Sex and Contraception After Childbirth 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Role of a Midwife in Assisted Reproductive Units
Clinical Obstetrics, Gynecology and Reproductive Medicine Research Article ISSN: 2059-4828 The role of a midwife in assisted reproductive units O Tsonis1, F Gkrozou2*, V Siafaka3 and M Paschopoulos1 1Department of Obstetrics and Gynaecology, University Hospital of Ioannina, Greece 2Department of Obstetrics and Gynaecology, university Hospitals of Birmingham, UK 3Department of Speech and Language Therapy, School of Health Sciences, University of Ioannina, Greece Abstract Problem: The role of midwifery in Assisted Reproductive Units remains unclear. Background: Midwives are valuable health workers in every field or phase of women’s health. Their true value has been consistently demonstrated and regards mainly their function in labour. Infertility is a quite new territory in which a great deal of innovating approaches has been made through the years. Aim: The aim of this study is to present the role of midwifery in Assisted Reproductive Units based on scientific data Methods: For this review 3 (three) major search engines were included MEDLINE, PubMed and EMBASE focusing on the role of midwives in the assisted reproductive units. Findings: It seems that midwives have three distinct roles, when it comes to emotional management of the infertile couple, being the representative of the infertile couple and also, performing assisted reproductive techniques in some cases. Their psychomedical support is profound and, in this review, we try to research their potential role in the assisted reproductive units. Discussion: In the literature, only few scientific articles have been conducted in search of the role of Midwifery in Infertility. Their importance is once again undeniable and further research needs to be conducted in order to increase their adequate participation into this medical field. -

Experiences of Transition to Motherhood Among Pregnant Women Following Assisted Reproductive Technology: a Systematic Review Protocol of Qualitative Evidence
SYSTEMATIC REVIEW PROTOCOL Experiences of transition to motherhood among pregnant women following assisted reproductive technology: a systematic review protocol of qualitative evidence 1,2 1,2 1,2 1,2 1,2 Kunie Maehara Hiroko Iwata Mai Kosaka Kayoko Kimura Emi Mori 1Graduate School of Nursing, Chiba University, Chiba, Japan, 2The Chiba University Centre for Evidence Based Practice: a Joanna Briggs Institute Affiliated Group ABSTRACT Objective: This systematic review aims to identify and synthesize available qualitative evidence related to the experiences of transition to motherhood during pregnancy in women who conceived through assisted reproductive technology (ART). Introduction: Women who conceived through ART experience pregnancy-specific anxiety and paradoxical feelings, and face unique challenges in their identity transition to motherhood. It is important for healthcare professionals working with these women to understand the context and complexity of this special path to parenthood, including the emotional adaptation to pregnancy following ART. A qualitative systematic review can provide the best available evidence to inform development of nursing interventions to meet the needs of pregnant women after ART. Inclusion criteria: This review will consider any qualitative research data from empirical studies published from 1992–2019 in English or Japanese that described experiences of transition to motherhood during pregnancy in women who conceived with ART. Methods: This review will follow the JBI approach for qualitative systematic reviews. Databases that will be searched for published and unpublished studies include MEDLINE, CINAHL, PsycINFO, ProQuest Health & Medical Collection, Google Scholar and Open Access Theses and Dissertations (in English), and Ichushi-Web, CiNii and the Institutional Repositories Database (in Japanese). -

Unintended Pregnancy Prevention: Home
Home About CDC Press Room A-Z Index Contact Us CDC en Español Search: Unintended Pregnancy Prevention: Home Home Unintended Pregnancy Contraception Medical Eligibility An unintended pregnancy is a pregnancy that is either mistimed or Criteria unwanted at the time of conception. It is a core concept in understanding Female Sterilization the fertility of populations and the unmet need for contraception. Vasectomy Unintended pregnancy is associated with an increased risk of morbidity for women, and with health behaviors during pregnancy that are associated with adverse effects. For example, women with an unintended pregnancy may delay prenatal care, which may affect the health of the infant. Women of all ages may have unintended pregnancies, but some groups, such as teens, are at a higher risk. Reproductive Health In 2001, approximately one-half of pregnancies in the United States were Home unintended (Finer 2006, Perspectives on Sexual and Reproductive Data and Statistics Health), and the United States has set a national goal of decreasing Publications and unintended pregnancies to 30% by 2010. Products Glossary Efforts to decrease unintended pregnancy include finding better forms of contraception, and Related Links increasing contraceptive use and adherence. Research has also focused on better understanding pregnancy intention and how it is measured. As one study suggests, “A better understanding of the Adolescent Reproductive multiple dimensions of unintended pregnancy also may lead to a better understanding of the Health consequences of these pregnancies” (Santelli 2003, The Measurement and Meaning of Unintended Assisted Reproductive Pregnancy* ). Technology Global Reproductive Health Selected Resources Maternal and Infant Health Refugee Reproductive Adolescent Reproductive Health Health When teens give birth, their future prospects decline. -

The Factors Affecting Amniocentesis Decision by Pregnant Women in the Risk Group and the Influence of Consultant
A L J O A T U N R I N R A E L P Original Article P L E R A Perinatal Journal 2019;27(1):6–13 I N N R A U T A L J O ©2019 Perinatal Medicine Foundation The factors affecting amniocentesis decision by pregnant women in the risk group and the influence of consultant Kanay Yararbafl1 İD , Ayflegül Kuflkucu2 İD 1Department of Medical Genetics, Faculty of Medicine, Ac›badem Mehmet Ali Ayd›nlar University, Istanbul, Turkey 2Department of Medical Genetics, Faculty of Medicine, Yeditepe University, Istanbul, Turkey Abstract Özet: Risk grubundaki gebelerin amniyosentez karar› almas›ndaki faktörler ve genetik dan›flman›n etkisi Objective: The most frequent goal for prenatal diagnosis is to Amaç: Do¤um öncesi tan›da günümüzde en s›k amaçlanan hedef detect pregnancies with Down syndrome. Since karyotyping, which Down sendromlu gebelikleri tespit etmektir. Tan›da alt›n standart is the golden standard for the diagnosis, has not been replaced with yöntem olan karyotiplemenin yerini henüz non-invaziv bir yön- a non-invasive method, pregnant women in the risk group should tem dolduramad›¤›ndan, CVS, amniyosentez gibi bir yöntem için choose the method such as CVS and amniocentesis. Therefore, risk alt›ndaki gebelerin seçimi gereklidir. Bu amaçla giriflimsel ol- screening tests are performed by non-invasive method, and preg- mayan yöntemlerle tarama testleri yap›lmakta, riskli gebelere ge- nant women under risk are provided genetic consultation and the netik dan›flma verilerek invaziv giriflim karar› aileye b›rak›lmakta- family is expected to make a decision for invasive procedure. -

Statement on Unassisted Birth Attended by a Doula
Statement On Unassisted Birth Attended by a Doula _______________________________________________________ Definition Unassisted childbirth – the process of intentionally giving birth without the assistance of a medical or professional birth attendant – is a decision made by a very small percentage of parents. DONA International certified and member doulas provide physical, informational and emotional support. Any type of medical or clinical assistance is outside the scope of practice agreed upon by DONA International certified and member doulas. DONA International opines herein on the considerations a doula must make when accepting clients planning an unassisted birth. Introduction Unassisted childbirth (UC) refers to the process of intentionally giving birth without the assistance of a medical or professional birth attendant. UC is also sometimes referred to as free birth, DIY (do-it-yourself) birth, unhindered birth and couples birth. In response to the recent growth in interest over UC, several national medical societies, including the Society of Obstetricians and Gynaecologists of Canadai, the American College of Obstetricians and Gynecologistsii, and the Royal Australian and New Zealand College of Obstetricians and Gynaecologistsiii, have issued strongly worded public statements warning against the practice. Professional midwives' associations, including the Royal College of Midwivesiv and the American College of Nurse-Midwivesv also caution against UC. Those who promote UCvi claim the practice offers mothers-to-be a natural way of welcoming their child into the world, free from drugs, machinery and medical intervention. They also note that UC allows a woman to listen to her body's signals rather than coaching from an outsider. The women who are choosing UC may do so because they do not feel supported and respected in the obstetrical care facilities available in their areas, or they are unable to afford or obtain home midwifery or physician support, which is more in line with their philosophies. -

Midwifery: a Career for Men in Nursing
Midwifery: A career for men in nursing It may not be a common path men take, but how many male midwives are there? By Deanna Pilkenton, RN, CNM, MSN, and Mavis N. Schorn, RN, CNM, PHD(C) Every year, faculty at Vanderbilt University School of there are so few men in this profession. In fact, these Nursing reviews applications to the school’s nurse- conversations often lead to the unanimous sentiment midwifery program. The applicants’ diversity is always that men shouldn’t be in this specialty at all. Scanning of interest. A wide spectrum of age is common. A pleas- the web and reviewing blog discussions on this topic ant surprise has been the gradual improvement in the confirms that it’s a controversial idea, even among Eethnic and racial diversity of applicants. Nevertheless, midwives themselves. male applicants are still rare. It’s common knowledge that the profession of nurs- Many people wonder if there’s such thing as a male ing is female dominated, and the challenges and com- midwife. There are male midwives; there just aren’t plexities of this have been explored at length. many of them. When the subject of men in midwifery is Midwifery, however, may be one of the most exclusive- discussed, it usually conjures up perplexed looks. The ly and disproportionately female specialties in the field very idea of men in midwifery can create quite a stir, of nursing and it’s time to acknowledge the presence of and most laypeople don’t perceive it as strange that male midwives, the challenges they face, and the posi- www.meninnursingjournal.com February 2008 l Men in Nursing 29 tive attributes they bring to the pro- 1697, is credited with innovations fession. -
Fetal Heart Rate Monitoring This Document Should Be Read in Conjunction with the Disclaimer
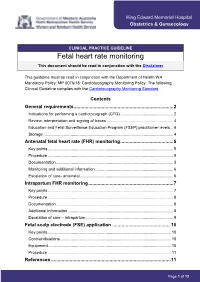
King Edward Memorial Hospital Obstetrics & Gynaecology CLINICAL PRACTICE GUIDELINE Fetal heart rate monitoring This document should be read in conjunction with the Disclaimer This guideline must be read in conjunction with the Department of Health WA Mandatory Policy: MP 0076/18: Cardiotocography Monitoring Policy. The following Clinical Guideline complies with the Cardiotocography Monitoring Standard. Contents General requirements ........................................................................... 2 Indications for performing a cardiotocograph (CTG) ............................................... 2 Review, interpretation and signing of traces ........................................................... 4 Education and Fetal Surveillance Education Program (FSEP) practitioner levels ... 4 Storage ................................................................................................................... 4 Antenatal fetal heart rate (FHR) monitoring ........................................ 5 Key points ............................................................................................................... 5 Procedure ............................................................................................................... 5 Documentation ........................................................................................................ 5 Monitoring and additional information ..................................................................... 6 Escalation of care- antenatal .................................................................................. -

1 Supplementary Table S2. Summary of the Results of Systematic Literature
Supplementary Table S2. Summary of the results of systematic literature review Question 1. What is the evidence that the following pre-conception (planned versus unintended pregnancy, disease activity and damage, antibody profile, lupus medications, management of flares, access to specialist services, immunization status and update) and post-conception/delivery (parenting issues, lupus medications, management of flares, access to specialist care) factors influence maternal and foetal outcomes, and thus, should be considered in pregnancy risk stratification and counselling in women with SLE or APS? 1. Women with SLE 1.1. Pre-conception factors associated maternal outcomes Factor/predictor Outcome(s) and example(s) of effect size Best study References design1 Active/flaring SLE (before Active/flaring SLE during pregnancy. SLE flares during the pre-gestation period had OR 4 1-21 or at conception) 5.1 for flare during pregnancy; previous (within 6 months before conception) organ involvement predicted same organ involvement during pregnancy (especially haematological, renal, skin, serological activity); SLE flares during the pre-gestation period had OR 5.1 for development of flare during pregnancy; SLEDAI ≥4 at conception had sensitivity 64% and specificity 75% for SLE exacerbation during pregnancy; remission during the 6-month period prior to conception is associated with lower odds for flare during pregnancy Organ damage. Pre-gestational SLE activity (SLAM-R index) correlates with post-partum 5 22 damage accrual Pregnancy-induced hypertension, (pre-)eclampsia/HELLP. Positive correlation with 4 12 14 21 23 pre-conception SLEDAI; active SLE within 4 months before conception was associated with pregnancy-induced hypertension (25% versus 11%) Adverse maternal outcome (composite outcome or death). -

Pregnancy Intention and Utilization of Maternal And
Jurnal Kesehatan Reproduksi, 9(1), 2018: 27-36 DOI: 10.22435/kespro.v9i1.891.27-36 PREGNANCY INTENTION AND UTILIZATION OF MATERNAL AND CHILD HEALTH CARE SERVICES IN INDONESIA Ika Saptarini1,2,*, Diahhadi Setyonaluri1 1Faculty of Economic and Business, University of Indonesia 2National Institute of Health Research and Development, Ministry of Health, Indonesia Submitted 31 May 2018; reviewed 3 June 2018; approved 30 June 2018 Abstrak Latar belakang: Antenatal care, persalinan oleh tenaga kesehatan, postnatal care serta imunisasi lengkap membantu meningkatkan kesehatan ibu dan anak. Tujuan: Penelitian ini bertujuan untuk mengetahui hubungan antara perencanaan kehamilan dan pemanfaatan pelayanan kesehatan ibu dan anak. Metode: Penelitian ini menggunakan data dari Survei Kesehatan Demografi Indonesia 2012. Empat model regresi digunakan untuk mengidentifikasi hubungan antara perencanaan kehamilan dan pemanfaatan pelayanan kesehatan ibu dan anak. Hasil: Lebih dari seperlima (25,5%) responden menerima kelima jenis perawatan ibu dan anak. Lima belas persen wanita melaporkan bahwa kehamilan terakhir mereka tidak diinginkan. Perencanaan kehamilan berhubungan secara bermakna dengan penggunaan antenatal care yang memadai (OR: 0,53, 95% CI, 0,46-0,60), pemanfaatan antenatal care dan persalinan oleh tenaga kesehatan (OR: 0,62, 95% CI, 0,55-0,71), pemanfaatan antenatal care, persalinan oleh tenaga kesehatan dan postnatal care ( OR: 0,82, 95% CI, 0,72-0,93), namun tidak berhubungan secara signifikan dengan pemanfaatan antenatal care, persalinan oleh tenaga kesehatan, postnatal care hingga imunisasi lengkap (OR: 1,06, 95% CI, 0,91-1,22) setelah dikontrol menggunakan variabel sosiodemografi dan faktor obstetrik. Kesimpulan: Intervensi diperlukan untuk mengurangi kehamilan yang tidak diinginkan seperti meningkatkan akses ke layanan keluarga berencana. -
Preventing Unplanned Pregnancy: Lessons from the States
JUNE 2019 Preventing Unplanned Pregnancy: Lessons from the States Isabel V. Sawhill Katherine Guyot Executive Summary In the context of a looming debate about women’s reproductive health, this paper reviews what we have learned about strategies for reducing unplanned pregnancies and births, especially at the state level. Our primary findings and conclusions are: • Unintended pregnancies are at an all-time low in the U.S. but still represent about 45% of all pregnancies. (Unintended pregnancies include those that women themselves say they did not want or that occurred earlier than they desired. We use “unintended” and “unplanned” interchangeably in this paper.) • About 40% of unplanned pregnancies end in abortion, while the other 60% result in a birth. The result is that about one-third of all births are unplanned. • Unintended pregnancies and births are most common among young unmarried women, especially teens and the most disadvantaged. However, these groups have also seen the largest declines in unintended pregnancy rates in recent years. • The reasons behind these declines remain somewhat obscure, but two potential reasons stand out. The first is changes in social norms around women’s roles, with more women expected to work, to get some postsecondary education, and to support their families, making unplanned childbearing more costly and the benefits of delay much greater. The second reason is greater access to and use of the most effective forms of contraception, such as long-acting reversible contraceptives. Other factors that could have played a role include the Great Recession and a decline in sexual activity. • Low-income women tend to have the least access to contraception through employer- sponsored health insurance, and many rely on publicly subsidized family planning services. -

Unintended Pregnancy and Abortion in the USA: Epidemiology and Public Health Impact
BLBK137-Paul February 13, 2009 13:25 CHAPTER 3 3 Unintended pregnancy and abortion in the USA: Epidemiology and public health impact Stanley K. Henshaw, PhD LEARNING POINTS r Unintended pregnancy occurs frequently in the USA, especially among women who are young, have low income, are Black or Hispanic, or have had a prior unintended pregnancy. r Unintended pregnancy and abortion result about equally from non-use of contraception and imperfect use, which in turn are related to chance-taking, problems with contraceptive methods, not expecting to have sex, and barriers to access to contraception. r Women with unwanted pregnancies have many reasons for choosing abortion, the most common of which are inadequate finances, lack of partner support, desire to continue education or career, not wanting more children, and feeling too immature. r The US abortion rate has been falling in recent years, especially among teenagers. r Although repeat abortion is often a source of concern, the data provide no justification for prejudicial attitudes. Guttmacher Institute were considered to result from unin- Introduction tended pregnancies, as were 35% of births, as reported in Couples in all developed countries want to control the the 2002 National Survey of Family Growth (NSFG) [2]. A timing and number of their children. Women typically pregnancy is considered to be unintended if the woman says initiate sexual activity long before they want children that at the time she became pregnant she wanted no more and continue long after they have their desired number, children or did not want to become pregnant until later. leaving them to rely on contraception during the majority Many unintended pregnancies come to be wanted, and of their reproductive lives. -
Amniocentesis and CVS UHL Obstetric Guideline
Amniocentesis and Chorionic Villus Sampling Maternity 1. Introduction and Scope This guideline is intended for the use of obstetric and midwifery staff involved in the care of pregnant women undergoing amniocentesis or chorionic villus sampling (CVS). It is estimated that around 5% of the pregnant population (approximately 30,000 women per annum in the UK) are offered a choice of invasive prenatal diagnostic tests. The type of test offered is dependent on several factors including gestational age, indication and placental position. Amniocentesis is the most common invasive antenatal diagnostic procedure undertaken in the United Kingdom (UK). Most amniocenteses are performed to obtain amniotic fluid for karyotyping. It is a procedure to remove amniotic fluid from the uterus. CVS involves aspiration or biopsy of placental villi and can be done via trans abdominal or trans cervical methods. In UHL this is done by a trans abdominal approach. 2. Recommendations 1. Women undergoing amniocentesis or CVS should be fully counselled prior to the procedure of the risks involved and informed consent documented. 2. Amniocentesis and CVS should be performed at the appropriate gestation. 3. A safe technique should be used to perform amniocentesis and CVS. 4. Operators performing amniocentesis and CVS should be trained to the local competencies expected, those expected by the Royal College of Obstetricians (RCOG) or an international equivalent. 5. Clinical considerations for performing amniocentesis or CVS for multiple pregnancy / in the third trimester / IUD / BBI. 1. Women undergoing amniocentesis or CVS should be fully counselled prior to the procedure and informed consent documented. Women should be advised of the risks of undergoing amniocentesis or CVS.