Glenmark Receives Approval for Combination of Remogliflozin Etabonate and Metformin Hydrochloride for Adults with Type 2 Diabetes in India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment of Diabetes Mellitus
TREATMENT OF DIABETES MELLITUS DIABETES is a condition that affects how the body makes energy from food. Food is broken down into sugar (glucose) in the body and released into the blood. When the blood sugar level rises after a meal, insulin responds to let the sugar into the cells to be used as energy. In diabetes, the body either does not make enough insulin or it stops responding to insulin as well as it should. This results in sugar staying in the blood and leads to serious health problems over time. DIAGNOSIS OF DIABETES1 • A1C Test: Lab test measuring average blood sugar over past two to three months • Fasting Blood Sugar Test: Lab test measuring blood sugar after eight hours of no food or drink • Oral Glucose Tolerance Test (OGTT): Measures blood sugar before and two hours after drinking a specific sugary liquid • Random Blood Sugar Test: Measures blood sugar at a moment in time, without any kind of preparation (like fasting) FASTING BLOOD ORAL GLUCOSE TOLERANCE RANDOM BLOOD RESULT A1C TEST SUGAR TEST TEST SUGAR TEST Diabetes ≥ 6.5% ≥126 mg/dL ≥ 200 mg/dL ≥ 200 mg/dL Prediabetes 5.7 – 6.4% 100 – 125 mg/dL 140 – 199 mg/dL N/A Normal < 5.7% ≤99 mg/dL < 140 mg/dL N/A NON-DRUG TREATMENTS2 THERAPY COST WHAT TO EXPECT Diet (Mediterranean diet) and exercise (30 minutes a day, five days a week of moderate- Weight loss $-$$ intensity exercise); 7% weight loss decreases risk of diabetes3 Psychological intervention $$-$$$ Psychotherapy may reduce diabetic distress and improve glycemic control4,5 nationalcooperativerx.com PRESCRIPTION TREATMENTS -

Dapagliflozin – Structure, Synthesis, and New Indications
Pharmacia 68(3): 591–596 DOI 10.3897/pharmacia.68.e70626 Review Article Dapagliflozin – structure, synthesis, and new indications Stefan Balkanski1 1 Bulgarian Pharmaceutical Union, Sofia, Bulgaria Corresponding author: Stefan Balkanski ([email protected]) Received 24 June 2021 ♦ Accepted 4 July 2021 ♦ Published 4 August 2021 Citation: Balkanski S (2021) Dapagliflozin – structure, synthesis, and new indications. Pharmacia 68(3): 591–596.https://doi. org/10.3897/pharmacia.68.e70626 Abstract Dapagliflozin is a sodium-glucose co-transporter-2 (SGLT2) inhibitors used in the treatment of patients with type 2 diabetes. An aryl glycoside with significant effect as glucose-lowering agents, Dapagliflozin also has indication for patients with Heart Failure and Chronic Kidney Disease. This review examines the structure, synthesis, analysis, structure activity relationship and uses of the prod- uct. The studies behind this drug have opened the doors for the new line of treatment – a drug that reduces blood glucoses, decreases the rate of heart failures, and has a positive effect on patients with chronic kidney disease. Keywords Dapagliflozin, SGLT2-inhibitor, diabetes, heart failure Structure of dapagliflozin against diabetes (Lee et al. 2005; Lemaire 2012; Mironova et al. 2017). Embodiments of (SGLT-2) inhibitors include C-glycosides have a remarkable rank in medicinal chemis- dapagliflozin, canagliflozin, empagliflozin and ipragliflozin, try as they are considered as universal natural products shown in Figure 1. It has molecular formula of C24H35ClO9. (Qinpei and Simon 2004). Selective sodium-dependent IUPAC name (2S,3R,4R,5S,6R)-2-[4-chloro-3-[(4- glucose cotransporter 2 (SGLT-2) inhibitors are potent ethoxyphenyl)methyl]phenyl]-6-(hydroxymethyl)oxa- medicinal candidates of aryl glycosides that are functional ne-3,4,5-triol;(2S)-propane-1,2-diol;hydrate. -

CDR Clinical Review Report for Soliqua
CADTH COMMON DRUG REVIEW Clinical Review Report Insulin glargine and lixisenatide injection (Soliqua) (Sanofi-Aventis) Indication: adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus inadequately controlled on basal insulin (less than 60 units daily) alone or in combination with metformin. Service Line: CADTH Common Drug Review Version: Final (with redactions) Publication Date: January 2019 Report Length: 118 Pages Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services. While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. -

Download Product Insert (PDF)
PRODUCT INFORMATION Remogliflozin A Item No. 14340 CAS Registry No.: 329045-45-6 OH Formal Name: 5-methyl-4-[[4-(1-methylethoxy) N O OH phenyl]methyl]-1-(1-methylethyl)- N 1H-pyrazol-3-yl β-D- O glucopyranoside OH Synonym: GSK189074 OH MF: C23H34N2O7 FW: 450.5 Purity: ≥98% λ: 229 nm UV/Vis.: max O Supplied as: A crystalline solid Storage: -20°C Stability: ≥2 years Information represents the product specifications. Batch specific analytical results are provided on each certificate of analysis. Laboratory Procedures Remogliflozin A is supplied as a crystalline solid. A stock solution may be made by dissolving the remogliflozin A in the solvent of choice. Remogliflozin A is soluble in organic solvents such as ethanol, DMSO, and dimethyl formamide, which should be purged with an inert gas. The solubility of remogliflozin A in these solvents is approximately 30 mg/ml. Remogliflozin A is sparingly soluble in aqueous buffers. For maximum solubility in aqueous buffers, remogliflozin A should first be dissolved in ethanol and then diluted with the aqueous buffer of choice. Remogliflozin A has a solubility of approximately 0.5 mg/ml in a 1:1 solution of ethanol:PBS (pH 7.2) using this method. We do not recommend storing the aqueous solution for more than one day. Description Remogliflozin A is a potent inhibitor of sodium-glucose transporter 2 (SGLT2; Kis = 12.4 and 26 nM 1 for human and rat SGLT2, respectively). It is selective for SGLT2 over SGLT1 (Kis = 4,520 and 997 nM for human and rat SGLT1, respectively). Following administration of a prodrug, remogliflozin etabonate, that is rapidly converted to remogliflozin A in vivo, rat urinary glucose excretion increases and plasma glucose and insulin concentrations decrease. -

Qtern (Dapagliflozin/Saxagliptin) – New Drug Approval
Qtern® (dapagliflozin/saxagliptin) – New drug approval • On February 28, 2017, AstraZeneca announced the FDA approval of Qtern (dapagliflozin/saxagliptin) as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus (T2DM) who have inadequate control with Farxiga® (dapagliflozin) or who are already treated with dapagliflozin and Onglyza® (saxagliptin). • Qtern is not indicated for the treatment of type 1 diabetes mellitus or diabetic ketoacidosis, and it should only be used in patients who tolerate 10 mg of dapagliflozin. • Qtern combines two anti-hyperglycemic agents, dapagliflozin, a sodium-glucose co-transporter 2 (SGLT-2) inhibitor, and saxagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor. • The efficacy of Qtern was evaluated in a study of 315 T2DM patients. Patients were randomized to saxagliptin or placebo, in combination with dapagliflozin and metformin. — Patients treated with add-on saxagliptin therapy had significantly greater reductions in HbA1c from baseline vs. the placebo group (-0.5% vs. -0.2%, respectively; difference between groups in HbA1c: -0.4%, p < 0.0001). — The proportion of patients achieving HbA1c < 7% at week 24 was 35.3% in the saxagliptin group vs. 23.1% in the placebo group. • Qtern is contraindicated in patients with a history of a serious hypersensitivity reaction to dapagliflozin or to saxagliptin (eg, anaphylaxis, angioedema or exfoliative skin conditions), and in patients with moderate to severe renal impairment (eGFR < 45 mL/min/1.73 m2), end-stage renal disease, or on dialysis. • Warnings and precautions of Qtern include pancreatitis, heart failure, hypotension, ketoacidosis, acute kidney injury and impairment in renal function, urosepsis and pyelonephritis, hypoglycemia with concomitant use of insulin or insulin secretagogues, genital mycotic infections, increases in low- density lipoprotein cholesterol, bladder cancer, severe and disabling arthralgia, and bullous pemphigoid. -

Remogliflozin Etabonate, a Selective Inhibitor of the Sodium-Glucose
Clinical Care/Education/Nutrition/Psychosocial Research BRIEF REPORT Remogliflozin Etabonate, a Selective Inhibitor of the Sodium-Glucose Transporter 2, Improves Serum Glucose Profiles in Type 1 Diabetes 1,2 3 SUNDER MUDALIAR, MD JUNE YE, PHD placebo (placebo), 2) mealtime insulin 1 3 DEBRA A. ARMSTRONG, BA, RN, CCRC ELIZABETH K. HUSSEY, PHARMD 2 3 injection + RE placebo (prandial insulin), ANNIE A. MAVIAN, MD DEREK J. NUNEZ, MD 3 3 1,2 ) placebo insulin injection + 50 mg RE (RE ROBIN O’CONNOR-SEMMES, PHD ROBERT R. HENRY, MD 3 3 50 mg), 4) placebo insulin injection + 150 PATRICIA K. MYDLOW, BS ROBERT L. DOBBINS, MD, PHD mg RE (RE 150 mg), and 5) placebo insulin injection + 500 mg RE (RE 500 mg). d fl Each individual received 75-g oral OBJECTIVES Remogli ozin etabonate (RE), an inhibitor of the sodium-glucose transporter glucose and identical meals during all 2, improves glucose profiles in type 2 diabetes. This study assessed safety, tolerability, pharma- cokinetics, and pharmacodynamics of RE in subjects with type 1 diabetes. treatment periods. Frequent samples were obtained for measurement of plasma RESEARCH DESIGN AND METHODSdTen subjects managed with continuous sub- glucose and insulin concentrations. Urine cutaneous insulin infusion were enrolled. In addition to basal insulin, subjects received five samples were collected for 24 h to assess randomized treatments: placebo, prandial insulin, 50 mg RE, 150 mg RE, and mg RE 500. creatinine clearance and glucose excre- d tion. Plasma samples were collected for RESULTS Adverse events and incidence of hypoglycemia with RE did not differ from placebo fl and prandial insulin groups. -

202293Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 202293Orig1s000 RISK ASSESSMENT and RISK MITIGATION REVIEW(S) Department of Health and Human Services Public Health Service Food and Drug Administration Center for Drug Evaluation and Research Office of Surveillance and Epidemiology Office of Medication Error Prevention and Risk Management Final Risk Evaluation and Mitigation Strategy (REMS) Review Date: December 20, 2013 Reviewer(s): Amarilys Vega, M.D., M.P.H, Medical Officer Division of Risk Management (DRISK) Team Leader: Cynthia LaCivita, Pharm.D., Team Leader DRISK Drug Name(s): Dapagliflozin Therapeutic Class: Antihyperglycemic, SGLT2 Inhibitor Dosage and Route: 5 mg or 10 mg, oral tablet Application Type/Number: NDA 202293 Submission Number: Original, July 11, 2013; Sequence Number 0095 Applicant/sponsor: Bristol-Myers Squibb and AstraZeneca OSE RCM #: 2013-1639 and 2013-1637 *** This document contains proprietary and confidential information that should not be released to the public. *** Reference ID: 3426343 1 INTRODUCTION This review documents DRISK’s evaluation of the need for a risk evaluation and mitigation strategy (REMS) for dapagliflozin (NDA 202293). The proposed proprietary name is Forxiga. Bristol-Myers Squibb and AstraZeneca (BMS/AZ) are seeking approval for dapagliflozin as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus (T2DM). Bristol-Myers Squibb and AstraZeneca did not submit a REMS or risk management plan (RMP) with this application. At the time this review was completed, FDA’s review of this application was still ongoing. 1.1 BACKGROUND Dapagliflozin. Dapagliflozin is a potent, selective, and reversible inhibitor of the human renal sodium glucose cotransporter 2 (SGLT2), the major transporter responsible for renal glucose reabsorption. -

Real-Life Prescribing of SGLT2 Inhibitors: How to Handle the Other Medications, Including
Kidney360 Publish Ahead of Print, published on February 1, 2021 as doi:10.34067/KID.0000412021 Real-life prescribing of SGLT2 inhibitors: How to handle the other medications, including glucose-lowering drugs and diuretics David Lam1 and Aisha Shaikh1,2 1Icahn School of Medicine at Mount Sinai, Dept. of Medicine, New York, NY 2James J. Peters VA Medical Center, Dept. of Medicine, Bronx, NY Corresponding Author: Aisha Shaikh, MD James J. Peters VA Medical Center 130 w. Kingsbridge Road Bronx, NY – 10468 Email: [email protected] Phone: 718-584-9000, Ext# 6630 Copyright 2021 by American Society of Nephrology. Introduction Sodium-glucose cotransporter-2 inhibitors (SGLT2is) have emerged as an effective therapy for improving outcomes in diabetic and non-diabetic kidney disease (1, 2). Clinical trials have demonstrated the benefits of SGLT2is for secondary prevention of adverse cardiovascular (CV) effects in patients with established atherosclerotic disease and/or heart failure with reduced ejection fraction (3-7). It is imperative for clinicians to assess the use of SGLT2is in medically eligible patients and prescribe these agents when appropriate. Despite the overwhelming evidence of the benefits of SGLT2i therapy, the prescription rate remains dismally low particularly among patients most likely to benefit from cardiorenal protective effects (8). Several potential factors contribute to low SGLT2i prescription rate including prescriber hesitancy, treatment inertia and high drug cost. In this article, we review clinical indications for SGLT2i use, therapeutic and adverse effects, and our approach to handling concomitant medications. Clinical indications for SGLT2i Use 1. Type 2 diabetes mellitus (T2DM) and albuminuric kidney disease (albuminuria of ≥ 200 mg/gram of creatinine plus eGFR of 25 – 90 ml/min/1.73 m2). -
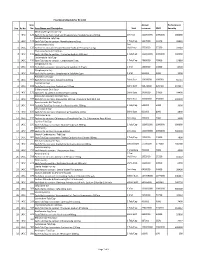
Sno. Rc No Item No. Item Name and Description Unit Annual Turnover
Final Drug Schedule for RC 145C Item Annual Performance Sno. Rc No No. Item Name and Description Unit turnover EMD Security Medroxy Progesterone Inj- 1 145C 126 Each ml to contain: Medroxy Progesterone Acetate Suspn.150mg. 1ml Vial 100000000 1000000 600000 Norethisterone Tab/Cap- 2 145C 128 Each Tab/Cap to contain: Norethisterone 5mg. 1 Tab/Cap 5637000 56370 33822 Dexamethasone Inj- 2ml 3 145C 133 Each ml to contain: Dexamethasone Sodium Phosphate 4 mg. Vial/Amp 5735000 57350 34410 Thyroxine Sodium Tab/Cap- 4 145C 135 Each Tab/Cap to contain: Thyroxine Sodium 100 mcg 1 Tab/Cap 100000000 1000000 600000 Carbimazole Tab/Cap- 5 145C 136 Each Tab/Cap to contain: Carbimazole 5 mg. 1 Tab/Cap 2980000 29800 17880 Streptomycin Inj- 6 145C 151 Each Vial to contain: Streptomycin Sulphate 0.75gm 1 Vial 1400000 14000 8400 Streptomycin Inj- 7 145C 152 Each Vial to contain: Streptomycin Sulphate 1gm 1 Vial 500000 5000 3000 Ampicillin Dry Syp- 8 145C 161 Each 5ml to contain: Ampicillin 125mg 30ml Bott 10959000 109590 65754 Cephalexin Syp- 9 145C 168 Each 5ml to contain: Cephalexin 125mg 30ml Bott 32874000 328740 197244 Erthyromycin Oral Susp- 10 145C 172 Each 5ml to contain: Erythromycin 125mg 30ml Bott 2400000 24000 14400 Amoxy & Clavulanic Acid Dry Syp- 11 145C 183 Each 5ml to contain: Amoxycillin 200 mg, Clavulanic Acid 28.5 mg 30ml Bott 35000000 350000 210000 Pyrazinamide Kid Tab/Cap- 12 145C 191 Each Kid Tab/Cap to contain: Pyrazinamide 300mg 1 Tab/Cap 500000 5000 3000 Chloroquine Syp- 13 145C 196 Each 5ml to contain: Chloroquine Phosphate 50mg. -

SGLT2) Inhibitors (Gliflozins) in Adults with Type 2 Diabetes (T2DM
Sodium-glucose cotransporter-2 (SGLT2) inhibitors (Gliflozins) in Adults with Type 2 Diabetes (T2DM) There are currently four SGLT2 inhibitors (canagliflozin, dapagliflozin, empagliflozin and ertugliflozin) licensed in the UK for the management of adults with T2DM. No head to head trials between the SGLT2 inhibitors have been conducted. As at December 2019, clinical outcome data is available for three of the four SGLT2 inhibitors around their cardiovascular effects in people with T2DM. Ertugliflozin is still to report on this data. This document summarises the key prescribing considerations. NICE Technology Appraisal Recommendation NICE makes recommendations for when SGLT2 inhibitors can be considered in adults with T2DM; Hertfordshire Medicines Management Committee Recommendations are in line with NICE guidance: Monotherapy NICE TA 390: Canagliflozin, Dapagliflozin and Empagliflozin and NICE TA 572: Ertugliflozin as monotherapies for treating T2DM Monotherapy recommended as option in adults for whom metformin is contraindicated or not tolerated and when diet & exercise alone do not provide adequate glycaemic control, only if: •a DPP‑4 inhibitor would otherwise be prescribed and •a sulfonylurea or pioglitazone is not appropriate. Dual therapy NICE TA 315: Canagliflozin, NICE TA288: Dapagliflozin, TA 336: Empagliflozin, TA 572: Ertugliflozin as combination therapies for treating T2DM In a dual therapy regimen in combination with metformin is recommended as an option, only if: •a sulfonylurea is contraindicated or not tolerated or •the person is at significant risk of hypoglycaemia or its consequences. In combination with insulin NICE TA 315: Canagliflozin, NICE TA288: Dapagliflozin, TA 336: Empagliflozin in combination with insulin with or without other antidiabetic drugs is recommended as an option. -

Exploring Glycosuria As a Mechanism for Weight and Fat Mass Reduction. a Pilot Study with Remogliflozin Etabonate and Sergliflozin Etabonate in Healthy Obese Subjects
Journal of Clinical & Translational Endocrinology 1 (2014) e3ee8 Contents lists available at ScienceDirect Journal of Clinical & Translational Endocrinology journal homepage: www.elsevier.com/locate/jcte Research Paper Exploring glycosuria as a mechanism for weight and fat mass reduction. A pilot study with remogliflozin etabonate and sergliflozin etabonate in healthy obese subjects Antonella Napolitano a,*, Sam Miller a, Peter R. Murgatroyd c, Elizabeth Hussey b, Robert L. Dobbins b, Edward T. Bullmore a, Derek J.R. Nunez b View metadata, citation and similar papers at core.ac.uk brought to you by CORE a Clinical Unit in Cambridge, GlaxoSmithKline, Addenbrookes Hospital, Cambridge, UK b Metabolic Pathways and Cardiovascular Unit, GlaxoSmithKline,provided by NC, Elsevier USA - Publisher Connector c Wellcome Trust Clinical Research Facility, Cambridge University Hospital NHS Trust, UK article info abstract Article history: Inhibitors of sodium-dependent glucose co-transporter 2 (SGLT2) increase glucose excretion in the urine Received 16 October 2013 and improve blood glucose in Type 2 diabetes mellitus. Glycosuria provides an energy and osmotic drain Received in revised form that could alter body composition. We therefore conducted a pilot study comparing the effects on body 26 November 2013 composition of two SGLT2 inhibitors, remogliflozin etabonate (RE) 250 mg TID (n ¼ 9) and sergliflozin Accepted 5 December 2013 etabonate (SE) (1000 mg TID) (n ¼ 9), with placebo (n ¼ 12) in obese non-diabetic subjects. Both drugs Available online 7 February 2014 were well tolerated during 8 weeks of dosing, and the most common adverse event was headache. No urinary tract infections were observed, but there was one case of vaginal candidiasis in the RE group. -

(SGLT2) Inhibitors Reference Number: HIM.PA.91 Effective Date: 01.01.15 Last Review Date: 02.20 Line of Business: HIM Revision Log
Clinical Policy: Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitors Reference Number: HIM.PA.91 Effective Date: 01.01.15 Last Review Date: 02.20 Line of Business: HIM Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description The following agents contain a sodium-glucose co-transporter 2 (SGLT2) inhibitor and require prior authorization: canagliflozin (Invokana®), canagliflozin/metformin (Invokamet®), dapagliflozin (Farxiga®), dapagliflozin/metformin (Xigduo® XR), empagliflozin (Jardiance®), empagliflozin/linagliptin (Glyxambi®), empagliflozin/linagliptin/metformin (TrijardyTM XR), and empagliflozin/metformin (Synjardy®). FDA Approved Indication(s) SGLT2 inhibitors are indicated as adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. Dapagliflozin-, canagliflozin-, and empagliflozin-containing products are also indicated in adult patients with type 2 diabetes mellitus and established cardiovascular disease (or multiple cardiovascular risk factors [dapagliflozin only]) to: Reduce the risk of hospitalization for heart failure (HF) (dapagliflozin) Reduce the risk of major adverse cardiovascular events: cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke (canagliflozin) Reduce the risk of cardiovascular death (empagliflozin) Canagliflozin-containing products are additionally indicated to reduce the risk of end-stage kidney disease, doubling of serum creatinine, cardiovascular death, and hospitalization for HF in adults with type 2 diabetes mellitus and diabetic nephropathy with albuminuria > 300 mg/day. Limitation(s) of use: SGLT2 inhibitors should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis. Policy/Criteria Provider must submit documentation (such as office chart notes, lab results or other clinical information) supporting that member has met all approval criteria.