Of 112 Minutes of the Meeting of the Pharmacy Practices Committee
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Old Smiddy CLIFTON • MID CALDER • WEST LOTHIAN • EH53 0HT Charming Traditional Cottage with Fantastic Views Over Open Countryside
The Old Smiddy CLIFTON • MID CALDER • WEST LOTHIAN • EH53 0HT Charming traditional cottage with fantastic views over open countryside Entrance hall u drawing room u dining room u kitchen shower room u WC u three bedrooms Two further bedrooms u family room u study Garage u conservatory u garden About 0.5 acres in all EPC Rating = F Edinburgh Airport 4.7 miles, Edinburgh city bypass 5.7 miles, Edinburgh city centre 10 miles Viewing Strictly by appointment with Savills Edinburgh 0131 247 3700. Directions From Edinburgh take the A8 to Newbridge. Leave the Newbridge Roundabout on the Old Liston Road and, immediately after the service station and McDonald’s restaurant, turn left onto Cliftonhall Road (B7030). Follow the road under the motorway and under the canal. Take the second right onto Clifton Road, after passing the Edinburgh International Climbing Arena on the left. The Old Smiddy is the first property on the right, approximately 300m down the road, partially hidden from view by a coppice. Situation Set in a lovely rural location, near to the picturesque River Almond, The Old Smiddy is surrounded by open countryside, yet has the benefit of being close to ideal transport links for commuting to Edinburgh or Glasgow. The nearby train stations of Kirknewton and Uphall provide excellent commuter train services and the property is also extremely well placed for commuting to both Edinburgh and Glasgow, via the A71 and M8/M9 motorway network. Furthermore, the nearby villages of East Calder and Mid Calder have a good local bus service linking the area with Edinburgh, Livingston and Bathgate. -
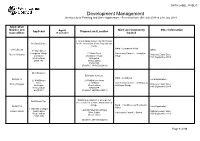
Development Management Weekly List of Planning and Other Applications - Received from 15Th July 2019 to 21St July 2019
DATA LABEL: PUBLIC Development Management Weekly List of Planning and Other Applications - Received from 15th July 2019 to 21st July 2019 Application Number and Ward and Community Other Information Applicant Agent Proposal and Location Case officer (if applicable) Council Listed building consent for alterations Mr Gary Corbett for the conversion of two flats into one house . Ward :- Livingston North 0381/LBC/19 Other 11 Main Street Livingston Village 11 Main Street Community Council :- Livingston Steven McLaren Statutory Expiry Date: Livingston Livingston Village Village 16th September 2019 West Lothian Livingston EH54 7AF West Lothian EH54 7AF (Grid Ref: 303835,666892) Mr A McLaren Extension to house. Ward :- Linlithgow 0408/H/19 Local Application 27 Kettil'stoun 27 Kettil'stoun Grove Grove Linlithgow Community Council :- Linlithgow & Nancy Douglas Statutory Expiry Date: Linlithgow West Lothian Linlithgow Bridge 14th September 2019 West Lothian EH49 6PP EH49 6PP (Grid Ref: 298996,676214) Planning permission in principle for Mr Richard Rae the erection of a house and detached garage. Ward :- Fauldhouse & The Breich 0425/P/19 Local Application Valley 1 Pateshill Cottages Land At Pateshill Cottages Gillian Cyphus West Calder Statutory Expiry Date: West Calder Community Council :- Breich West Lothian 15th September 2019 West Lothian EH55 8NS (Grid Ref: 298458,660284) Page 1 of 10 Shiraz Riaz Installation of UPVC windows, Mr Steven Bull Everest Limited replacement door and formation of decking. 0601/H/19 Everest House Ward :- Armadale & Blackridge Local Application 12 Craigs Court Sopers Road 12 Craigs Court Nancy Douglas Torphichen Cuffley Community Council :- Torphichen Statutory Expiry Date: Torphichen West Lothian Potters Bar 18th September 2019 West Lothian EH48 4NU Hertfordshire EH48 4NU EN6 4SG (Grid Ref: 297047,672165) Mr Steven McMillan Installation of a 7m high amateur radio mast (in retrospect). -

24 25 TT Bklt
24 25 N25 including service 20 on Sunday morning Blackridge and Armadale – Edinburgh Serving: Bathgate (25) Deans Eliburn (24) Livingston Pumpherston (24) Uphall Broxburn Ratho Station Corstophine Bus times from 28 October 2019 Welcome aboard! Operating many bus routes throughout Central Scotland and West Lothian that are designed to make your journey as simple as possible. Thank you for choosing to travel with First. • Route Page 12-13 • Timetables Pages 3-11, 14-23 • Customer services Back Page Your latest timetable updates: Revised timetable early mornings and evenings. Value for money! Here are some of the ways we can save you money and speed up your journey: FirstDay – enjoy unlimited journeys all day in your chosen zone. FirstWeek – enjoy unlimited journeys all week in your chosen zone. Contactless – seamless payment to speed up journey times. First Bus App – purchase and store tickets on your mobile phone with our free app. Plan your journey in advance and track your next bus. 3+ Zone – travel all week throughout our network for £25 with our 3+ Zone Weekly Ticket. Find out more at firstscotlandeast.com Correct at the time of printing. GET A DOWNLOAD OF THIS. NEWNEW Download the new First Bus App to plan EASYEAASSY journeys and buy tickets all in one place. APPAPP TECH THE BUS WITH LESS FUSS 24 – Deans – Livingston – Edinburgh 24 25 25 – Blackridge – Livingston – Edinburgh Mondays to Fridays Service Number 25 24 25 25 24 25 25 24 25 25 24 25 25 24 25 25 24 25 Blackridge Terminus — — — — — — — — — — — — — — 0639 — — 0717 Armadale, -

Pdf X22, X23 Shotts
X22 X23 Shotts - Edinburgh Serving: Harthill (X22 ) Whitburn (X22 ) Blackburn (X22 ) Deans (X23 ) Eliburn (X23 ) Livingston Dedridge East Mid Calder East Calder Hermiston Park & Ride Bus times from 27 January 2020 GET A DOWNLOAD OF THIS. NEW EASY APP THE NEW FIRST BUS APP IS THE SMARTER WAY TO GET WHERE YOU’RE GOING. IT’S HERE TO HELP WITH EVERY PART OF YOUR JOURNEY. Real-time bus updates and simple, secure mTicket purchasing on the new First Bus App mean you can be on your way even quicker. Simply download the Running late? No problem! The First Bus App, and you’ll be First Bus App also lets you know able to securely buy and store when your next bus is arriving. tickets on your phone. You Simply hop on board, pay using never have to worry about your First Bus App, contactless losing your pass or forgetting card, Apple Pay or Google Pay, your change again! and you’re ready to go! TECH THE BUS WITH LESS FUSS Thanks for choosing to travel with First. Our gu ide will help you plan your next bus journey or for more information visit: www.firstscotlandeast.com Customer Services 0345 646 0707 (Mon-Fri 7am-7pm & weekends 9am-5pm) @FirstScotland FirstScotlandEast Carmuirs House, 300 Stirling Road, Larbert, FK5 3NJ A ch o ice of tickets We offer a range of tickets to suit your travelling needs. As well a s singles and returns , we have tickets offering unlimited travel such as First Day , First Week , First 4Week and First Year . Contact our Customer Services team for more information. -

East Calder & District Community Council Meeting East Calder
East Calder & District Community Council Meeting East Calder Partnership Centre Tuesday 1 May 2018 Declarations of Conflict of Interest - None Present - David Philip, Chris Davidson, Janet Davidson, Morag Lyall, Caroline Wright, David Ogg, Kenny Ireland Attending - Jayne Murphy (Resident), PC Alan Murray, Councillor Carl John & Councillor Dave King, Alan Wright Apologies - Ray Kirk, Damien Timson, Neil Lovett Matters Arising - Litter Pick - Postpone till later in the year. April Minutes - Proposed Kenny Ireland, Seconded David Ogg Minutes for Website - Alan Wright requested minutes to be uploaded to Website. Minutes for Library - David Philip received request for Previous copies of minutes to be held in library. David Philip and Chris Davidson attended the West Lothian Council session - 34 Community Council's are rebranding the previously known The Association. David Philip has been elected as Office Bearer. Angus McKinness (Police Superintendent) will be the chair person. Chris Davidson advised that Lorraine McGroarty, West Lothian Council will send out slides from the Sessions in due course to all Community Councils. It is hoped by creating the community council's we can all share the common issues - ongoing transport, roads, planning, infrastructure, asset transfer, funding. Public Requests to the NHS Chamber of Commerce have 30 days to respond. Mid Calder and Pumpherston Community Council's - David Philip confirmed that the contacts are Eleanor Blair (Mid Calder) and Sharon Gibson (Pumpherston). Craigsfarm Community Development Project - Facebook. Health centre. Dog Fouling - Councillor King advised that the council no longer supply bins for dogs this should be disposed of in the normal bins. Household Waste - David Philip gave an update West Lothian Council were experiencing issues with garden waste however are now catching up. -

The Mineral Resources of the Lothians
The mineral resources of the Lothians Information Services Internal Report IR/04/017 BRITISH GEOLOGICAL SURVEY INTERNAL REPORT IR/04/017 The mineral resources of the Lothians by A.G. MacGregor Selected documents from the BGS Archives No. 11. Formerly issued as Wartime pamphlet No. 45 in 1945. The original typescript was keyed by Jan Fraser, selected, edited and produced by R.P. McIntosh. The National Grid and other Ordnance Survey data are used with the permission of the Controller of Her Majesty’s Stationery Office. Ordnance Survey licence number GD 272191/1999 Key words Scotland Mineral Resources Lothians . Bibliographical reference MacGregor, A.G. The mineral resources of the Lothians BGS INTERNAL REPORT IR/04/017 . © NERC 2004 Keyworth, Nottingham British Geological Survey 2004 BRITISH GEOLOGICAL SURVEY The full range of Survey publications is available from the BGS Keyworth, Nottingham NG12 5GG Sales Desks at Nottingham and Edinburgh; see contact details 0115-936 3241 Fax 0115-936 3488 below or shop online at www.thebgs.co.uk e-mail: [email protected] The London Information Office maintains a reference collection www.bgs.ac.uk of BGS publications including maps for consultation. Shop online at: www.thebgs.co.uk The Survey publishes an annual catalogue of its maps and other publications; this catalogue is available from any of the BGS Sales Murchison House, West Mains Road, Edinburgh EH9 3LA Desks. 0131-667 1000 Fax 0131-668 2683 The British Geological Survey carries out the geological survey of e-mail: [email protected] Great Britain and Northern Ireland (the latter as an agency service for the government of Northern Ireland), and of the London Information Office at the Natural History Museum surrounding continental shelf, as well as its basic research (Earth Galleries), Exhibition Road, South Kensington, London projects. -

276 Bus Time Schedule & Line Route
276 bus time schedule & line map 276 Bathgate View In Website Mode The 276 bus line (Bathgate) has 4 routes. For regular weekdays, their operation hours are: (1) Bathgate: 5:20 AM - 5:07 PM (2) Broxburn: 6:07 AM - 10:32 PM (3) Livingston: 10:30 PM (4) Loganlea: 6:37 AM - 9:30 PM Use the Moovit App to ƒnd the closest 276 bus station near you and ƒnd out when is the next 276 bus arriving. Direction: Bathgate 276 bus Time Schedule 81 stops Bathgate Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 5:20 AM - 5:07 PM Dunnet Way, Broxburn Hunter Gardens, Broxburn Tuesday 5:20 AM - 5:07 PM Thistle Business Park, Broxburn Wednesday 5:20 AM - 5:07 PM Aitken Orr Drive, Broxburn Thursday 5:20 AM - 5:07 PM East Main Street, Broxburn Friday 5:20 AM - 5:07 PM Aitken Orr Drive, Broxburn Saturday 7:07 AM - 5:07 PM Church Street, Broxburn 91-95 East Main Street, Broxburn Post O∆ce, Broxburn 276 bus Info Direction: Bathgate New Holygate, Broxburn Stops: 81 New Holygate, Broxburn Trip Duration: 84 min Line Summary: Dunnet Way, Broxburn, Thistle Kirkhill Road, Broxburn Business Park, Broxburn, Aitken Orr Drive, Broxburn, Aitken Orr Drive, Broxburn, Church Street, Broxburn, Cardross Road, Broxburn Post O∆ce, Broxburn, New Holygate, Broxburn, West Main Street, Broxburn Kirkhill Road, Broxburn, Cardross Road, Broxburn, Cardross Road, Broxburn, Freeland Avenue, Cardross Road, Broxburn Broxburn, Cemetery, Uphall, Alexander Street, Uphall, Oatridge Hotel, Uphall, St Andrews Drive, Uphall, Freeland Avenue, Broxburn Millbank Place, Uphall, Stankards -
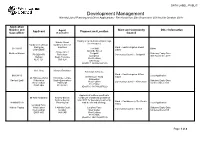
Development Management Weekly List of Planning and Other Applications - Received from 30Th September 2019 to 6Th October 2019
DATA LABEL: PUBLIC Development Management Weekly List of Planning and Other Applications - Received from 30th September 2019 to 6th October 2019 Application Number and Ward and Community Other Information Applicant Agent Proposal and Location Case officer (if applicable) Council Display of an illuminated fascia sign Natalie Gaunt (in retrospect). Cardtronics UK Ltd, Cardtronic Service trading as Solutions Ward :- East Livingston & East 0877/A/19 The Mall Other CASHZONE Calder Adelaide Street 0 Hope Street Matthew Watson Craigshill Statutory Expiry Date: PO BOX 476 Rotherham Community Council :- Craigshill Livingston 30th November 2019 Hatfield South Yorkshire West Lothian AL10 1DT S60 1LH EH54 5DZ (Grid Ref: 306586,668165) Ms L Gray Maxwell Davidson Extenison to house. Ward :- East Livingston & East 0880/H/19 Local Application 20 Hillhouse Wynd Calder 20 Hillhouse Wynd 19 Echline Terrace Kirknewton Rachael Lyall Kirknewton South Queensferry Statutory Expiry Date: West Lothian Community Council :- Kirknewton West Lothian Edinburgh 1st December 2019 EH27 8BU EH27 8BU EH30 9XH (Grid Ref: 311789,667322) Approval of matters specified in Mr Allan Middleton Andrew Bennie conditions of planning permission Andrew Bennie 0462/P/17 for boundary treatments, Ward :- Fauldhouse & The Breich 0899/MSC/19 Planning Ltd road details and drainage. Local Application Valley Longford Farm Mahlon Fautua West Calder 3 Abbotts Court Longford Farm Statutory Expiry Date: Community Council :- Breich West Lothian Dullatur West Calder 1st December 2019 EH55 8NS G68 0AP West Lothian EH55 8NS (Grid Ref: 298174,660738) Page 1 of 8 Approval of matters specified in conditions of planning permission G and L Alastair Nicol 0843/P/18 for the erection of 6 Investments EKJN Architects glamping pods, decking/walkway 0909/MSC/19 waste water tank, landscaping and Ward :- Linlithgow Local Application Duntarvie Castle Bryerton House associated works. -
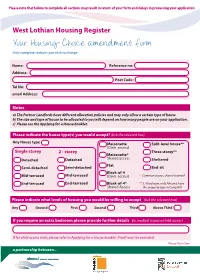
Housing Choice Amendment Form Only Complete Sections You Wish to Change
Please note that failure to complete all sections may result in return of your form and delays in processing your application West Lothian Housing Register Your Housing Choice amendment form Only complete sections you wish to change Name: Reference no: Address: Post Code: Tel No: email Address: Notes a) The Partner Landlords have different allocation policies and may only allow a certain type of house b) The size and type of house to be allocated to you will depend on how many people are on your application. c) Please see the Applying for a House Booklet. Please indicate the house type(s) you would accept? (tick the relevant box) Any House type Maisonette Split-level house** (Own access) Single storey 2 - storey Three storey** Maisonette* Detached Detached Shared access Sheltered Flat Semi-detached Semi-detached Bed-sit Block-of-4 Mid-terraced Mid-terraced (Own access) * Common access, shared stairwell End-terraced End-terraced Block-of-4* ** 3, 4 bedroom, only Almond have Shared Access this property type in Craigshill Please indicate what levels of housing you would be willing to accept (tick the relevant box) Any Ground First Second Third Above Third If you require an extra bedroom please provide further details (ie medical reasons/child access) If for child access visits, please refer to Applying for a House booklet. Proof must be provided Please Turn Over a partnership between... What heating type would you accept? (tick the relevant box) Any Gas Electric Coal Please tick the areas below for which you would wish to be considered Any -

X24 Bus Time Schedule & Line Route
X24 bus time schedule & line map X24 Deans - Edinburgh View In Website Mode The X24 bus line (Deans - Edinburgh) has 4 routes. For regular weekdays, their operation hours are: (1) Broxburn: 4:57 PM - 5:27 PM (2) Deans: 6:36 AM - 9:26 PM (3) Edinburgh: 5:27 AM - 9:13 PM (4) Uphall: 5:54 PM Use the Moovit App to ƒnd the closest X24 bus station near you and ƒnd out when is the next X24 bus arriving. Direction: Broxburn X24 bus Time Schedule 45 stops Broxburn Route Timetable: VIEW LINE SCHEDULE Sunday 9:37 AM - 10:22 PM Monday 4:57 PM - 5:27 PM Nu Moves Dance Studios, Deans Tuesday 4:57 PM - 5:27 PM Burnsknowe, Deans Wednesday 4:57 PM - 5:27 PM Meldrum Primary School, Deans Thursday 4:57 PM - 5:27 PM Deans North Road, Livingston Friday 4:57 PM - 5:27 PM Jubilee Avenue, Deans 70 Kenmore Avenue, Livingston Saturday 4:57 PM - 5:37 PM Masonic Lodge, Deans Deans Primary School, Deans Deans South, Livingston X24 bus Info Direction: Broxburn Muirƒeld Way, Deans Stops: 45 Roseberry Park, Livingston Trip Duration: 51 min Line Summary: Nu Moves Dance Studios, Deans, Lochshot Place, Eliburn Burnsknowe, Deans, Meldrum Primary School, 3 Lochshot Place, Livingston Deans, Jubilee Avenue, Deans, Masonic Lodge, Deans, Deans Primary School, Deans, Muirƒeld Way, Kilne Place, Eliburn Deans, Lochshot Place, Eliburn, Kilne Place, Eliburn, 1 Longpark Place, Livingston Oldwood Place, Eliburn, Lady Place, Eliburn, Gavin Place, Eliburn, Peel Roundabout, Eliburn, Braehead Oldwood Place, Eliburn Junction, Howden, Quarrywood Court, Livingston, 208 Oldwood Place, Livingston -

Out in the Open Citation for Published Version: Moore, D 2012, out in the Open: Paraffin Harvester
Edinburgh Research Explorer Out In The Open Citation for published version: Moore, D 2012, Out In The Open: Paraffin Harvester. in Out in the Open: public Art in West Lothian. 1 edn, vol. 1, West Lothian Council Community Arts, Scotland, pp. Images pages pp. 11 and 48. Works cited pp. 18 and 43, Quotatation p. 33. Feature p. 49 and Acknowlegements p. 95. <http://lmmscache1.server.westlothian.gov.uk/media/downloaddoc/1799441/2195888/Out_in_the_Open_Pu blic_Art_book> Link: Link to publication record in Edinburgh Research Explorer Document Version: Publisher's PDF, also known as Version of record Published In: Out in the Open Publisher Rights Statement: © Moore, D. (2012). Out In The Open: Paraffin Harvester. In Out in the Open. West Lothian Council, Scotland. General rights Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 10. Oct. 2021 PUBLIC ART IN Firth of Forth M9 Harperrig VISITING PUBLIC ART IN WEST LOTHIAN Reservoir WEST LOTHIAN Rd 4 Each public art piece in this publication tells a story about the place in which it 3 A706 Grange A803 Blackness stands. -

East Livingston and East Calder
West Lothian Council Area Ward Performance Report Quarter 4 2018/19 East Livingston and East Calder DISCLAIMER The figures included in this report are provisional and subject to change as a result of quality assurance and review. The statistics quoted are internal management information published in the interests of transparency and openness. The Scottish government publishes Official Statistics each year which allow for comparisons to be made over longer periods of time. Please ensure any external partners in receipt of these reports are aware of this. Accidental Dwelling Fires Per 10,000 head of population 5.0 Introduction 4.0 Welcome to the Scottish Fire and Rescue Service Ward Performance Report. This 3.0 performance report is designed to provide citizens, stakeholders and partners with information relating to ward based activity undertaken by the Scottish Fire and Rescue 2.0 Service. 1.0 In addition to historical ward based activity, this performance report provides information 0.0 on the historic activity in the West Lothian Council area and Scotland. To allow benchmarking to be undertaken, the units of measurement in the performance graphs in the report are based on incidents/events per head of population. Whilst using historic statistical benchmarking data, consideration must be taken of the somewhat random nature of fire related incidents and events, and how this can pose difficulties in interpreting emerging patterns and trends. This is of specific relevance where ward level data is analysed due to the relatively small number of actual incidents/events that occur in ward areas. However, regardless of statistical anomalies, emerging patterns and trends in fire related Fire Casualties and Fatalaties Per 1,000,000 head of population incidents and events can assist the Scottish Fire and Rescue Service and Community 120 Planning Partners plan and implement preventative intervention initiatives to target 100 reducing fire related incidents and events.