Diagnosing, Treating, and Managing Scleritis in 2020 an Expert Panel Recommendation Panel Members Melissa Toyos, Md Stephen D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Preseptal and Orbital Cellulitis
Journal of Microbiology and Infectious Diseases / 2014; 4 (3): 123-127 JMID doi: 10.5799/ahinjs.02.2014.03.0154 REVIEW ARTICLE Preseptal and orbital cellulitis Emine Akçay, Gamze Dereli Can, Nurullah Çağıl Yıldırım Beyazıt Univ. Medical Faculty Atatürk Training and Research Hospital Dept. of Ophthalmology, Ankara, Turkey ABSTRACT Preseptal cellulitis (PC) is defined as an inflammation of the eyelid and surrounding skin, whereas orbital cellulitis (OC) is an inflammation of the posterior septum of the eyelid affecting the orbit and its contents. Periorbital tissues may become infected as a result of trauma (including insect bites) or primary bacteremia. Orbital cellulitis generally occurs as a complication of sinusitis. The most commonly isolated organisms are Staphylococcus aureus, Streptococcus pneu- moniae, S. epidermidis, Haempphilus influenzae, Moraxella catarrhalis and S. pyogenes. The method for the diagnosis of OS and PS is computed tomography. Using effective antibiotics is a mainstay for the treatment of PC and OC. There is an agreement that surgical drainage should be performed in cases of complete ophthalmoplegia or significant visual impairment or large abscesses formation. This infections are also at a greater risk of acute visual loss, cavernous sinus thrombosis, meningitis, cerebritis, endo- phthalmitis, and brain abscess in children. Early diagnosis and appropriate treatment are crucial to control the infection. Diagnosis, treatment, management and complications of PC and OC are summarized in this manuscript. J Microbiol Infect Dis 2014; 4(3): 123-127 Key words: infection, cellulitis, orbita, preseptal, diagnosis, treatment Preseptal ve Orbital Sellülit ÖZET Preseptal selülit (PS) göz kapağı ve çevresindeki dokunun iltihabi reaksiyonu iken orbital selülit (OS) orbitayı ve onun içeriğini etkileyen septum arkası dokuların iltihabıdır. -

CAUSES, COMPLICATIONS &TREATMENT of A“RED EYE”
CAUSES, COMPLICATIONS & TREATMENT of a “RED EYE” 8 Most cases of “red eye” seen in general practice are likely to be conjunctivitis or a superficial corneal injury, however, red eye can also indicate a serious eye condition such as acute angle glaucoma, iritis, keratitis or scleritis. Features such as significant pain, photophobia, reduced visual acuity and a unilateral presentation are “red flags” that a sight-threatening condition may be present. In the absence of specialised eye examination equipment, such as a slit lamp, General Practitioners must rely on identifying these key features to know which patients require referral to an Ophthalmologist for further assessment. Is it conjunctivitis or is it something more Iritis is also known as anterior uveitis; posterior uveitis is serious? inflammation of the choroid (choroiditis). Complications include glaucoma, cataract and macular oedema. The most likely cause of a red eye in patients who present to 4. Scleritis is inflammation of the sclera. This is a very rare general practice is conjunctivitis. However, red eye can also be presentation, usually associated with autoimmune a feature of a more serious eye condition, in which a delay in disease, e.g. rheumatoid arthritis. treatment due to a missed diagnosis can result in permanent 5. Penetrating eye injury or embedded foreign body; red visual loss. In addition, the inappropriate use of antibacterial eye is not always a feature topical eye preparations contributes to antimicrobial 6. Acid or alkali burn to the eye resistance. The patient history will usually identify a penetrating eye injury Most general practice clinics will not have access to specialised or chemical burn to the eye, but further assessment may be equipment for eye examination, e.g. -

A Case of Very Limited Wegener's Granulomatosis and Scleritis
A Case of Very Limited Wegener's Granulomatosis and Scleritis Jean Yang, M.D. Case Presentation: The patient is a 75 year old man who underwent cataract extraction of the right eye in March 93. The surgery was uneventful. A year and half later, the patient developed a large, rapidly advancing conjunctival mass medially in the right eye. Biopsy of the lesion revealed chronic inflammation. The right eye was treated with topical dexamethasone/neomycin/polytrim without any improvement. The patient was referred in August this year. The past medical history was significant for hypertension. Review of systems was significant for fatigue. On examination, the visual acuity was counting fingers at 3 ft OD, and 20/30 OS. The biomicroscopic examination showed a large conjunctival mass superonasally as seen below. There was diffuse conjunctival injection and inflammation. Conjunctiva inferotemporally also appeared to be elevated as seen in the figure below. Superiorly, a corneal pannus was also noted. The rest of the exam and the exam of the left eye was unremarkable. An immunologic workup included a negative ANCA, an erythrocyte sedimentation rate of 65, mildly elevated soluble IL-2 receptor level at 894, and ANA with rat liver subtrate of 1:80. Urinalysis was positive for glucose, but negative for RBC. The rest of the workup including a chest X-ray, CBC, FTA-abs, RPR, rheumatoid factor, and immune complex assays were all negative. The patient underwent conjunctival and scleral biopsy of the right eye. Intraoperatively, after the conjunctiva was lifted, multiple scleral nodules were noted. Histopathology of the specimen revealed probable vasculitis with micro-abscesses, seen below, with epithelioid cells and eosinophils seen further below, suggestive of Wegener's granulomatosis. -

Red Eye Sub-Conjunctival Hemorrhage
AEP Course 1 Friday 1:00 - 2:00 pm Disclosures Red Eye • Consultant for Alcon Cecelia Koetting, OD FAAO Virginia Eye Consultants Norfolk, VA VOA Conference Norfolk 2018 Nothing makes the office more Multiple Causes of “Red Eye” nervous than when this walks in. • Sub-Conjunctival hemorrhage • Allergic Conjunctivitis • Viral Conjunctivitis • Bacterial Conjunctivitis • Episcleritis • Scleritis • Ocular Surface Disease How to Triage Sub-Conjunctival • On the phone • Get as much information as possible about which eye, Hemorrhage when, how, recent surgeries, recent trauma and what medications have been used • In the room • Gather the same information as well as details on symptoms • Help to avoid possible spread of bacterial and viral conjunctivitis 1 AEP Course 1 Friday 1:00 - 2:00 pm Causes • Straining from: • Broken blood vessel releasing blood into the • Coughing • Vomiting surrounding sub conjunctival tissue • Constipation • A bruise • Diarrhea • Lifting • More common in patients on blood thinners • Sneezing • Bruise more easily and will take longer to resolve • Rubbing the eyes • Contact lens • Severe dryness • Trauma, surgery, injections • Blood clotting disorders and blood thinners • Occasionally, high blood pressure High BP • Remember to ask if the patient is on blood thinners or blood pressure meds Allergic Conjunctivitis • Last time took BP meds • Possibly check BP in office if haven't taken • Inflammation in the lining of the conjunctiva from allergies • IgE and Mast Cell release • Symptoms: itching, redness, tearing, foreign body -
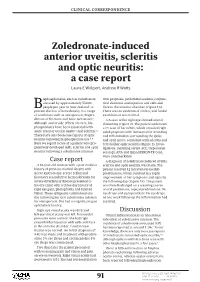
Zoledronate-Induced Anterior Uveitis, Scleritis and Optic Neuritis: a Case Report Laura E Wolpert, Andrew R Watts
clinical correspondence Zoledronate-induced anterior uveitis, scleritis and optic neuritis: a case report Laura E Wolpert, Andrew R Watts isphosphonates, such as zoledronate, with proptosis, periorbital oedema, conjunc- are used by approximately 55,000 tival chemosis and injection and cells and Bpeople per year in New Zealand1 to flare in the anterior chamber (Figure 1A). prevent the loss of bone density in a range There was no evidence of vitritis, and fundal of conditions such as osteoporosis, Paget’s examination was normal. 2 disease of the bone and bone metastases. A B-scan of the right eye showed scleral Although ocular side effects are rare, bis- thickening (Figure 2). The patient underwent phosphonates have been associated with a CT scan of her orbits, which revealed right- 3,4 4,5 acute anterior uveitis (AAU) and scleritis. sided proptosis with intraconal fat stranding There have also been case reports of optic and inflammation surrounding the globe 6–8 neuritis following bisphosphonate use. and optic nerve, consistent with scleritis and Here we report a case of a patient who pro- retrobulbar optic neuritis (Figure 3). Inves- gressively developed AAU, scleritis and optic tigations, including serum ACE, treponemal neuritis following a zoledronate infusion. serology, ANA and QuantiFERON-TB Gold, were unremarkable. Case report A diagnosis of zoledronate-induced uveitis, A 61-year-old woman with a past medical scleritis and optic neuritis was made. The history of previous morbid obesity with patient received 1g intravenous methyl- sleeve gastrectomy, severe reflux and prednisolone, which resulted in a rapid ileostomy secondary to hemicolectomy for improvement of her symptoms and signs by severe diverticular disease presented to the following day (Figure 1B). -

Retina Associated with Systemic Diseases*
MACULAR AND PARAMACULAR DETACHMENT OF THE NEUROSENSORY RETINA ASSOCIATED WITH SYSTEMIC DISEASES* BY Careen Y. Lowder, PhD, MD (BY INVITATION), Froncie A. Gutman, MD, Hernando Zegarra, MD (BY INVITATION), Z. Nicholas Zakov, MD (BY INVITATION)P James N. Lowder, MD (BY INVITATION), AND (BY INVITATION) John D. Clough, MD INTRODUCTION SEROUS RETINAL DETACHMENT (SRD) IN THE MACULAR REGION MAY DEVELOP AS A result of trauma, uveitis, optic neuritis, optic pit, and other conditions.1"2 In addition to these well-recognized disorders, there is a group ofpatients in whom transient episodes of SRD of the macula develop that are not presently associated with any recognized ocular or systemic disease. This group represents the clinical syndrome known as idiopathic central serous choroidopathy (CSC).2 The systemic implications of CSC are not known. Many reports have dealt with this without satisfactory evidence that there is a specific association between CSC and a systemic disease.1"3'4 This paper is a retrospective review of 168 cases of angiographically proved SRD of the macular region of unknown etiology that were seen at The Cleveland Clinic Foundation between 1971 and 1980. The associated systemic diseases were identified. Nine patients who had SRD of the posterior pole and subjective visual symptoms that appeared to correlate with an exacerbation oftheir system- ic diseases were included in the category of autoimmune disorders. Im- *From the Cleveland Clinic Foundation, Department of Ophthalmology, (Drs C. Lowder, Gutman, Zegarra, and Zakov), Department of Rheumatic and Immunologic Disease, (Dr Clough) and Department of Internal Medicine, University Hospitals,. (Dr J. Lowder) Cleveland, Ohio. -

The Clinical Features of Posterior Scleritis with Serous Retinal Detachment: a Retrospective Clinical Analysis
The clinical features of posterior scleritis with serous retinal detachment: A retrospective clinical analysis Zhizhang Dong The second aliated hospital and Yuying Children’s hospital of Wenzhou Medical University https://orcid.org/0000-0001-5150-8750 Yifeng Gan The second aliated hospital and Yuying Children’s hospital of Wenzhou Medical University Yinan Zhang The second aliated hospital and Yuying Children’s hospital of Wenzhou Medical University Yu Zhang The second aliated hospital and Yuying Children’s hospital of Wenzhou Medical University Juan Li ( [email protected] ) Guangren Hospital Aliated to School of Medicine of Xi'an Jiaotong University Haihua Zheng ( [email protected] ) The second aliated hospital and Yuying Children’s hospital of Wenzhou Medical University Research Article Keywords: Posted Date: November 30th, 2018 DOI: https://doi.org/10.21203/rs.2.48/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published at International Journal of Ophthalmology on July 18th, 2019. See the published version at https://doi.org/10.18240/ijo.2019.07.16. Page 1/13 Abstract Objective: To summarize the clinical features, systemic associations, risk factors and choroidal thickness(CT) changing in posterior scleritis (PS) with serous retinal detachment. Methods: This retrospective study included 23 patients with PS with retinal detachment from August 2012 to July 2017. All patients were documented with the Medical history and clinical features were recorded. The examinations included best corrected visual acuity (BACV), intraocular pressureIOP, fundus examination, routine eye examinations. Posterior coats thickness (PCT) was determined by B scan Ultrasound, the CT was measured by enhanced depth imaging spectral-domain optical coherence tomography (EDI-OCT). -

Ocular Manifestations of Systemic Lupus Erythematosus: a Review of the Literature Neal V
Ocular Manifestations of Systemic Lupus Erythematosus: A Review of the Literature Neal V. Palejwala, Emory University Harpreet S. Walia, Emory University Steven Yeh, Emory University Journal Title: Autoimmune Diseases Volume: Volume 2012, Number 2012 Publisher: Hindawi Publishing Corporation | 2012-05-31, Pages 1-9 Type of Work: Article | Final Publisher PDF Publisher DOI: 10.1155/2012/290898 Permanent URL: http://pid.emory.edu/ark:/25593/d8q18 Final published version: http://www.hindawi.com/journals/ad/2012/290898/ Copyright information: © 2012 Neal V. Palejwala et al. This is an Open Access work distributed under the terms of the Creative Commons Attribution 3.0 Unported License (http://creativecommons.org/licenses/by/3.0/). Accessed September 23, 2021 5:51 AM EDT Hindawi Publishing Corporation Autoimmune Diseases Volume 2012, Article ID 290898, 9 pages doi:10.1155/2012/290898 Review Article Ocular Manifestations of Systemic Lupus Erythematosus: A Review of the Literature Neal V. Palejwala, Harpreet S. Walia, and Steven Yeh Section of Vitreoretinal Disease and Surgery, Department of Ophthalmology, Emory Eye Center, Emory University School of Medicine, Atlanta, 30322 GA, USA Correspondence should be addressed to Steven Yeh, [email protected] Received 5 May 2012; Accepted 31 May 2012 Academic Editor: Hiroshi Okamoto Copyright © 2012 Neal V. Palejwala et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. About one-third of patients suffering from systemic lupus erythematosus have ocular manifestations. The most common manifestation is keratoconjunctivitis sicca. The most vision threatening are retinal vasculitis and optic neuritis/neuropathy. -

Aspergillus Niger As an Unusual Cause of Scleritis and Endophthalmitis
584 Manners, O'Connell, Guy,JGoynson, Canning, Etchells Table I Dye test titres, IgM levels, IgG avidity, and total although cases have been reported.6 Virtually all immunoglobulin levels in serum (S) and vitreous (V) samples reported cases had associated systemic features such as lymphadenopathy. Our provisional diag- Time (weeks) after Dye test Dye test IgM IgG Total Ig Br J Ophthalmol: first published as 10.1136/bjo.78.7.584 on 1 July 1994. Downloaded from onset ofsymptoms titre (IUlml) (IU) avidity (g) nosis of acquired toxoplasmosis affecting the eye 12 (S) 1/256 125 75 32% NT was extremely unusual in an immunocompetent 22 (S) 1/256 125 55 36% NT 60-year-old person with no other symptoms. The 37 (S) 1/256 125 36 NT 12-100 37 (V) 1/16 8 NT NT 0-237 presence of toxoplasmal DNA in the vitreous sample, demonstrated by PCR was strong addi- NT=not tested. tional supporting evidence. Part of this work was funded by a research grant from the Toxoplasmosis Trust. months previously. An avidity of 40% is usually seen in infections acquired more than 6 months I Aouizerate F, Cazenave J, Poirier L, Verin P, Cheyrou A, Begneret J, et al. Detection of Toxoplasma gondii in aqueous previously. The Goldmann-Witmer coefficient,3 humour by polymerase chain reaction. BrJ Ophthalmol 1993; the quotient of relative amounts of toxoplasmal 77: 107-9. 2 Burg L, Grover CM, Pontethy P, Boothroyd J. Direct and antibodies in vitreous and serum, was 3*19:1. sensitive detection of pathogenic protozoan Toxoplasma Baarsma et all consider a coefficient ofmore than gondii by polymerase chain reaction. -

Lacrimal Drainage Surgery in Wegener's Granulomatosis
Br J Ophthalmol 2000;84:329–331 329 Lacrimal drainage surgery in Wegener’s Br J Ophthalmol: first published as 10.1136/bjo.84.3.329 on 1 March 2000. Downloaded from granulomatosis AnthonySLKwan,GeoVrey E Rose Abstract A small number of surgeons were involved, Aim—To examine the results of open all using the following technique. A linear lacrimal surgery in patients with Wegen- paranasal incision was followed by complete er’s granulomatosis. release of medial canthal tendon and a large Methods—A retrospective review of pa- rhinostomy was created, together with partial tients with Wegener’s granulomatosis who anterior ethmoidectomy. Anterior and poste- underwent lacrimal surgery over a 17 year rior flaps were formed from both nasal and lac- period. rimal sac mucosa and the anastomoses united Results—11 patients were identified and a with multiple 6/0 Vicryl (Ethicon) sutures. The total of 14 primary dacryocystorhinosto- medial canthal tendon, orbicularis, and skin mies (DCR) and one revisional DCR were were closed in layers and silicone stents used in performed; symptomatic relief was most cases. achieved in 13/14 operations and one patient required revisional surgery for persistent symptoms. There were no in- Results traoperative and few postoperative com- Eleven patients (eight males, three females) plications. are included in the study, aged between 34 Conclusions—In contrast with some pre- to 63 years (mean 52 years) at presen- vious reports, open DCR appears to be a tation. Wegener’s disease had been safe procedure and it is recommended as a present for an average of 9.8 years (range treatment for lacrimal obstruction in 4–22) and 9/11 patients were maintained on patients with Wegener’s granulomatosis, systemic immunosuppression before surgery. -

Optic Neuritis As Ocular Manifestation of Wegener's Granulomatosis
CASE REPORT DOI: 10.5603/OJ.2016.0021 Optic neuritis as ocular manifestation of Wegener’s granulomatosis — case report Dorota Borowicz, Edyta Koman, Katarzyna Nowomiejska, Robert Rejdak Department of General Ophthalmology, Medical University in Lublin, Poland ABSTRACT Wegener’s granulomatosis (WG) is a systemic, autoimmune, granulomatous necrotising inflammation of unk- nown aetiology. WG is described by the triad, which includes: rhinitis, and pulmonary and kidney dysfunction. The ocular signs are inflammatory orbital disease, nasolacrimal ducts obstruction, conjunctivitis, episcleritis, scleritis uveitis, retinal vasculitis, and optic neuritis. This article describes the case of a patient with optic neuritis associated with WG. KEY WORDS: Wegener’s granulomatosis, ophthalmic manifestations, c-ANCA Ophthalmol J 2016; Vol. 1, No. 3, 109–113 INTRODUCTION of WG are based on patient examination and lab- Wegener’s granulomatosis (WG) is a systemic, oratory tests, which include kidney parameters, autoimmune, granulomatous necrotising inflamma- radiogram of the lungs, and histopathological veri- tion and vasculitis (inflammation of the small to the fication. The specific marker of this disease is anti- medium vessels). The aetiology of this disease is un- bodies against cytoplasmic neutrophils (c-ANCA), known. The first case of this disease was described in which increases by 95% in the active phase and 1897 by Peter McBride who was a Scottish otolar- only 10-20% in the inactive phase of the disease. yngologist. Heinz Karl Ernst Klinger was a medical The positive c-ANCA is a useful tool for screening. student who added information on the anatomical The general treatment is based on glucocorticoids pathology in 1931. Frederick Wegener was a Ger- and cyclophosphamide [1, 3].