Improving Access to Abortion Services in Aotearoa New Zealand
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rt I Are Sex Selective Abortions Wrong? J.M.Johnston Masters Student, Bioethics Centre, University of Otago
rt I Are Sex Selective Abortions Wrong? J.M.Johnston Masters Student, Bioethics Centre, University of Otago, 'THIRD WORLD GIRL ABORTIONS HERE-DOCTORS'. 8 weeks by chorionic villus sampling - a test checking chromosomal abnormalities that, like amniocentesis, is also 'WARNING OVER FOETAL SEX TESTS'. able to accurately identify the sex of the fetus (Morgan, 'FAMILY PLANNING WARNS OF SEX TEST'. 1988, p355). There seem to be two main reasons why a 'EXPERT URGES FEWER FOETUS SEX TESTS'. woman or a couple would want to use prenatal diagnosis and abortion to select the sex of their child. The first, and less controversial, reason may be to avoid the birth So read the headlines of The Dominion and The New of a child with sex linked diseases such as haemophilia or Zealand Herald in early April 2000. Identification of the sex Duchenne muscular dystrophy (Morgan, 1988, p356). The of a fetus is possible as early as six weeks into a second reason for sex selective abortion is to eliminate a pregnancy and based on anecdotal evidence from the Family fetus of the 'wrong' sex - for instance the abortion of a Planning Association, the New Zealand Medical Association male fetus by a woman who wants to have a daughter. It is believes that '[a] third world practice of couples aborting with this second use ofsex identification and abortion that I baby girls has spread to New Zealand' (The Dominion, 6 am concerned, although I do note that abortions performed April 2000, p.1). New Zealand Medical Association for the first mentioned 'therapeutic' reason are not without Chairwoman Pippa MacKay has said that although it is their critics ( see for instance Harris, 1985). -

The Epidemiology of Abortion and Its Prevention in Chile, 79(5) Rev
Gene Gene Start Gene End Motif Start Motif End Motif Strand Exon Start Exon End HS Start HS End Distance NLGN4X 5808082 6146706 5821352 5821364 gtggccacggcgg ‑ 5821117 5821907 5811910 5813910 7442 AFF2 147582138 148082193 148048477 148048489 ccaccatcacctc + 148048319 148048609 148036319 148040319 8158 NLGN3 70364680 70391051 70386983 70386995 gtggatatggtgg + 70386860 70387650 70371089 70377089 9894 MECP2 153287263 153363188 153296166 153296178 gtggtgatggtgg ‑ 153295685 153296901 153306976 153308976 10798 FRMPD4 12156584 12742642 12739916 12739928 ccaccatggccgc + 12738647 12742642 12721454 12727454 12462 PHF8 53963112 54071569 54012352 54012364 ccaccatgtcctc ‑ 54012339 54012382 54025089 54033089 12725 RAB39B 154487525 154493852 154493567 154493579 cctccatggccgc ‑ 154493358 154493852 154478566 154480566 13001 FRMPD4 12156584 12742642 12736309 12736321 ggggcaagggagg + 12735619 12736909 12721454 12727454 14867 GRPR 16141423 16171641 16170710 16170722 cctccgtggccac + 16170378 16171641 16208454 16211454 37732 AFF2 147582138 148082193 148079262 148079274 cccccgtcaccac + 148072740 148082193 148036319 148040319 38943 SH3KBP1 19552082 19905744 19564111 19564123 cctccttatcctc ‑ 19564039 19564168 19610454 19614454 46331 PDZD4 153067622 153096003 153070331 153070343 cccccttctcctc ‑ 153067622 153070355 153013976 153018976 51355 SLC6A8 152953751 152962048 152960611 152960623 ccaccctgacccc + 152960528 152962048 153013976 153018976 53353 FMR1 146993468 147032647 147026533 147026545 gaggacaaggagg + 147026463 147026571 147083193 147085193 56648 HNRNPH2 -
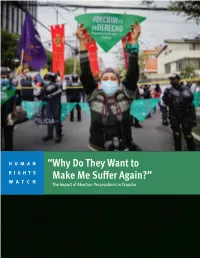
“Why Do They Want to Make Me Suffer Again?” the Impact of Abortion Prosecutions in Ecuador
HUMAN “Why Do They Want to RIGHTS WATCH Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador “Why Do They Want to Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador Copyright © 2021 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-62313-919-3 Cover design by Rafael Jimenez Human Rights Watch defends the rights of people worldwide. We scrupulously investigate abuses, expose the facts widely, and pressure those with power to respect rights and secure justice. Human Rights Watch is an independent, international organization that works as part of a vibrant movement to uphold human dignity and advance the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Sydney, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org JULY 2021 ISBN: 978-1-62313-919-3 “Why Do They Want to Make Me Suffer Again?” The Impact of Abortion Prosecutions in Ecuador Summary ........................................................................................................................... 1 Key Recommendations ....................................................................................................... 8 To the Presidency ................................................................................................................... -

Induced Abortion in Chile
In Brief Induced Abortion in Chile Chile is one of a small handful of countries worldwide that Abortion-related deaths and injuries appear to have declined dramatically prohibit induced abortion under any circumstance, including In the 1960s, many Chilean women if a woman’s life is at risk. The longstanding ban, which undergoing unsafe abortions died as a result, or suffered serious short- or long- runs counter to Chile’s stated commitment to international term health complications for which they women’s rights treaties, faces a robust challenge in the did not receive the medical treatment they needed.9 In 1960, there were 294 form of a recent bill proposed by the government of maternal deaths per 100,000 live births,10 and one-third of these deaths were at- President Bachelet that would allow the procedure under tributable to unsafe abortion.11 One in limited circumstances. Yet informed debate on the topic is five hospital beds in obstetric depart- ments were occupied by women receiving hindered by the lack of data on the incidence and context of postabortion treatment. clandestine induced abortion. Chile’s maternal mortality ratio fell to 55 deaths per 100,000 live births by In every country, regardless of the legal No data exist on the characteristics of 1990, and to 22 by 2013.12 The precise status of induced abortion, some women women obtaining abortions in Chile, nor contribution of unsafe induced abortion experiencing an unintended pregnancy on their reasons for doing so. As one to overall maternal mortality is unclear, turn to abortion to end it.1 Chile is no researcher points out, “we do not know… but experts agree that far fewer deaths exception to this worldwide pattern. -

Fighting to Choose: the Abortion Rights Struggle in New Zealand. by Alison Mcculloch
REVIEWS (BOOKS) 165 Fighting to Choose: The Abortion Rights Struggle in New Zealand. By Alison McCulloch. Victoria University Press, Wellington, 2013. 339pp. NZ price: $50.00. ISBN: 9780864738868. This is a partisan and passionate account of abortion politics in New Zealand, but it is also a scholarly, extensively footnoted, well-researched and fascinating history of pro- choice struggles, anti-abortion politics and the ongoing anomalies in this country’s abortion laws and regulatory processes. Acknowledgements start with McCulloch’s account of her need to present herself as ‘mentally unstable’ in order to secure her access to an abortion in her twenties and her anger at having to run the gauntlet of anti- abortion protesters as she entered Wellington’s Parkview Clinic for the procedure. Her research on the project was initiated in 2007 with a grant from the Women’s National Abortion Action Campaign (WONAAC). The book is illustrated by a range of photos assembled from the archives of the Alexander Turnbull Library and various activist organizations. McCulloch’s pro-choice position is articulated in the opening pages of the introduction. The first question that the book addresses is why the women’s movement in New Zealand failed to achieve control by women over their fertility – in particular, the right to abortion. Conservative thinking and the power of the Catholic Church, combined with what McCulloch identifies as the problematic reformist strategies of the Abortion Law Reform Association (ALRANZ), are identified as the reasons for New Zealand’s relatively restrictive abortion legislation, which nevertheless provides the framework within which 15,000 abortions are approved each year. -

Abortion MARCH 2016
MORAL, SOCIAL and ETHICAL issues for today’s SALVATION ARMY Published by the Moral and Social Issues (Ethics) Council New Zealand, Fiji and Tonga Territory Issued by authority of the Territorial Commander Abortion MARCH 2016 Is abortion an issue in New Zealand society today? Your response matters Abortion is on the decline overall in New Zealand. We have The Salvation Army believes life is a gift from God and that we achieved a 20-year low in the number of pregnancies terminated are answerable to God for the taking of life. We, like many other by choice. Nevertheless, more than13,000 abortions were Christian churches, accept the moment of fertilisation as the performed in this country in 2014. And more than a third of those start of human life and, in most instances would not accept were repeat occurrences where at least one abortion had been abortion as a justifiable choice. performed previously and, in some cases, as many as eight. There are exceptions where The Salvation Army accepts (as Abortion appears to be readily obtained in New Zealand. Despite noted in our International Positional Statement2), that a legislation requiring various checks and balances on decisions termination is appropriate. These are when: that an abortion is permitted, 98–99% of all abortions are • carrying the pregnancy further seriously threatens the life of granted on the basis of the mother’s medical health. Some the mother; or would say this is virtually ‘abortion on demand’. • reliable diagnostic procedures have identified a foetal Abortion is a polarising issue. Political debate on abnormality considered incompatible with survival for more decriminalisation has surfaced repeatedly in New Zealand over than a very brief post-natal period. -

Housewives' Depression
Housewives' Depression THE DEBATE OVER ABORTION AND BIRTH CONTROL IN THE 1930s* NEW ZEALAND has received acclaim for its ready recognition of women's rights. Women had, in the public sphere, less difficulty in breaking down the barriers to their participation than their sisters in England or America.' But, in the central areas of private morality, birth control and abortion, New Zealand women have not been granted such ready recog- nition of their autonomy. The first birth control clinic was established in New Zealand in 1953, 37 years after Margaret Sanger's first attempt to open a clinic in New York City, and 32 years after the opening of Marie Stopes's Marlborough Road clinic.2 While in England and America the government eventually took some responsibility for ensuring access to legal abortion, in New Zealand abortion remains limited to certain health grounds.3 Control of fertility raises questions of social, religious, and psycho- logical importance. Women's demands for birth control challenge the 'basic moral assumptions of a male dominated society' and threaten to overturn accepted social roles.4 This was particularly true in New Zealand. The nineteenth-century ideal of woman as the 'colonial help- * I am indebted to Erik Olssen who directed the original research for this paper. Thanks also to Lynne Milne for her comments, and Andree Levesque for her encouragement. 1 Raewyn Dalziel has persuasively argued that the vote was granted precisely because it did not threaten a change in women's prescribed sphere. R. Dalziel, 'The Colonial Helpmeet: Women's Role and the Vote in Nineteenth-Century New Zealand', New Zealand Journal of History, II (1977), 112-23. -

Bibliography of Sexuality Studies in Latin America
Bibliography of Sexuality Studies in Latin America In 1997 Donna J. Guy and I published a bibliography of sexuality studies on Latin America in our edited book Sex and Sexuality in Latin America (New York University Press, 1997), including studies in a wide variety of fields. This bibliography was updated for the Spanish edition of that book, Sexo y sexualidades en América Latina (Paidos, Buenos Aires, 1998); that version included a number of items that had come to our attention after we turned in the book to NYU. Interestingly, the number of publications in Latin America (and in Spanish and Portuguese) increased in that brief period, and continues to increase. Adán Griego has added his own bibliography and has agreed to maintain it and keep it current. The bibliography that follows is based on the previous ones but has the advantage of not being fixed in time. —— Daniel Balderston, 1999. This bibliographic list is organized alphabetically by author, or by title in a few cases where no specific author appears. Select the initial letter of the author or the title of the work you are looking for or simply scroll down the list. Please send corrections, additions and comments to: [email protected] A A las orillas de Lesbos. Narrativa lésbica. Lima: MHOL, 1997. Abad, Erika Gisela. "¿La Voz de Quién?" Diálogo, No.12, (Summer 2009): 28. Abdalla, Fernanda Tavares de Mello and Nichiata, Lúcia Yasuko Izumi. A Abertura da privacidade e o sigilo das informações sobre o HIV/Aids das mulheres atendidas pelo Programa Saúde da Família no município de São Paulo, Brasil. -

Amnesty International Report 2014/15 the State of the World's Human Rights
AMNESTY INTERNATIONAL OF THE WORLD’S HUMAN RIGHTS THE STATE REPORT 2014/15 AMNESTY INTERNATIONAL REPORT 2014/15 THE STATE OF THE WORLD’S HUMAN RIGHTS The Amnesty International Report 2014/15 documents the state of human rights in 160 countries and territories during 2014. Some key events from 2013 are also reported. While 2014 saw violent conflict and the failure of many governments to safeguard the rights and safety of civilians, significant progress was also witnessed in the safeguarding and securing of certain human rights. Key anniversaries, including the commemoration of the Bhopal gas leak in 1984 and the Rwanda genocide in 1994, as well as reflections on 30 years since the adoption of the UN Convention against Torture, reminded us that while leaps forward have been made, there is still work to be done to ensure justice for victims and survivors of grave abuses. AMNESTY INTERNATIONAL This report also celebrates those who stand up REPORT 2014/15 for human rights across the world, often in difficult and dangerous circumstances. It represents Amnesty International’s key concerns throughout 2014/15 the world, and is essential reading for policy- THE STATE OF THE WORLD’S makers, activists and anyone with an interest in human rights. HUMAN RIGHTS Work with us at amnesty.org AIR_2014/15_cover_final.indd All Pages 23/01/2015 15:04 AMNESTY INTERNATIONAL Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. -

Abortion Law and Policy Around the World: in Search of Decriminalization Marge Berer
HHr Health and Human Rights Journal HHR_final_logo_alone.indd 1 10/19/15 10:53 AM Abortion Law and Policy Around the World: In Search of Decriminalization marge berer Abstract The aim of this paper is to provide a panoramic view of laws and policies on abortion around the world, giving a range of country-based examples. It shows that the plethora of convoluted laws and restrictions surrounding abortion do not make any legal or public health sense. What makes abortion safe is simple and irrefutable—when it is available on the woman’s request and is universally affordable and accessible. From this perspective, few existing laws are fit for purpose. However, the road to law reform is long and difficult. In order to achieve the right to safe abortion, advocates will need to study the political, health system, legal, juridical, and socio-cultural realities surrounding existing law and policy in their countries, and decide what kind of law they want (if any). The biggest challenge is to determine what is possible to achieve, build a critical mass of support, and work together with legal experts, parliamentarians, health professionals, and women themselves to change the law—so that everyone with an unwanted pregnancy who seeks an abortion can have it, as early as possible and as late as necessary. Marge Berer is international coordinator of the International Campaign for Women’s Right to Safe Abortion, London, UK, and was the editor of Reproductive Health Matters, which she founded, from 1993 to 2015. Please address correspondence to Marge Berer. Email: [email protected]. -
Access to Abortion Reports
ACCESS TO ABORTION: An Annotated Bibliography of Reports and Scholarship Second edition (as of April 1, 2020) prepared by The International Reproductive and Sexual Health Law Program Faculty of Law, University of Toronto, Canada, 2020 http://www.law.utoronto.ca/documents/reprohealth/abortionbib.pdf Online Publication History: This edition: Access to Abortion: An Annotated Bibliography of Reports and Scholarship. “Second edition,” current to April 1 2020, published online August 31, 2020 at: http://www.law.utoronto.ca/documents/reprohealth/abortionbib.pdf Original edition: “Access to Abortion Reports: An Annotated Bibliography” (published online January 2008, slightly updated January 2009) has been moved to: http://www.law.utoronto.ca/documents/reprohealth/abortionbib2009.pdf Publisher: The International Reproductive and Sexual Health Law Program Faculty of Law, University of Toronto, 78 Queen’s Park Crescent, Toronto Canada M5S 2A5 Website Reprohealthlaw Blog Contact: reprohealth.law{at}utoronto.ca Acknowledgements: We are most grateful to Professor Joanna Erdman for founding this bibliography in 2008-9. We are also indebted to Katelyn Sheehan (LL.M.) and Sierra Farr (J.D. candidate) for expertly collecting and analyzing new resources up to April 1, 2020, and to Sierra Farr for updating the introduction to this second edition. Updates: Kindly send suggestions for the next edition of this bibliography to: Professor Joanna Erdman, MacBain Chair in Health Law and Policy, Health Law Institute, Schulich School of Law, Dalhousie University, Email: joanna.erdman{at}dal.ca ACCESS TO ABORTION: An Annotated Bibliography of Reports and Scholarship, 2020 AN INTRODUCTION TO THE ANNOTATED BIBLIOGRAPHY: Widespread evidence indicates that abortion services remain inaccessible and inequitably available for many people despite legal entitlement.1 This is true in jurisdictions that permit abortion for specific indications (e.g. -

Submission of the Equal Employment Opportunities Commissioner on Abortion Law Reform
Submission of the Equal Employment Opportunities Commissioner on Abortion Law Reform 1 June 2018 Contact Person: Jackie Blue Equal Opportunities Commissioner New Zealand human Rights Commission [email protected] 1 Submission of the Equal Employment Opportunities Commissioner on Abortion Law Reform Contents Introduction ............................................................................................................................................ 3 I. Current Law ..................................................................................................................................... 4 What makes abortion a crime? ........................................................................................................... 4 Regulation of abortions ...................................................................................................................... 5 II. Human Rights Law and Abortion .................................................................................................... 6 New Zealand Bill of Rights Act 1990 ................................................................................................... 6 International Human Rights Framework ............................................................................................ 6 CEDAW Committee Comments to New Zealand .............................................................................. 10 III. Specific Issues ..........................................................................................................................