Hypersensitivity Pneumonitis and Metalworking Fluids Contaminated by Mycobacteria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Obliterative Bronchiolitis, Cryptogenic Organising Pneumonitis and Bronchiolitis Obliterans Organizing Pneumonia: Three Names for Two Different Conditions
Eur Reaplr J EDITORIAL 1991, 4, 774-775 Obliterative bronchiolitis, cryptogenic organising pneumonitis and bronchiolitis obliterans organizing pneumonia: three names for two different conditions R.M. du Bois, O.M. Geddes Over the last five years, increasing confusion has has been applied to conditions in which airflow obstruc developed over the use of the terms "bronchiolitis tion is prominent and in which response to treatment is obliterans" and "bronchiolitis obliterans organizing poor. pneumonia". The confusion stems largely from the common use of the term "bronchiolitis obliterans" or "obliterative bronchiolitis" in the diagnostic labels applied "Cryptogenic organizing pneumonitis" or "bronchi· to two entities which are quite distinct clinically but which otitis obliterans organizing pneumonia" (BOOP) bear certain resemblances histologically. Cryptogenic organizing pneumonitis was first described by DAVISON et al. [7] in 1983. The clinical syndrome ObUterative bronchiolitis consisted of breathlessness, malaise, fever, high erythrocyte sedimentation rate (ESR), pneumonic In 1977, GEODES et al. [1] reported the case histories shadowing on chest radiograph with a restrictive of six patients whose clinical condition was characterized pulmonary function defect and low gas transfer coeffi by airways obliteration in association with rheumatoid cient. On histological examination of lung biopsy mate· arthritis. The striking clinical features were of rapidly rial, the typical and distinguishing feature was the progressive breathlessness and the fmding on examination presence of connective tissue within the alveoli, alveolar of a high-pitched mid-inspiratory squeak heard over the ducts and, occasionally, in respiratory bronchioles. This lung fields. Chest radiographs showed hyperinflated lungs connective tissue consisted of "loosely woven fibres of but were otherwise normal. -

Pneumonitis, Pleural Effusion and Pericarditis Following Treatment with Dantrolene
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.47.5.553 on 1 May 1984. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry 1984;47:553-554 Short report Pneumonitis, pleural effusion and pericarditis following treatment with dantrolene DH MILLER, LF HAAS From the Neurology Department, Wellington Hospital, Wellington, New Zealand SUMMARY A patient developed pulmonary infiltration, pleural effusions and pericarditis three months after starting dantrolene sodium. Peripheral blood eosinophilia and a raised ESR were present. Symptoms and signs resolved after the drug was discontinued. Dantrolene toxicity should be considered in the differential diagnosis of pneumonitis and pleuro-pericarditis. Use of dantrolene sodium (dantrium) to lessen spas- ticity can be limited by hepatic toxicity.' There has also been one report of potentially serious pleuro- pericardial reactions.2 We describe a further case Protected by copyright. with pulmonary parenchymal involvement in addi- tion to pleuro-pericardial reaction. Case report A 43-year-old female suffered from multiple sclerosis since 1973. By January 1983 she had bilateral optic atro- __- t- w..Ssu phy, horizontal and vertical nystagmus, incoordination of the upper limbs, marked spasticity and weakness of the >Ss _1v' <*t. -1|1 iikkx. lower limbs with frequent painful spasms. Baclofen 80 f. ; ............. ,.: | ee: combined with ... :' ::' mg/day physiotherapy made little differ- .... ence to her spasticity or spasms. Dantrolene was then a. introduced in late January 1983, increasing to 100 mg qid. j Chest radiograph prior to treatment was normal. Two months after starting dantrolene pleuritic pains in the left shoulder and chest occurred without other respiratory symptoms. Temperature was 38 2°C. -

Radiation-Induced Pneumonitis in the Era of the COVID-19 Pandemic: Artificial Intelligence for Differential Diagnosis
cancers Article Radiation-Induced Pneumonitis in the Era of the COVID-19 Pandemic: Artificial Intelligence for Differential Diagnosis Francesco Maria Giordano 1,† , Edy Ippolito 2,†, Carlo Cosimo Quattrocchi 1,*, Carlo Greco 2, Carlo Augusto Mallio 1 , Bianca Santo 2, Pasquale D’Alessio 1 , Pierfilippo Crucitti 3 , Michele Fiore 2 , Bruno Beomonte Zobel 1 , Rolando Maria D’Angelillo 4 and Sara Ramella 2 1 Departmental Faculty of Medicine and Surgery, Diagnostic Imaging and Interventional Radiology, Università Campus Bio-Medico di Roma, 00128 Rome, Italy; [email protected] (F.M.G.); [email protected] (C.A.M.); [email protected] (P.D.); [email protected] (B.B.Z.) 2 Departmental Faculty of Medicine and Surgery, Radiation Oncology, Università Campus Bio-Medico di Roma, 00128 Rome, Italy; [email protected] (E.I.); [email protected] (C.G.); [email protected] (B.S.); m.fi[email protected] (M.F.); [email protected] (S.R.) 3 Departmental Faculty of Medicine and Surgery, Thoracic Surgery, Università Campus Bio-Medico di Roma, 00128 Rome, Italy; [email protected] 4 Departmental Faculty of Medicine and Surgery, Radiation Oncology, Università degli Studi Tor Vergata, 00133 Rome, Italy; [email protected] * Correspondence: [email protected]; Tel.: +39-06225411708 † These authors contributed equally to this manuscript. Simple Summary: Radiation-induced pneumonitis and severe acute respiratory syndrome coron- Citation: Giordano, F.M.; Ippolito, E.; avirus 2 (SARS-CoV-2) interstitial pneumonia show overlapping clinical features. As we are facing Quattrocchi, C.C.; Greco, C.; Mallio, the COVID-19 pandemic, the discrimination between these two entities is of paramount importance. -
The Use of Aerodynamic Analysis in the Diagnosis of Adults with Paradoxical Vocal Cord Dysfunction
THE USE OF AERODYNAMIC ANALYSIS IN THE DIAGNOSIS OF ADULTS WITH PARADOXICAL VOCAL CORD DYSFUNCTION DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Kathleen Mary Treole, M.A. The Ohio State University 1996 Dissertation Committee: Approved by Professor Michael D. Trudeau, Adviser \jL nA Professor Janet M. Weisenberger Adviser Department of Professor Jessica R. Harris Speech and Hearing Science UMI Number: 9639361 Copyright 1996 by Treole, Kathleen Mary All rights reserved. UMI Microform 9639361 Copyright 1996, by UMI Company. All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code. UMI 300 North Zeeb Road Ann Arbor, MI 48103 ABSTRACT 50 adults with paradoxical vocal cord dysfunction (PVCD) and 50 adult, laryngeally normal adults control subjects were evaluated to determine which of 26 aerodynamic measurements in a clinical protocol differentiated the groups. Videolaryngostroboscopy (VLS) was performed on persons suspected of having PVCD to confirm the presence of abnormal vocal fold adduction and to determine if laryngeal lesion or abnormality (other than PVCD) contributed to the presentation of symptoms. Control subjects were examined via VLS to ensure structural and functional integrity of the larynx. The aerodynamic protocol included the following measures: vital capacity, phonatory volumes, mean flow of sustained phonemes (/a, s, z ,/), mean durations of sustained phonemes, rapid syllable repetitions (/a, ha/), spikes of flow during connected speech (reading, counting), cessations of flow during sustained phoneme tasks, and ratios of tasks (s/z, ha/a). The following measurements demonstrated a group effect in which control subjects demonstrated higher mean values than did subjects with PVCD: volumes, durations, and mean peak flow of /a/ and /ha/ repetitions. -

Simultaneous Bilateral Spontaneous Pneumothorax and Radiation Pneumonitis Following Thoracic Radiotherapy for the Treatment of High Grade Follicular Lymphoma
J Case Rep Images Oncology 2018;4:100050Z10DM2018. Mudawi et al. 1 www.edoriumjournals.com/case-reports/jcro CCASEASE REPORT PEER REVIEWED OPE| OPEN NACCESS ACCESS Simultaneous bilateral spontaneous pneumothorax and radiation pneumonitis following thoracic radiotherapy for the treatment of high grade follicular lymphoma Dalia Mudawi, George Antunes, Rajesh Mamadigi ABSTRACT He received intensive chemotherapy comprising of rituximab, cyclophosphamide, doxorubicin, Introduction: Spontaneous pneumothorax is vincristine and prednisolone (R-CHOP) a potentially life-threatening condition but and intrathecal methotrexate. He received an under-recognised and rarely described consolidation radiotherapy totalling 30Gy over complication of thoracic radiotherapy. 15 fractions to the thoracic spine at levels T2- We report a case of bilateral spontaneous T4 and left humerus. The patient presented to pneumothoraces and radiation pneumonitis secondary care within eight weeks of completing following moderate dose of thoracic radiation thoracic radiotherapy complaining of worsening to the spine for high grade follicular lymphoma. dyspnoea on exertion. Arterial blood gas Case Report: A 66-year-old Caucasian male, analysis confirmed hypoxemic respiratory non-smoker and no pre-existing pulmonary failure and computed tomography (CT) scan pathology, was diagnosed with low grade of the thorax demonstrated bilateral small follicular lymphoma in 1999 and treated with to moderate sized pneumothoraces, bilateral chlorambucil and dexamethasone, followed by patchy ground glass opacification suggestive 30Gy radiotherapy to para-aortic lymph nodes. of radiation pneumonitis, and atelectasis. A subsequent relapse in 2005 was treated The patient was started on a tapering course with a further eight cycles of chlorambucil of high dose systemic corticosteroids leading and dexamethasone followed by radiotherapy to a rapid improvement in clinical symptoms to the pelvis. -
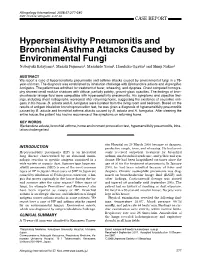
Hypersensitivity Pneumonitis and Bronchial Asthma Attacks Caused
Allergology International. 2008;57:277-280 ! DOI: 10.2332 allergolint. C-07-56 CASE REPORT Hypersensitivity Pneumonitis and Bronchial Asthma Attacks Caused by Environmental Fungi Nobuyuki Katayama1, Masaki Fujimura1, Masahide Yasui1, Haruhiko Ogawa1 and Shinji Nakao1 ABSTRACT We report a case of hypersensitivity pneumonitis and asthma attacks caused by environmental fungi in a 75- year-old man. The diagnosis was established by inhalation challenge with Bjerkandera adusta and Aspergillus fumigatus. The patient was admitted for treatment of fever, wheezing, and dyspnea. Chest computed tomogra- phy showed small nodular shadows with diffuse, partially patchy, ground-glass opacities. The findings of bron- choalveolar lavage fluid were compatible with hypersensitivity pneumonitis. His symptoms and objective find- ings, including chest radiographs, worsened after returning home, suggesting the existence of causative anti- gens in his house. B. adusta and A. fumigatus were isolated from the living room and bedroom. Based on the results of antigen inhalation bronchoprovocation test, he was given a diagnosis of hypersensitivity pneumonitis caused by B. adusta and bronchial asthma attacks caused by B. adusta and A. fumigatus. After cleaning the entire house, the patient has had no recurrence of the symptoms on returning home. KEY WORDS Bjerkandera adusta, bronchial asthma, home environment provocation test, hypersensitivity pneumonitis, inha- lation challenge test sity Hospital on 29 March 2006 because of dyspnea, INTRODUCTION productive cough, fever, and wheezing. He had previ- Hypersensitivity pneumonia (HP) is an interstitial ously received outpatient treatment for bronchial lung disease characterized by an abnormal immu- asthma, sinobronchial syndrome, and yellow nail syn- nologic reaction to specific antigens contained in a drome. -

Pleural Effusion Associated with Pegylated Interferon Alpha and Ribavirin Treatment for Chronic Hepatitis C
CASE REPORT Pleural Effusion Associated with Pegylated Interferon Alpha and Ribavirin Treatment for Chronic Hepatitis C Amit Arora1 1 Department of Medicine, NorthShore University HealthSystem, Evanston, Illinois. 1 Leonardo Vargas 2 Division of Pulmonary and Critical Care Medicine, NorthShore University HealthSystem, Evanston, Illinois. Tomasz J. Kuzniar2 Disclosure: Nothing to report. Lung toxicity related to interferon (IFN) alpha typically takes a form of interstitial pneumonitis, granulomatous inflammation, or organizing pneumonia. We report a case of a 52-year-old woman, who developed pneumonitis with exudative, lymphocytic-predominant pleural effusion following treatment with pegylated IFN alpha and ribavirin for hepatitis C. Her symptoms and lung findings resolved over 3 months of observation without corticosteroid therapy. Journal of Hospital Medicine 2009;4:E45–E46. VC 2009 Society of Hospital Medicine. KEYWORDS: hepatitis C, interferon alpha, lung toxicity, pleural effusion, ribavirin. Case Report There were no atypical or malignant cells. Bacterial, fungal, A 52-year-old woman with chronic hepatitis C was admitted viral, acid-fast stains and cultures, and polymerase chain with complaints of dry cough, shortness of breath, and reaction (PCR) for Mycobacterium tuberculosis were all neg- fever. Four days prior to admission, she had successfully fin- ative. An echocardiogram and plasma B-type natriuretic ished a 44-week course of pegylated interferon (IFN) alpha peptide were normal. and ribavirin with undetectable viral load on completion of Serum antinuclear and antineutrophilic cytoplasmic anti- treatment. At 30 weeks, she had developed a dry cough, bodies, Bordetella pertussis PCR, serologies for Mycoplasma, which she initially ignored. Three weeks later, as a result of Chlamydia, Coxiella, and urinary antigens for Legionella and a violent coughing episode, she sustained a spontaneous Blastomyces were all negative. -

COVID-19 Pneumonitis and Cystic Lung Disease, Pneumothorax And
Images in Thorax COVID-19 pneumonitis and cystic lung disease, Thorax: first published as 10.1136/thoraxjnl-2021-217390 on 8 July 2021. Downloaded from pneumothorax and pneumomediastinum Serenydd Everden,1 Irfan Zaki,1 Gareth Trevelyan,1 James Briggs2 1Department of Respiratory CASE PRESENTATION Medicine, Royal Berkshire NHS A- 57- year old man with no medical history and Foundation Trust, Reading, UK 2Department of Radiology, Royal <5 pack-year smoking history presented with Berkshire NHS Foundation Trust, dyspnoea. Presentation was 4 days (day 13 from Reading, UK first presentation) post a 9- day admission with COVID-19 pneumonitis (SARS- CoV-2 PCR Correspondence to positive day 0) treated with nasal cannula oxygen Dr Serenydd Everden, and 9 days of dexamethasone. Repeat CXR (day Department of Respiratory Medicine, Royal Berkshire NHS 13) was unchanged and there was no biochemical Foundation Trust, Reading RG1 evidence of bacterial infection. A CT pulmonary 5AN, UK; angiogram (day 13) showed extensive bilateral serenydd. everden@ googlemail. predominantly peripheral subpleural cystic areas com of consolidation, with admixed ground glass changes consistent with COVID-19 pneumo- Received 5 May 2021 Accepted 24 June 2021 nitis (figure 1A). He remained stable and was discharged. He re- presented on day 15 with dyspnoea, oxygen saturations of 83% and left- sided pleu- ritic chest pain. Chest X- ray confirmed left- sided tension pneumothorax, chest drain was inserted, Figure 2 Day 18 CT Thorax: left side pneumothorax, and he improved over 48 hours. Subsequently, pneumomediastinum and subcutaneous emphysema. he deteriorated with pain and swelling around chest and neck. CT Thorax (day 18) showed pneumomediastinum (figure 2) and increased monoxide transfer coefficient (KCO) 0.99 (71% size of the already formed cysts, which were predicted). -

COVID-19 Vaccine-Related Interstitial Lung Disease: a Case Study
Case based discussion COVID-19 vaccine- related interstitial lung disease: a Thorax: first published as 10.1136/thoraxjnl-2021-217609 on 6 August 2021. Downloaded from case study Ji Young Park ,1 Joo- Hee Kim ,1 In Jae Lee,2 Hwan Il Kim,1 Sunghoon Park,1 Yong Il Hwang,1 Seung Hun Jang,1 Ki- Suck Jung1 1Division of Pulmonary, Allergy DR JI YOUNG PARK aspartate aminotransferase, 18 IU/L; and alanine and Critical Care Medicine, Herd immunity through extensive and rapid vaccina- aminotransferase, 11 IU/L. Chest radiograph revealed Department of Internal bilateral reticular opacities. Empirical antibiotics Medicine, Hallym University tion rather than natural immunity acquired by infec- Sacred Heart Hospital, Hallym tion is necessary to control a global pandemic like were administered for 3 days considering a diagnosis University College of Medicine, COVID-19. The development of COVID-19 vaccines of pneumonia; however, the symptoms and chest Anyang, South Korea radiograph findings worsened. Chest CT revealed 2 has been accelerated through government funding Department of Radiology, and the collaborative efforts of the medical–scien- bilateral diffuse ground- glass opacities (GGO) with Hallym University College of 1 2 Medicine, Anyang, South Korea tific institutions and the pharmaceutical industry. focal consolidations, centrilobular micronodules In South Korea, the ChAdOx1 nCoV-19 (Oxford/ and interlobular septal thickening (figure 1A,B). The Correspondence to AstraZeneca) and BNT162b2 (Pfizer/BioNTech) C reactive protein level increased to 11.43 mg/dL. Dr Ji Young Park, Division of vaccines have received emergency approval and are The brain natriuretic peptide level (88 pg/mL) was Pulmonary, Allergy and Critical being used. -

Hypersensitivity Pneumonitis and Pulmonary Hypertension: How the Breeze Affects the Squeeze
EDITORIAL | PULMONARY VASCULAR DISEASES Hypersensitivity pneumonitis and pulmonary hypertension: how the breeze affects the squeeze Steven D. Nathan Affiliations: Advanced Lung Disease and Transplant Program, Dept of Medicine, Inova Fairfax Hospital, Falls Church, VA, USA. Correspondence: Steven D. Nathan, Advanced Lung Disease and Transplant Program, Dept of Medicine, Inova Fairfax Hospital, 3300 Gallows Road, Falls Church, VA 22042, USA. E-mail: [email protected] @ERSpublications Chronic hypersensitivity pneumonitis is commonly complicated by PH, which results in increased functional limitation http://ow.ly/vGBOS The current World Health Organization (WHO) classification of pulmonary hypertension (PH) categorises PH due to chronic lung disease under group 3 [1]. There are many reports of PH complicating the course of the more common interstitial lung diseases (ILD), such as idiopathic pulmonary fibrosis (IPF), connective tissue disease associated-ILDandconditionswithinWHOgroup5,suchassarcoidosis.Whatissurprisingthoughistherelative paucity of data on PH complicating the course of other forms of ILD. The study in this issue of the European Respiratory Journal by OLIVEIRA et al. [2] is the largest to date of right heart catheterisation (RHC) documented PH associated with chronic hypersensitivity pneumonitis (CHP). The authors documented the presence of PH in 50% of their cohort, most of whom (22 out of 25) had group 3 PH, with the three remaining patients having evidence of group 2PH.SimilarlytoIPF,theyfoundthatthepresenceofPH was associated with worse functional impairment [3]. This study raised a number of important issues. The first point of interest does not pertain to PH, but rather the broad spectrum of ILD. Specifically, the authors evaluated 1023 consecutive patients with ILD, of whom 95 were documented to have CHP. -

A False Alarm of COVID-19 Pneumonia in Lung Cancer
Dai et al. J Med Case Reports (2021) 15:41 https://doi.org/10.1186/s13256-020-02619-y CASE REPORT Open Access A false alarm of COVID-19 pneumonia in lung cancer with anti-PD-1 related pneumonitis: a case report and review of the literature Ying Dai, Sha Liu, Yiruo Zhang, Xiaoqiu Li, Zhiyan Zhao, Pingping Liu† and Yingying Du*† Abstract Background: Pneumonitis belongs to the fatal toxicities of anti-PD-1/PD-L1 treatments. Its diagnosis is based on immunotherapeutic histories, clinical symptoms, and the computed tomography (CT) imaging. The radiological fea- tures were typically ground-glass opacities, similar to CT presentation of 2019 Novel Coronavirus (COVID-19) pneumo- nia. Thus, clinicians are cautious in diferential diagnosis especially in COVID-19 epidemic areas. Case presentation: Herein, we report a 67-year-old Han Chinese male patient presenting with dyspnea and nor- mal body temperature on the 15th day of close contact with his son, who returned from Wuhan. He was diagnosed as advanced non-small cell lung cancer and developed pneumonitis post Sintilimab injection during COIVD-19 pandemic period. The chest CT indicated peripherally subpleural lattice opacities at the inferior right lung lobe and bilateral thoracic efusion. The swab samples were taken twice within 72 hours and real-time reverse-transcription polymerase-chain-reaction (RT-PCR) results were COVID-19 negative. The patient was thereafter treated with pred- nisolone and antibiotics for over 2 weeks. The suspicious lesion has almost absorbed according to CT imaging, consistent with prominently falling CRP level. The anti-PD-1 related pneumonitis mixed with bacterial infection was clinically diagnosed based on the laboratory and radiological evidences and good response to the prednisolone and antibiotics. -

Pulmonary Disorders, Including Vocal Cord Dysfunction
Pulmonary disorders, including vocal cord dysfunction Paul A. Greenberger, MD, and Leslie C. Grammer, MD Chicago, Ill The lung is a very complex immunologic organ and responds in a variety of ways to inhaled antigens, organic or inorganic Abbreviations used materials, infectious or saprophytic agents, fumes, and irritants. ABPA: Allergic bronchopulmonary aspergillosis There might be airways obstruction, restriction, neither, or both ANCA: Antineutrophil cytoplasmic antibody accompanied by inflammatory destruction of the pulmonary ARDS: Acute respiratory distress syndrome BAL: Bronchoalveolar lavage interstitium, alveoli, or bronchioles. This review focuses on COPD: Chronic obstructive pulmonary disease diseases organized by their predominant immunologic CSS: Churg-Strauss syndrome responses, either innate or acquired. Pulmonary innate immune CT: Computed tomography conditions include transfusion-related acute lung injury, World FVC: Forced vital capacity Trade Center cough, and acute respiratory distress syndrome. HDAC: Histone deacetylase Adaptive immunity responses involve the systemic and mucosal LT: Leukotriene immune systems, activated lymphocytes, cytokines, and PMN: Polymorphonuclear leukocyte 1 antibodies that produce CD4 TH1 phenotypes, such as for RADS: Reactive airways dysfunction syndrome tuberculosis or acute forms of hypersensitivity pneumonitis, and TLR: Toll-like receptor 1 TRALI: Transfusion-related acute lung injury CD4 TH2 phenotypes, such as for asthma, Churg-Strauss VCD: Vocal cord dysfunction syndrome, and allergic