 16933, 717-662-4275. Forum on Physics & Society BULK RATE Physics Department U.S. POSTAGE PAID Mansfield State College Mansfield, Pa. Permit No.3 Mansfield, PA 16933 Educational Non-Profit ARTI-'UR 7 QOSEN **** PHYSICS DEPARTMEkT CAL POLY STATE UkIVERSITY SAN LUIS OBISPO CA 93407 PHYSICS AND SOCIETY, Volume 10, Number 3 ••••••••••••••••••••••••• July 1981 Page 2 Synop.l. -

1 the Creation, Shipping, and Use of Radioactive Material Is Highly Regulated
Brooke Buddemeier, CHP Global Security Principal Directorate LLNLLLNL--PRESPRES--491531491531 1 This work performed under the auspices of the U.S. Department of Energy by Lawrence Livermore National Laboratory under Contract DE-AC52-07NA27344. The creation, shipping, and use of radioactive material is highly regulated (IAEA, NRC, DOT, et)tc.). High Activity Sources can only be produced by sophisticated methods (e.g. reactors & accelerators). High activity sources can only be obtained after special licensing to ensure their safe use and their security. Similar regulations exist in other countries were radioactive material is produced or used. 2 LLNLLLNL--PRESPRES--491531491531 Buddemeier 1 1 --1010 kiloCi 1 - 500 10 --100100 (when spent) kiloCi kiloCi Fuel Assembly (when spent) . Spent Nuclear Fuel & High Level Waste 0010.01 - 020.2 1-10 . Radioisotope Thermoelectric kiloCi kiloCi Generators (RTG) . Medical & Radiographic sources 3 LLNLLLNL--PRESPRES--491531491531 Buddemeier CDC Emergency Preparedness & Response Radionuclides Radionuclide Half Life Radiation Information (years) billions of Natural uranium is comprised of several different isotopes. Uranium α, When enriched in the isotope of U-235, it’s used to power years + progeny nuclear reactor or nuclear weapons. Am-241 is used for neutron generation (AmBe), in industrial Americium-241 430 y α devices that measure density and thickness, and in smoke dilldetectors in small amounts. Radionuclide thermoelectric generators and heat sources Plutonium-238 88 y α (primarily for space applications) Blood irradiators, tumor treatment through external Cesium-137 30.2 y β exposure. Also used for industrial radiography. Radionuclide thermoelectric generators, industrial gauges Strontium-90 29 y β and to treat bone tumors. -

Asia Treads the Nuclear Path, Unaware That Self- Assured Destruction Would Result from Nuclear War
The Journal of Asian Studies Vol. 76, No. 2 (May) 2017: 437–456. © The Association for Asian Studies, Inc., 2017 doi:10.1017/S0021911817000080 Asia Treads the Nuclear Path, Unaware That Self- Assured Destruction Would Result from Nuclear War OWEN B. TOON, ALAN ROBOCK, MICHAEL MILLS AND LILI XIA F THE NINE COUNTRIES known to have nuclear weapons, six are located in Asia and Oanother, the United States, borders the Pacific Ocean. Russia and China were the first Asian nations with nuclear weapons, followed by Israel, India, Pakistan, and North Korea. Most of the world’s nuclear powers are reducing their arsenals or maintaining them at historic levels, but several of those in Asia—India, Pakistan, and North Korea— continue to pursue relentless and expensive programs of nuclear weapons development and production. Hopefully, the nuclear agreement reached in July 2015 between Iran, the European Union, and the five permanent members of the United Nations Security Council will be a step toward eliminating nuclear weapons throughout Asia and the rest of the world. As we will discuss below, any country possessing a nuclear arsenal is on a path leading toward self-assured destruction, and is a threat to people everywhere on Earth. Nuclear-armed countries are a threat to people everywhere partly because of the destructive power of single weapons—one weapon is enough to destroy a small city— and partly because of the growing ability of nations to launch missiles across the globe. Nuclear powers such as India and North Korea, the latter of which is thought currently to have a very small nuclear capability that is not in the form of useful weapons, are working on the means to deliver weapons globally. -

NRC Collection of Abbreviations
I Nuclear Regulatory Commission c ElLc LI El LIL El, EEELIILE El ClV. El El, El1 ....... I -4 PI AVAILABILITY NOTICE Availability of Reference Materials Cited in NRC Publications Most documents cited in NRC publications will be available from one of the following sources: 1. The NRC Public Document Room, 2120 L Street, NW., Lower Level, Washington, DC 20555-0001 2. The Superintendent of Documents, U.S. Government Printing Office, P. 0. Box 37082, Washington, DC 20402-9328 3. The National Technical Information Service, Springfield, VA 22161-0002 Although the listing that follows represents the majority of documents cited in NRC publica- tions, it is not intended to be exhaustive. Referenced documents available for inspection and copying for a fee from the NRC Public Document Room include NRC correspondence and internal NRC memoranda; NRC bulletins, circulars, information notices, inspection and investigation notices; licensee event reports; vendor reports and correspondence; Commission papers; and applicant and licensee docu- ments and correspondence. The following documents in the NUREG series are available for purchase from the Government Printing Office: formal NRC staff and contractor reports, NRC-sponsored conference pro- ceedings, international agreement reports, grantee reports, and NRC booklets and bro- chures. Also available are regulatory guides, NRC regulations in the Code of Federal Regula- tions, and Nuclear Regulatory Commission Issuances. Documents available from the National Technical Information Service Include NUREG-series reports and technical reports prepared by other Federal agencies and reports prepared by the Atomic Energy Commission, forerunner agency to the Nuclear Regulatory Commission. Documents available from public and special technical libraries include all open literature items, such as books, journal articles, and transactions. -

PHYSICS and SOCIETY
PHYSICS and SOCIETY THE NEWSLETTER OF THE FORUM ON PHYSICS AND SOCIETY, PUBLISHED BY THE AMERICAN PHYSICAL SOCIETY, 335 EAST 45th ST., NEW YORK, NY 10017 PRINTED BY PENNY-SAVER, MANSFIELD, PA. 16933 Volume 10, Number 1 January, 1981 TABLE OF CONTENTS News of the Forum............................................................................................. 2 Update on the DeWitt Case.................................................................................. 2 Committee on Opportunities in Physics, Earl Callen.. ................................................. 2 Forum Sessions at the Annual APS-AAPT Meeting................................................... 3 Forum Sessions at the Phoenix APS Meeting............................................................ 5 $1,000,000,000,000 for Defense, Reviewed by John Dowling........................................ 5 Ground Zero, Leo Sartori..................................................................................... 6 Enlist New Forum Members............................... ....... ............................................ 8 PHYSICS AND SOCIETY is a quarterly newsletter of the Forum on Physics and Society. a division of the American Physical Society. The newsletter is distributed free to members of the Forum and also to physics libraries upon request. It presents news of the Forum and of the American Physical Society and provides a medium for Forum members to exchange ideas. PHYSICS AND SOCIETY also presents articles and letters on the scientific and economic health of the -

Antinuclear Politics, Atomic Culture, and Reagan Era Foreign Policy
Selling the Second Cold War: Antinuclear Cultural Activism and Reagan Era Foreign Policy A dissertation presented to the faculty of the College of Arts and Sciences of Ohio University In partial fulfillment of the requirements for the degree Doctor of Philosophy William M. Knoblauch March 2012 © 2012 William M. Knoblauch. All Rights Reserved. 2 This dissertation titled Selling the Second Cold War: Antinuclear Cultural Activism and Reagan Era Foreign Policy by WILLIAM M. KNOBLAUCH has been approved for the Department of History and the College of Arts and Sciences by __________________________________ Chester J. Pach Associate Professor of History __________________________________ Howard Dewald Dean, College of Arts and Sciences 3 ABSTRACT KNOBLAUCH, WILLIAM M., Ph.D., March 2012, History Selling the Second Cold War: Antinuclear Cultural Activism and Reagan Era Foreign Policy Director of Dissertation: Chester J. Pach This dissertation examines how 1980s antinuclear activists utilized popular culture to criticize the Reagan administration’s arms buildup. The 1970s and the era of détente marked a decade-long nadir for American antinuclear activism. Ronald Reagan’s rise to the presidency in 1981 helped to usher in the “Second Cold War,” a period of reignited Cold War animosities that rekindled atomic anxiety. As the arms race escalated, antinuclear activism surged. Alongside grassroots movements, such as the nuclear freeze campaign, a unique group of antinuclear activists—including publishers, authors, directors, musicians, scientists, and celebrities—challenged Reagan’s military buildup in American mass media and popular culture. These activists included Fate of the Earth author Jonathan Schell, Day After director Nicholas Meyer, and “nuclear winter” scientific-spokesperson Carl Sagan. -

Building MR-Simulation Competency in Radiotherapy
Radiation Oncology MRI Building MR-simulation competency in radiotherapy FieldStrength MRI magazine User experiences - November 2019 www.philips.com/mrinrt Starting from scratch, The Christie develops a MR-sim education and training program for proton beam radiotherapy service In the development of the National Health Services’ first high energy proton beam “The biggest problem in therapy (PBT) center at Manchester’s The Christie Hospital, acquisition of a dedicated ensuring the safe and MRI system for PBT planning was essential. MRI can provide exceptional soft tissue smooth implementation visualization for precise target and organs-at-risk (OAR) delineation for treatment planning and monitoring on-treatment variation – an imperative for safely delivering of an MR-sim service proton therapy. was a lack of knowledge, However, integrating MRI in a radiotherapy department presented a challenge – experience and training” radiotherapy personnel typically have little or no experience in safely and effectively operating in an MRI environment, while diagnostic radiographers have no or limited exposure to the needs of pre-treatment radiotherapy. To enable the safe, smooth implementation of an MR-sim Service, the Christie team developed and executed a training and education program for all PBT employees. The Christie NHS Foundation Trust The Christie NHS Foundation Trust in Manchester, UK, is the largest single site cancer centre in Europe, treating more than 44,000 patients a year. The centre has access to 15 linear accelerators and offers both proton beam therapy and MR-guided therapy. The Christie pre-treatment staff of the Proton Beam Therapy Center consists of: • One Diagnostic Band 7 Superintendent (MR Responsible Person) • Two Diagnostic Band 6 Senior Radiographers • Two Therapy Band 7 Superintendents • Two Therapy Band 6 Pre-treatment Radiographers Thomas Edwards is pre-treatment principal radiographer for protons at the Christie NHS Foundation Trust and has worked in radiotherapy for 16 years, specializing in radiotherapy imaging. -

Ground Zero Nagasaki Akitoshi Nakamura Akitoshi Nakamura Is the Director of the Nagasaki Atomic Bomb Museum
International Review of the Red Cross (2015), 97 (899), 543–552. The human cost of nuclear weapons doi:10.1017/S1816383116000084 VOICES AND PERSPECTIVES Photo gallery: Ground zero Nagasaki Akitoshi Nakamura Akitoshi Nakamura is the Director of the Nagasaki Atomic Bomb Museum. He has received a number of Japanese literary awards under the pen name Yuichi Seirai, including most notably the Akutagawa prize in 2001 for Holy Water, set in Nagasaki. Abstract This selection of photos is meant as an appeal from the Nagasaki Atomic Bomb Museum to remember the atomic bombing of Nagasaki on 9 August 1945. It was compiled by museum director Akitoshi Nakamura based on the collection at the Nagasaki Atomic Bomb Museum.1 Readers are invited to visit the Nagasaki Atomic Bomb Museum and spend some time viewing its collection of over 1,000 photographs and remnants from the city at that time to get a sense of what happened before and after the atomic bombing that summer seventy years ago, and how devastating the atomic bomb’s destructive effects were. Figures 1 and 2, below, show the area of the hypocentre in northern Nagasaki two days prior to the atomic bombing and about one month after the bombing. The meandering black line that cuts diagonally across each image from top to bottom is the Urakami River, which flows from the north to the south of the hypocentre. The oval near the centre is the track of an athletic field. In the second photo, one can see that the formerly varied cityscape of tightly-packed buildings has almost completely disappeared. -

Restricted Data Declassification Decisions 1946 to the Present (RDD 8)
OFFICIAL USE ONLY RESTRICTED DATA DECLASSIFICATION DECISIONS 1946 TO THE PRESENT (RDD-8) January 1, 2002 U.S. Department of Energy Office of Health, Safety and Security Office of Classification Contains information which may be exempt from public release under the Freedom of Information Act (5 U.S.C. 552), exemption number(s) 2. Approval by the Department of Energy prior to public release is required. Reviewed by: Richard J. Lyons Date: 3/20/2002 NOTICE This document provides historical perspective on the sequence of declassification actions performed by the Department of Energy and its predecessor agencies. It is meant to convey the amount and types of information declassified over the years. Although the language of the original declassification authorities is cited verbatim as much as possible to preserve the historical intent of the declassification, THIS DOCUMENT IS NOT TO BE USED AS THE BASIS FOR DECLASSIFYING DOCUMENTS AND MATERIALS without specific authorization from the Director, Information Classification and Control Policy. Classification guides designed for that specific purpose must be used. OFFICIAL USE ONLY OFFICIAL USE ONLY This page intentionally left blank OFFICIAL USE ONLY OFFICIAL USE ONLY FOREWORD This document supersedes Restricted Data Declassification Decisions - 1946 To The Present (RDD-7), January 1, 2001. This is the eighth edition of a document first published in June 1994. This latest edition includes editorial corrections to RDD-7, all declassification actions that have been made since the January 1, 2001, publication date of RDD-7 and any additional declassification actions which were subsequently discovered or confirmed. Note that the terms “declassification” or “declassification action,” as used in this document, refer to changes in classification policy which result in a specific fact or concept that was classified in the past being now unclassified. -

The Atomic Cafe
The Atomic Cafe By John Wills The documentary movie The Atomic Cafe Released on March 17, 1982, The Atomic relates the story of the American atomic Cafe met with largely positive reviews. bomb from its inception in 1945 through to Vincent Canby for the New York Times dominance over world affairs in the late applauded the “devastating collage film” 1950s. Consisting solely of archival for its exploration of atomic culture, and footage, filmmakers Jayne Loader, Kevin called it a picture “deserving national Rafferty and Pierce Rafferty craft a attention.” Richard Harrington for the convincing narrative of early Cold War Washington Post declared, “The Atomic events and attitudes. Their film provides a Cafe could be the most important film of critical glimpse into post-war America: a 1982,” and a “place from which to start world of Duck and Cover school drills, rethinking about the unthinkable.” 60 troops marching toward ground zero at the Minutes, Good Morning America and Nevada Test Site, and politicians waxing David Letterman all showed clips from the lyrical over both the threat and the movie. promise of a new atomic era. The film highlights the aesthetic spectacle, The release of the film proved timely. The abundant novelty and kitsch appropriation Atomic Cafe spoke to lingering of the bomb endemic to the period, but disillusionment with government stemming also reveals the drama, deceit and even from the Watergate scandal and the death associated with atomic Vietnam War. It aligned with the peak of experimentation. public distrust over national atomic policy. In the 1970s, renegade scientists such as An expansive US Government film John Gofman questioned the safety of the catalogue provided the initial inspiration American nuclear industry, and in 1979, a for Atomic Cafe. -
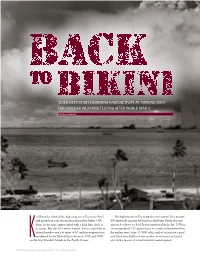
Scientists Study Lingering Radioactivity at 'Ground Zero'
SCIENTISTS STUDY LINGERING RADIOACTIVITY AT ‘GROUND ZERO’ FOR NUCLEAR WEAPONS TESTING AFTER WORLD WAR II by Evan Lubofsky en Buesseler climbed the highest peak on Enewetak Atoll The highest peak on Enewetak also isn't natural. It’s a massive and peered out over the expanse of paradise below. Off- 350-foot-wide concrete lid known as the Runit Dome that rises shore lay an azure lagoon inked with a dark-blue circle at just ten feet above sea level. It was constructed in the late 1970s as its center. But this hole wasn’t natural. It was created by an an attempt by the U.S. government to contain radioactivity from atomic bomb—one a of series of 67 nuclear weapons tests the nuclear tests. Some 111,000 cubic yards of radioactive topsoil conducted by the United States between 1946 and 1958 and debris were bulldozed into another bomb crater and sealed Kon the tiny Marshall Islands in the Pacific Ocean. over with a mosaic of several hundred concrete panels. 32 Oceanus Magazine Vol. 52, No. 2, Spring 2017 | www.whoi.edu/oceanus In July 1946, the U.S. military detonated a nuclear weapon 90 feet under water near Bikini Atoll. A geyser of radioactive water fell back into the lagoon, contaminating many nearby target ships. It was the second of 67 nuclear weapons tests inflicted on the Marshall Islands between 1946 and 1958. “It was a temporary fix,” said Buesseler, a marine chemist at “As an oceanographer who studies groundwater,” Charette Woods Hole Oceanographic Institution. As Buesseler stood atop said, “when I first saw the dome, I could immediately picture the dome with his WHOI colleague Matthew Charette, palm that it was filled with water beneath us, and with the rising and fronds rustled softly in the distance. -

Fallout from Nuclear Weapons Tests and Cancer Risks
A reprint from American Scientist the magazine of Sigma Xi, The Scientific Research Society This reprint is provided for personal and noncommercial use. For any other use, please send a request to Permissions, American Scientist, P.O. Box 13975, Research Triangle Park, NC, 27709, U.S.A., or by electronic mail to [email protected]. ©Sigma Xi, The Scientific Research Society and other rightsholders Fallout from Nuclear Weapons Tests and Cancer Risks Exposures 50 years ago still have health implications today that will continue into the future Steven L. Simon, André Bouville and Charles E. Land rior to 1950, only limited consider- weapons in the atmosphere. By the ear- explosive power of 440 megatons of Pation was given to the health im- ly 1960s, there was no place on Earth TNT (see Figure 2). pacts of worldwide dispersion of ra- where the signature of atmospheric The earliest concern about health ef- dioactivity from nuclear testing. But in nuclear testing could not be found in fects from exposure to fallout focused on the following decade, humanity began soil, water and even polar ice. possible genetic alterations among off- to significantly change the global ra- Cancer investigators who specialize in spring of the exposed. However, herita- diation environment by testing nuclear radiation effects have, over the interven- ble effects of radiation exposure have not ing decades, looked for another signature been observed from decades of follow-up of nuclear testing—an increase in cancer studies of populations exposed either to Steven L. Simon received a Ph.D. in radiological health rates. And although it is difficult to de- medical x rays or to the direct gamma ra- sciences from Colorado State University in 1985.