Prehospital-Scene-Managementv6.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2013 ANNUAL REPORT CITY of MILTON FIRE DEPARTMENT 2013 ANNUAL REPORT
CITY OF MILTON FIRE DEPARTMENT 2013 ANNUAL REPORT CITY of MILTON FIRE DEPARTMENT 2013 ANNUAL REPORT 2013 was another very active and productive year for the City of Milton Fire Department which afforded great opportunities to implement positive improvements, placing the department in a very stable position for coming years. Overall emergency response activity was slightly below the prior year, allowing members to complete many ongoing projects, while also accomplishing several long-term goals. All of this activity has placed us in an excellent position to accomplish our primary mission of providing emergency services to the citizens of Milton. EMERGENCY ACTIVITY Despite a slight reduction in the overall number of emergency responses, 2013 still presented several challenging incidents requiring more than the response of the initial alarm assignment. The total number of emergency calls decreased by roughly 1.75%, down to 1,463 calls, from 1,489 the previous year. This reduction is attributable to two related issues: a reduction of nearly 5% in the number of medical response calls, and a nearly 16% reduction in the number of vehicle accidents. There is no clear explanation for the cause of these reductions. Otherwise, this year’s activity actually reflects a continued stabilization of annual activity over the past 10 years to roughly 1,500 calls per year. Rescue calls decreased this year, now totaling 1,202 calls, but still constitute the vast majority of our emergency calls, now 82% of our annual emergency activity. Rescue calls include: medical emergencies such as strokes, heart attacks, falls, etc.; all vehicle accidents including those that involve entrapment requiring forcible extrication with specialized hydraulic tools such as the “Jaws of Life”; and rescue calls like a child locked in a vehicle, elderly who have fallen and need help back into bed (lift assist), and even the occasional animal rescue. -

Vehicle Extrication
VEHICLE EXTRICATION Rio Hondo Regional Truck Operations Academy COURSE OBJECTIVES • Review of basic operations and terminology • Review Airbags, SRS, Battery locations and 5-10-20 Rule • Review Hybrid and AFV • Review Stabilization • Review Extrication techniques • Station A Equipment Review • Questions BASIC OPERATIONS • Scene Size Up • Vehicle Assessment “Reading the Wreck” • Patient Assessment • Stabilization • Scan for Airbags/SRS “Peel and Peek” • Gain Access to Patient “5-10-20 Rule” • Extrication Techniques • Patient Removal SIZE UP • Scene Safety and assessment • Victim assessment • Vehicle assessment “Reading the Wreck” • Extrication assessment • Size-up continues until the incident is terminated SCENE ASSESSMENT • Scene Safety • Vehicle traffic • Safe working area • Fuel spills • Down power lines • Environmental considerations • Fires • Alternative Fuel Vehicle leak VEHICLE ASSESSMENT • “Reading the Wreck” Position, Damage and Stability Vehicle construction and type Vehicle and Patient Condition • Vehicle safety systems Air bags/SRS Seat belt Pretensioners Batteries Glass Management READING THE WRECK FULL FRAME CONSTRUCTION Designed to Deflect Energy UNIBODY CONSTUCTION Designed to Absorb/Transfer Energy SPACE FRAME CONSTRUCTION Designed to Absorb/Transfer Energy High Strength Steel VEHICLE ANATOMY One-piece hydroformed body side rings. Door hinges secured by thick through-bolts located in A- and B-pillars. Cast magnesium transverse beam behind the instrument panel. Triple-rolled Pillar/Rail design resists roof collapse. Shock -
Highway Safety and Vehicle Extrication
CHAPTER 38 Highway Safety and Vehicle Extrication HANDOUT 38-1: Evaluating Content Mastery Student’s Name CHAPTER 38 QUIZ EVALUATION Write the letter of the best answer in the space provided. ______ 1. The recommended method of stabilizing a vehicle on its wheels is to use: A. three-step chocks.C. one-step chock. B. two-step chocks.D. bumper jacks. ______ 2. When placing cribbing under a vehicle, remember to: A. kneel down while keeping one hand on the vehicle. B. kneel down while keeping one hand on the ground. C. squat down and remain on the balls of your feet. D. lie down and slip the cribbing in place. ______ 3. The two types of vehicle glass include: A. laminated (contains a plastic sheet) and tempered (breaks into small fragments). B. laminated (breaks into rounded pieces) and tempered (contains a plastic sheet). C. laminated (contains a plastic sheet) and tempered (breaks into rounded pieces). D. laminated (breaks into sharp fragments) and tempered (contains a plastic sheet). ______ 4. If you “try before you pry,” you can often achieve: 1 A. limited access.C. high-angle access. B. simple access.D. complex access. ______ 5. A flathead ax is usually required to: A. remove a crushed steering wheel.C. pry open a distorted car door. B. break through a windshield.D. remove seat backs. ______ 6. The roof support that is between the front door and the back door of a four-door sedan is called the: A. safety post.C. B-post. B. A-post.D. C-post. -
Crash Injury Research and Engineering Network Program Report
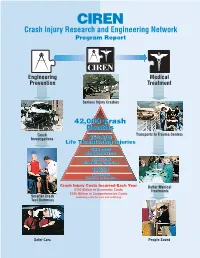
CIREN Crash Injury Research and Engineering Network Program Report Engineering Medical Prevention Treatment Serious Injury Crashes 42,000 Crash Deaths Crash Transports to Trauma Centers Investigations 250,000 Life Threatening Injuries 500,000 Hospitalized 2,000,000 Disabling Injuries 4,000,000 ER Visits 27,000,000 Vehicles in Crashes Crash Injury Costs Incurred Each Year Better Medical $100 Billion in Economic Costs Treatments $350 Billion in Comprehensive Costs Smarter Crash (including costs for pain and suffering) Test Dummies Safer Cars People Saved Engineering Medical Prevention Treatment Foreword by Jeffrey W. Runge, M.D., NHTSA Administrator As an emergency physician I personally have learned from CIREN research. I have used the life- saving techniques developed by CIREN for the diagnosis of liver injuries in crashes with 2-point belts. Furthermore, I have been able to teach better emergency care for crash victims because of CIREN findings. The medical and engineering research efforts of CIREN form a valuable program of the National Highway Traffic Safety Administration (NHTSA). CIREN has forged powerful teams of medical researchers and safety engineers from NHTSA, universities, and the automotive industry. These teams are performing leading edge research on serious injuries in real-world crashes to advance safety. The crash injury research contributions of the CIREN centers that are noted in this report include many findings that currently are in various stages of development, testing, and evaluation. As these findings are applied over time, the safety benefits of this basic research will become a reality and result in a Safer America. CIREN researchers have produced more than 100 scientific publications based on research on more than 1,000 crash injured people. -

Fireterminology.Pdf
Abandonment: Abandonment occurs when an emergency responder begins treatment of a patient and the leaves the patient or discontinues treatment prior to arrival of an equally or higher trained responder. Abrasion: A scrape or brush of the skin usually making it reddish in color and resulting in minor capillary bleeding. Absolute Pressure: The measurement of pressure, including atmospheric pressure. Measured in pound per square inch absolute. Absorption: A defensive method of controlling a spill by applying a material that absorbs the spilled material. Accelerant: Flammable fuel (often liquid) used by some arsonists to increase size or intensity of fire. Accelerator: A device to speed the operation of the dry sprinkler valve by detecting the decrease in air pressure resulting in acceleration of water flow to sprinkler heads. Accountability: The process of emergency responders (fire, police, emergency medical, etc...) checking in as being on-scene during an incident to an incident commander or accountability officer. Through the accountability system, each person is tracked throughout the incident until released from the scene by the incident commander or accountability officer. This is becoming a standard in the emergency services arena primarily for the safety of emergency personnel. Adapter: A device that adapts or changes one type of hose thread, type or size to another. It allows for connection of hoses and pipes of incompatible diameter, thread, or gender. May contain combinations, such as a double-female reducer. Adapters between multiple hoses are called wye, Siamese, or distributor. Administrative Warrant: An order issued by a magistrate that grants authority for fire personnel to enter private property for the purpose of conducting a fire prevention inspection or similar purpose. -
An Examination of Emergency Response Scenarios for ADS Final Report October 2018
An Examination of Emergency Response Scenarios for ADS Final Report October 2018 Emergency Response Scenarios for ADS Final Report Terry, T., Trimble, T. E., Blanco, M., Fitzgerald, K. E., Fitchett, V. L., and Chaka, M. (2018). An Examination of Emergency Response Scenarios for ADS. Farmington Hills, MI: Crash Avoidance Metrics Partners LLC. i Emergency Response Scenarios for ADS Final Report Executive Summary In the future, vehicles equipped with automated driving systems (ADS) that drive us instead of us driving them will become a reality. These vehicles will integrate onto roadways and may change operational interactions with other vehicles in certain scenarios. Public safety officials, such as law enforcement, fire and rescue, and emergency medical personnel routinely interact with a broad spectrum of public and private vehicles to protect people, to investigate crimes or crashes, and to save lives. This research effort sought to determine the following: • What are the common scenarios where public safety officials must engage in several different interactions and interaction types with a broad spectrum of public and private vehicles? • What are the protocols used during those scenarios and the different interactions and interaction types? • Do variables such as weather, roadway type, geometry, or vehicle type impact current protocols used in those scenarios? • How may the current operations change due to the introduction of ADS-equipped vehicles in driverless operation (DO)? • Are there opportunities where the interactions of public safety officials could be improved with the introduction of ADS-equipped vehicles in DO? An extensive review of available literature and consultations with subject matter experts allowed the research team to determine the most common scenarios where public safety officials interact with other vehicles. -

Emergency Response Guide
INFORMATION FOR FIRST AND SECOND RESPONDERS EMERGENCY RESPONSE GUIDE TESLA MODEL S ELECTRIC VERSION: 001 CONTENTS 0. Emergency Response Sheet Page 1 1. Identification / recognition Page 2 2. Immobilization / stabilization / lifting Page 5 3. Disable direct hazards / safety regulations Page 7 4. Access to the occupants Page 12 5. Stored energy / liquids / gases / solids Page 19 6. In case of fire Page 23 7. In case of submersion Page 25 8. Towing / transportation / storage Page 26 9. Important additional information Page 28 10. Explanation pictograms used Page 29 Model S Emergency Response Guide TESLA MODEL S From 2016—2021 Airbag Stored gas Seatbelt SRS Pedestrian inflator preten- Control protection sioner Unit active system Automatic Gas strut/ High Zone rollover pre-loaded strength requiring protection spring zone special system attention Battery Ultra ca- Fuel tank Gas tank Safety low volt- pacitor, low valve age voltage High High volt- High Fuse box Ultra voltage age power voltage disabling capaci- battery cable/com- discon- high tor, high pack ponent nect voltage voltage system Cable cut TESLA MODEL S ID No. Version No. From 2016 — 2021 TESLA–202012–004 01 1. Identification / recognition WARNING LACK OF ENGINE NOISE DOES NOT MEAN VEHICLE IS OFF. SILENT MOVEMENT OR INSTANT RESTART CAPABILITY EXISTS UNTIL VEHICLE IS FULLY SHUT DOWN. WEAR APPROPRIATE PERSONAL PROTECTIVE EQUIPMENT (PPE). Badging and Door Handles Model S can be identified by its badges and uniquely shaped door handles. The model name appears on the rear of the vehicle. NOTE: The “D” at the end of the battery badge (or “DUAL MOTOR” badge for newer vehicles) on the RH side of the vehicle indicates that the vehicle is a Dual Motor configuration. -
Basic Vehicle Extrication Student Guide
State of Michigan Basic Vehicle Extrication Student Guide Copyright Copyright © 2001 Raymond Haring and George Lutz. All rights reserved. Basic Vehicle Extrication This course is the property of Raymond Haring and George Lutz and is protected by copyright. Any reproduction in whole, part or by any means is strictly prohibited without prior written permission. Permission for the use and reproduction of this course has been extended to the Michigan Fire Fighter’s Training Council and their qualified instructors for instruction of Michigan Fire Fighter’s Training Council sanctioned classes in the state of Michigan only. Microsoft Word, Copyright © Microsoft Corporation Microsoft Powerpoint, Copyright © Microsoft Corporation Adobe Pagemaker, Copyright © Adobe Systems Incorporated Adobe Acrobat, Copyright © Adobe Systems Incorporated Corel Draw, Copyright © Corel Corporation Corel Paint, Copyright © Corel Corporation Student Guide 3 Vehicle Extrication Rev. 03/01/01 Blank Page Student Guide 4 Vehicle Extrication Rev. 03/01/01 Preface The developer's of this course would like to thank you for participating, This course was designed to help you, the extrication team, stay current with the latest developments in vehicle construction and technology. Through continued education in this field, we can truly help to save more lives then those of yesterday. We strongly encourage you to take this guide and make suggestions to further its' development. Through your participation, this course can only get better. Staff: Raymond Haring Chief Elmwood Township -

“Is Anyone Pinned (Trapped)?” During Motor Vehicle
International Academies of Emergency Dispatch EMERGENCY DISPATCH RESEARCH AT WORK RESEARCH BRIEF A “YES” ANSWER TO THE PROTOCOL SHOULD WE ASK CALLERS KEY QUESTION “IS “IS ANYONE PINNED ANYONE PINNED (TRAPPED)?” IS A (TRAPPED)?” DURING MOTOR BETTER PREDICTOR OF EXTRICATION BY VEHICLE ACCIDENTS (MVAs)? RESPONDERS FOR We should! The question directs callers to pay MVAs THAN THE PRESENCE OF SEMI- attention to what matters most. TRUCK OR HEAD- ON MECHANISM. What is Extrication?: For a traffic collision, the higher the speed of the vehicle, the higher the chances an occupant suffers severe injuries.1 After a serious crash, the absorbed kinetic energy can cause the vehicle to deform significantly, displacing parts of the vehicle into the interior. This displacement frequently limits an occupant’s ability to move or be removed. When there is need for extrication, deformity and damage hinder an occupant’s safe exit or removal. The primary focus of most vehicle extrication operations is to remove the entanglement from around an occupant, not an occupant from the entanglement. Extrication of an No Time to Lose occupant from a damaged vehicle can be accomplished several ways dependent on the extent and nature of the damage and the urgency of an occupant’s removal. Some vehicle extrication operations require removal of the roof and doors. Other operations require forced hydraulic movement of interior vehicle parts to create room around an occupant. Vehicle extrication can be technically challenging and time-consuming, requiring multiple personnel, specialized equipment, and occasionally, extended periods of time to achieve the desired safe outcome.2 50% Identifying the need for extrication during a Motor Vehicle Accident (MVA) is very important. -

Victim Disentanglement and Extrication
Victim Disentanglement and Extrication Chapter Contents Victim Entrapment ............................279 Chapter Review .............................. 308 Victim Locations ....................................................... 279 Discussion Questions ....................... 308 Points of Entrapment ............................................... 280 Skill Sheets ................................... 309 Dynamics of Disentanglement ................................. 281 Multiple Vehicle Incidents ........................................ 285 Minimizing Hazards to Victims ................................. 287 Passenger Vehicle Access and Egress Points ............................287 Passenger Vehicle Access and Egress Routes ......... 288 Passenger Vehicle Entry Points ............................... 288 Passenger Vehicle Disentanglement and Extrication Operations ................. 290 Techniques for Creating Access and Egress Openings on Passenger Vehicles ............................................... 290 Alternative Techniques for Creating Access and Egress Openings on Passenger Vehicles with Advanced Steel ............................................. 301 Techniques for Disentangling Victims from Passenger Vehicles .............................................. 303 276 Section C • Chapter 8 – Victim Disentanglement and Extrication Victim Disentanglement and Extrication Key Terms 8 Access ......................................................288 Disentanglement .....................................279 Egress .......................................................288 -

Vehicle Extrication Passenger Safety Systems
VEHICLE EXTRICATION Extrication operations on today’s vehicles are significantly different and more dangerous than what we have faced in the past. The government is requiring that auto makers adhere to tougher, more stringent safety standards. These safety standards increase the survivability of passengers that have been involved in an accident, at the same time we are finding that the vehicles manufactured to these newer standards are presenting us with tougher challenges. These vehicles are now being armed with multiple airbags that are controlled by smart computer system which can be extremely dangerous to rescuers and patients during extrication operations. Firefighters will also find that automakers are using more exotic metals to strengthen and reinforce vital structural components. In the past, we have gone to the scene of an extrication knowing that our tools, regardless of the brand, could cut through any vehicle we came up against. Today, however, because of these stronger, more lightweight metals, the tools that we have relied on in the past are having a tougher time cutting through and spreading these metals. Never before has it been so important to understand the capabilities and limitations of our rescue tools. Rescuers will have to find alternative techniques and tools to achieve the same results as in the past. Understanding how vehicles are constructed and knowing what they are constructed of, will allow us to make better decisions on scene Rescuers must also understand that the auto makers are constantly improving on the designs of their safety systems. These changes are happening so quickly, that it would be safe to say that by the time this chapter and volume are published, the material you are reading will outdated. -

Emergency Response Guide
INFORMATION FOR FIRST AND SECOND RESPONDERS EMERGENCY RESPONSE GUIDE TESLA MODEL Y ELECTRIC VERSION: 001 CONTENTS 0. Emergency Response Sheet Page 1 1. Identification / recognition Page 2 2. Immobilization / stabilization / lifting Page 5 3. Disable direct hazards / safety regulations Page 7 4. Access to the occupants Page 12 5. Stored energy / liquids / gases / solids Page 19 6. In case of fire Page 23 7. In case of submersion Page 25 8. Towing / transportation / storage Page 26 9. Important additional information Page 28 10. Explanation pictograms used Page 29 Model Y Emergency Response Guide TESLA MODEL Y From 2020—Present Stored gas Seatbelt SRS Con- Pedestrian Airbag inflator preten- trol Unit protection sioner active system Automatic Gas strut/ High Zone rollover pre-loaded strength requiring protection spring zone special system attention Battery Ultra ca- Fuel tank Gas tank Safety low volt- pacitor, low valve age voltage High High volt- High Fuse box Ultra voltage age power voltage disabling capaci- battery cable/com- discon- high tor, high pack ponent nect voltage voltage system Cable cut TESLA MODEL Y ID No. Version No. From 2020 — present TESLA-202012-001 01 1. Identification / recognition WARNING LACK OF ENGINE NOISE DOES NOT MEAN VEHICLE IS OFF. SILENT MOVEMENT OR INSTANT RESTART CAPABILITY EXISTS UNTIL VEHICLE IS FULLY SHUT DOWN. WEAR APPROPRIATE PERSONAL PROTECTIVE EQUIPMENT (PPE). Badging and Door Handles Model Y can be identified by its badges and uniquely shaped door handles. The model name does not appear on the rear of the vehicle. NOTE: Model Y may have a “DUAL MOTOR” badge on the trunk to indicate that it is a dual motor configuration.